
Abstract
We present five cases of osteolysis in the Motec total wrist prosthesis, three around the radial implant, one around the metacarpal implant and one around both. Three of these were progressive and required revision, and biomechanical explant analyses of these revised prostheses were performed. Ex vivo testing of the contact points of the Motec implants was also performed at maximum extension. Here, impingement occurs between the metacarpal screw and the dorsal rim of the cup (non-articulating surfaces) with the short-necked prosthesis, leading to metacarpal screw damage, titanium debris formation and osteolysis. An analysis of three previously published cases suggests that this may have been the likely mode of failure in those cases. This complication is preventable by avoiding use of the short-neck prosthesis.
Introduction
The Motec total wrist prosthesis (Swemac Innovation AB, Linkoping, Sweden) was launched in 2006 and has a 10-year survival rate of 86% (Reigstad et al., 2017). It is increasingly used for younger, higher demand patients and has shown good intermediate-term results (Giwa et al., 2018; Reigstad et al., 2017).
It is a modular ball-and-socket design comprising metacarpal and radial conical threaded titanium screws. The head is made from cobalt-chrome (CoCr), and four neck lengths are available. The cup is made from either CoCr or carbon fibre-reinforced polyether ether ketone (PEEK).
Recent publications have described osteolysis in three patients treated with the Motec prosthesis and have postulated that this is related to the release of debris secondary to articular surface wear (Karjalainen et al., 2018; Rothe et al., 2022).
Our hypothesis is that the wear debris is generated from non-articular surfaces when the proximal end of the metacarpal screw strikes the distal edge of the cup during extreme extension, in line with the opinion of Reigstad and Røkkum (2018), the developers of the Motec prosthesis. They stated, ‘We have seen metal rim wear in wrists using the short neck with indentations in the titanium screw due to fretting of the cup and [causing] osteolysis’.
Methods
We retrospectively reviewed prospectively collected data for all primary and revision Motec prostheses in our department and identified osteolysis at the implant–bone interface from routine annual postoperative radiographs. Only cases with at least 2 years of follow-up were included. A stable periprosthetic radiolucent line from physiological stress shielding was not considered osteolysis.
If revision surgery was performed, clinical and operative records and laboratory results, including metal ion levels, histology and microbiology reports, were reviewed.
All surfaces of the explanted components were analysed macroscopically and microscopically and measured using a Quickscope (Mitutoyo, Kawasaki, Japan), a non-contact vision measuring system, at 25× magnification. The articulating surfaces of the heads were examined using a TM3030 (Hitachi, Tokyo, Japan) scanning electron microscope (SEM).
In addition, we evaluated different combinations of Motec implants through a maximum range of motion ex vivo to identify the site of contact between the proximal and distal components.
Results
Three cases of osteolysis were found out of 30 primary Motec prostheses implanted in our department between 2016 and 2020 (cases A, B and C). Two additional cases with osteolysis were referred for revision surgery (cases D and E). Three out of five cases underwent revision surgery (C, D and E).
Of the 30 primary arthroplasties, 20 of the patients were female. The mean age was 64 years (age range 42–86 years). Seven patients had a short-neck prosthesis, and 23 had a medium-neck prosthesis.
Details of the five cases of osteolysis are shown in Table 1. In all five cases, a short-necked head with a diameter of 15 mm was used. There were no cases of osteolysis in any of the patients with medium-neck heads.
Demographics, implant details, osteolysis, blood ions and revision details of cases with osteolysis.
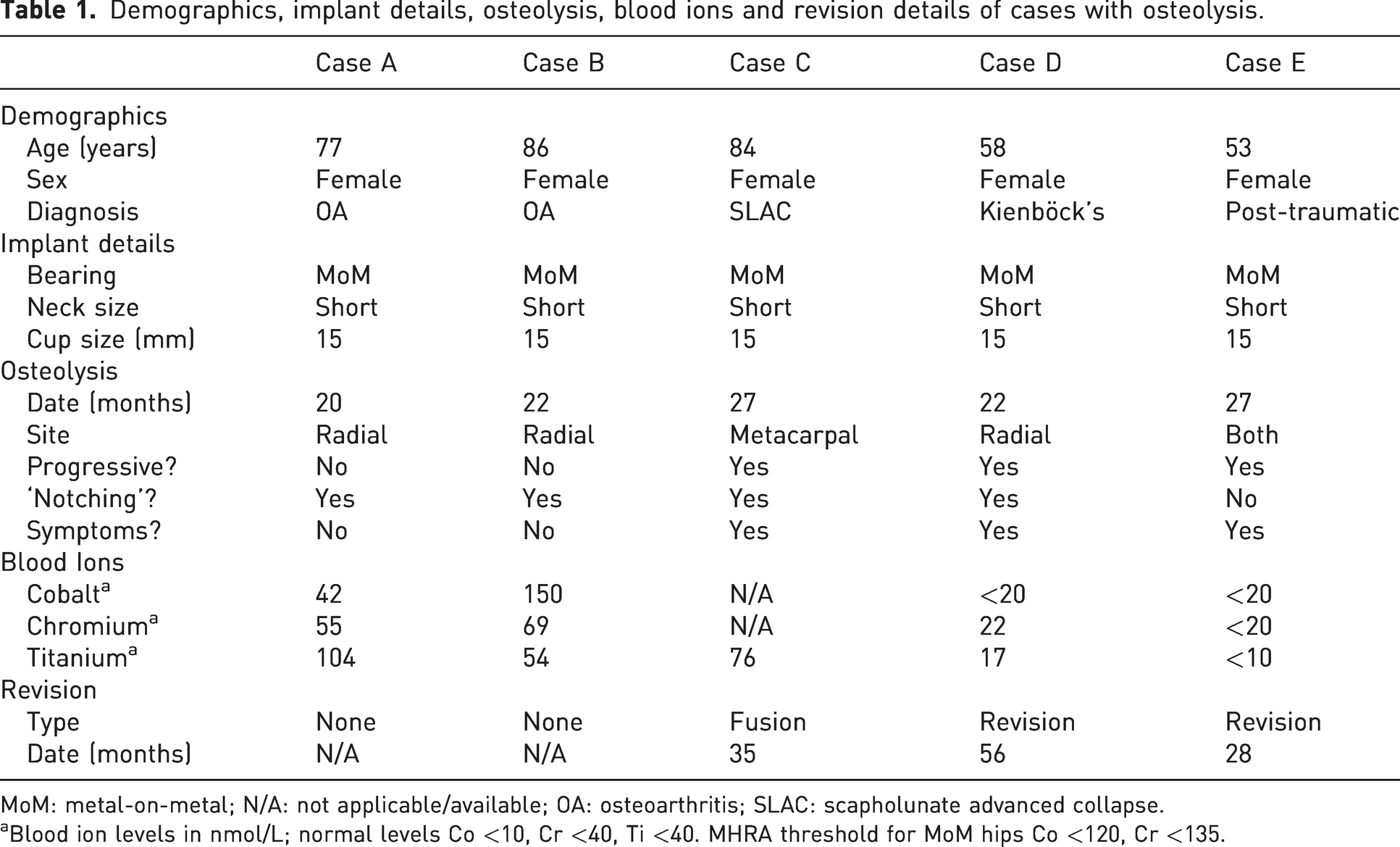
MoM: metal-on-metal; N/A: not applicable/available; OA: osteoarthritis; SLAC: scapholunate advanced collapse.
Blood ion levels in nmol/L; normal levels Co <10, Cr <40, Ti <40. MHRA threshold for MoM hips Co <120, Cr <135.
Postoperative radiographs showed appropriately sized, well-positioned components in all cases. Some degree of osteolysis was present on radiographs before patients became symptomatic. Before revision, radiographs showed marked osteolysis with erosions and resorption around the implants (Figure 1a and 1b). Lateral radiographs in four out of five cases showed obvious damage (‘notching’) to the dorsal aspect of the proximal edge of the metacarpal screw (Figure 1c). This notching was not seen in the other four cases of the primary Motec series where a short-necked head was used but no osteolysis was seen.
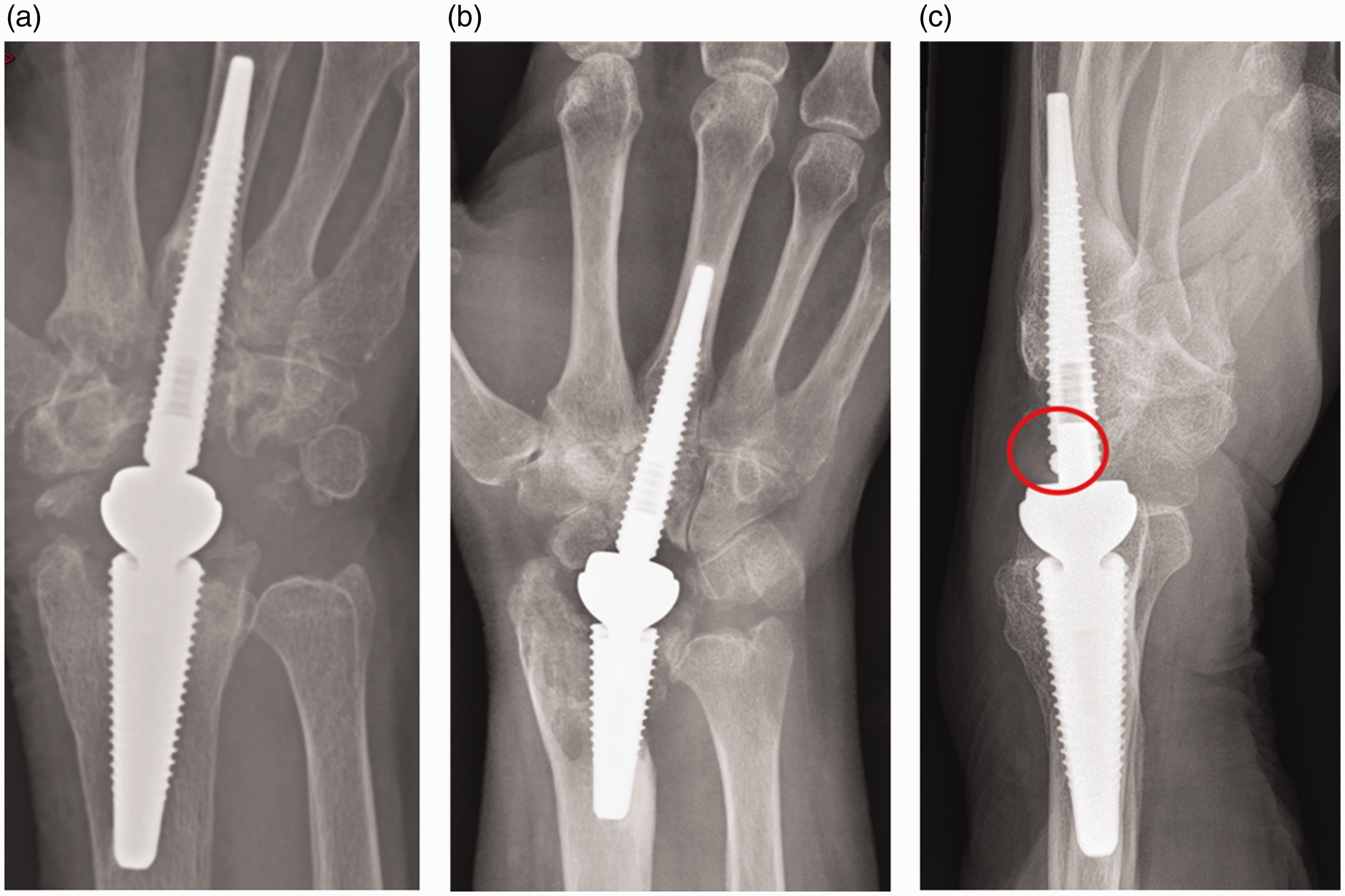
Radiographs showing (a) marked osteolysis around the metacarpal component, (b) the radial component and (c) damage to the metacarpal screw threads (circled).
The blood metal ions of cobalt, chromium and titanium are detailed in Table 1. The elevated cobalt and chromium levels in case B were below the Medicines and Healthcare products Regulatory Agency (MHRA) threshold for closer follow-up and cross-sectional imaging in metal-on-metal (MoM) hip replacements (MHRA 2017). In four out of five cases, titanium levels were significantly elevated.
Case C underwent a two-stage revision to arthrodesis. Case D underwent a two-stage revision to another Motec and case E underwent a single-stage revision of the metacarpal screw and bearing surface components. Intraoperatively, in all cases there was evidence of metallosis with marked black synovitis with green fluid in the joint, similar to the pseudotumours described in MoM hip arthroplasty (Pandit et al., 2008). Macroscopic damage was seen on the dorsal rim of the metacarpal screw in all three cases. Histology in all cases showed a patchy infiltrate of lymphocytes and many macrophages containing small particles of metallic debris. No neutrophils were identified, and no acid-fast bacilli or fungi were found on extended staining.
Infection was excluded in all cases after extended culture of multiple samples.
Explant analysis of the revised prostheses showed evidence of impingement, where the rim of the cup impinged on the metacarpal screw and created a defect in it (Figure 2). When measured microscopically these defects measured up to 1.22 mm wide, 5.01 mm long and 0.50 mm deep, resulting in a loss of 3.03 mm3 Ti alloy from the screw of case C, 0.03 mm3 from case D and 2.79 mm3 from case E. In cases C and E, the area on the rim of the cup where contact with the metacarpal screw occurred appeared relatively darker compared to the rest of the rim. The cup in case D was normal.
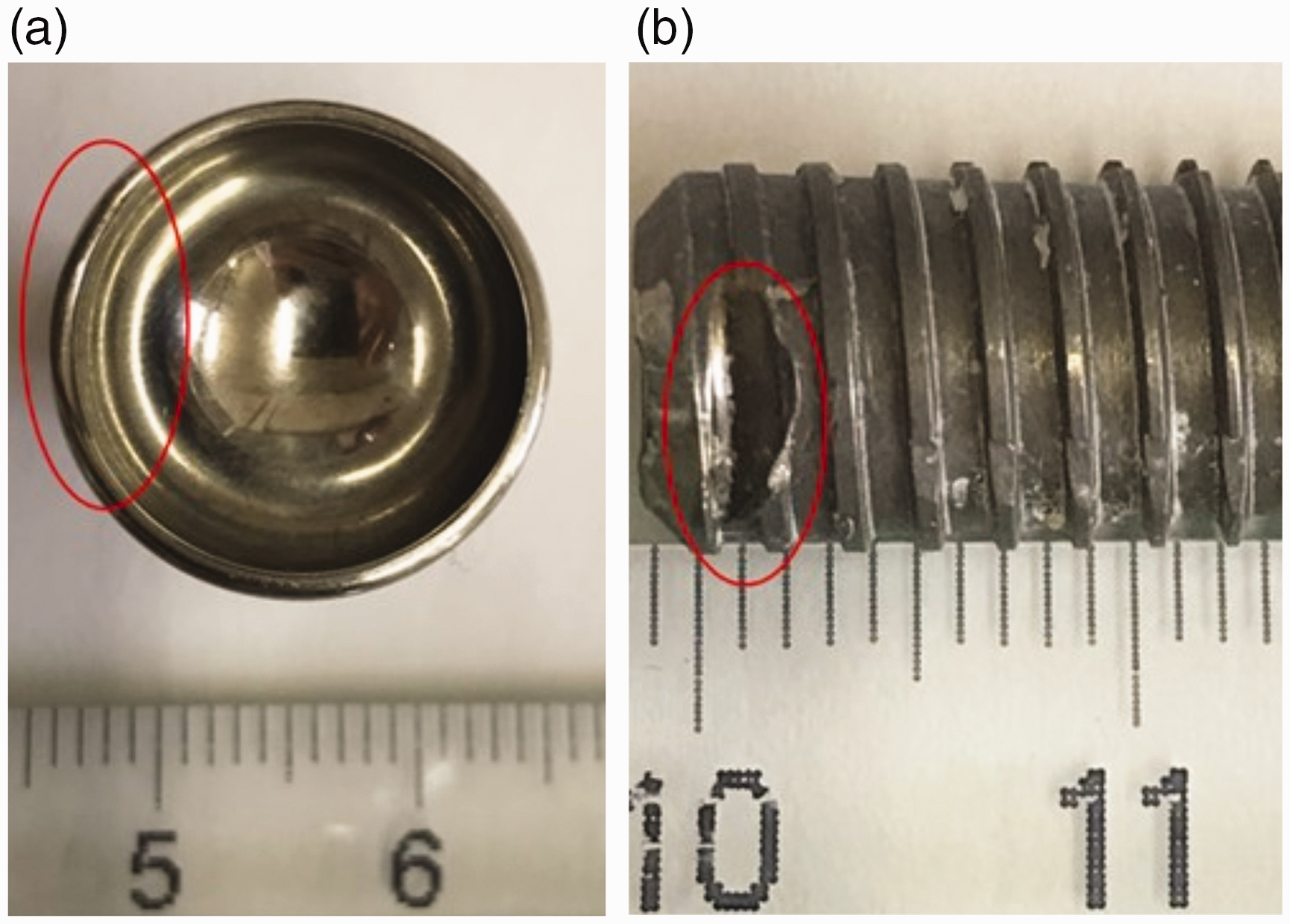
(a) The cup and (b) the proximal end of the metacarpal screw of case C. The damage by impingement of the components, the relatively darker area on the rim and the hole in the metacarpal screw are highlighted by the red ellipses.
The heads showed some dark grey markings on the articular surface (Figure 3a). These marks were not present in case D. SEM analysis identified these marks on the head of explants in cases C (Figure 3b) and E as adherent titanium alloy debris, with a material composition of titanium, aluminium, and vanadium in case C, and titanium and aluminium in case E, consistent with the alloy (Ti6Al4V) of the Motec screws (Reigstad and Røkkum, 2018). Apart from minor superficial scratches, there was no evidence of notable wear on the cups.
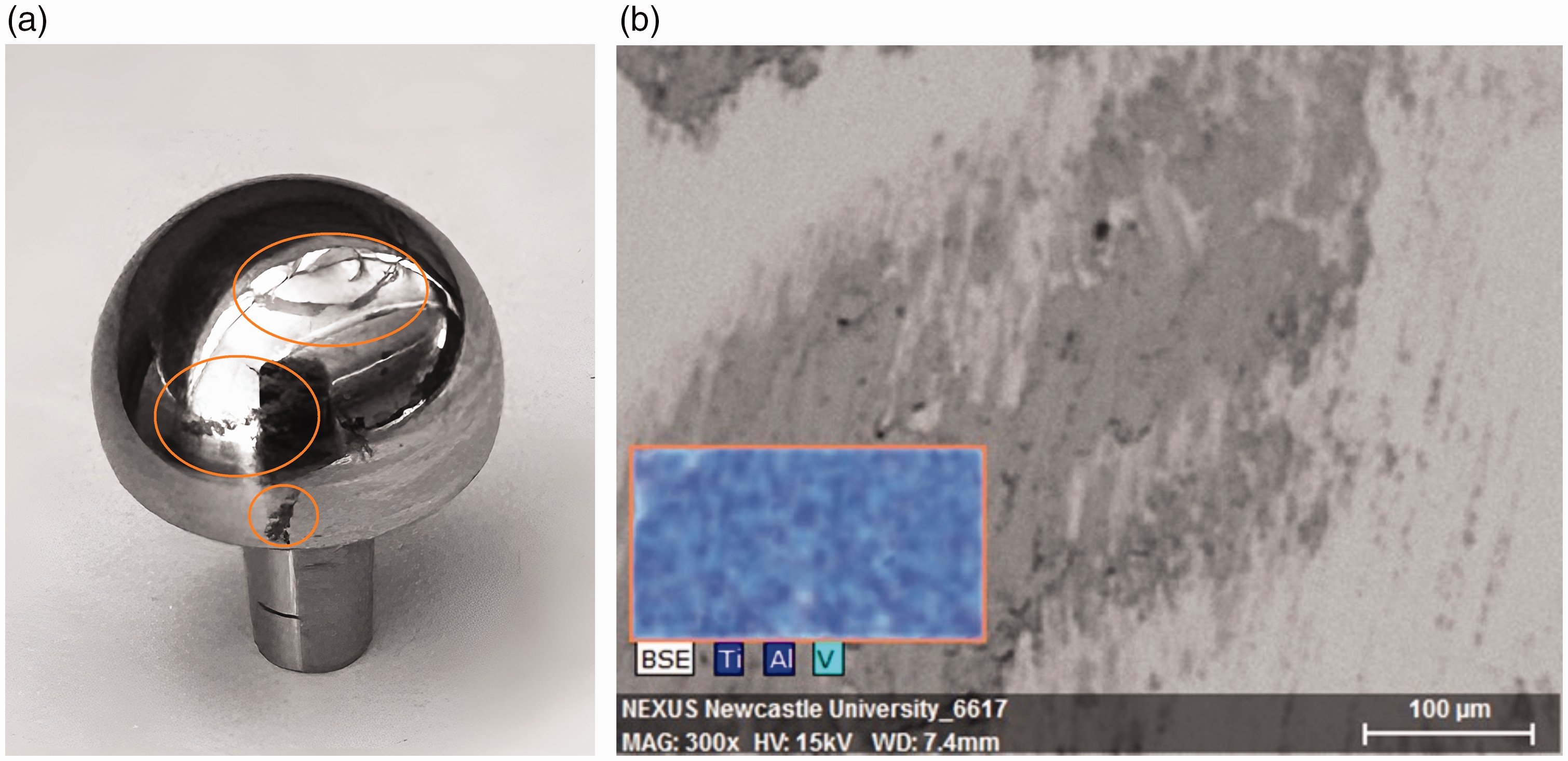
The explanted head of case C. (a) The dark grey marks observed on its articulating surface are highlighted, and (b) an SEM image shows adhered titanium alloy debris. The dark grey marks observed consisted of titanium, aluminium and vanadium.
No damage was observed on the outer surfaces of the radial screws. The necks of the cups were undamaged except for some minor scratches where the neck of the cup was located within the morse taper of the radial screws.
Ex vivo observation of the Motec sample components in maximum flexion-extension over 65° showed that for the short-necked component, the threaded titanium metacarpal component struck either the rim of the CoCr (Figure 4a) or the PEEK cup (Figure 4b). With the medium-, long- and extra-long-necked heads, the smooth CoCr neck hits the CoCr or PEEK cup rim (ROM ≥72°), and there is no contact with the threaded titanium metacarpal screw (Figure 4c and 4d).
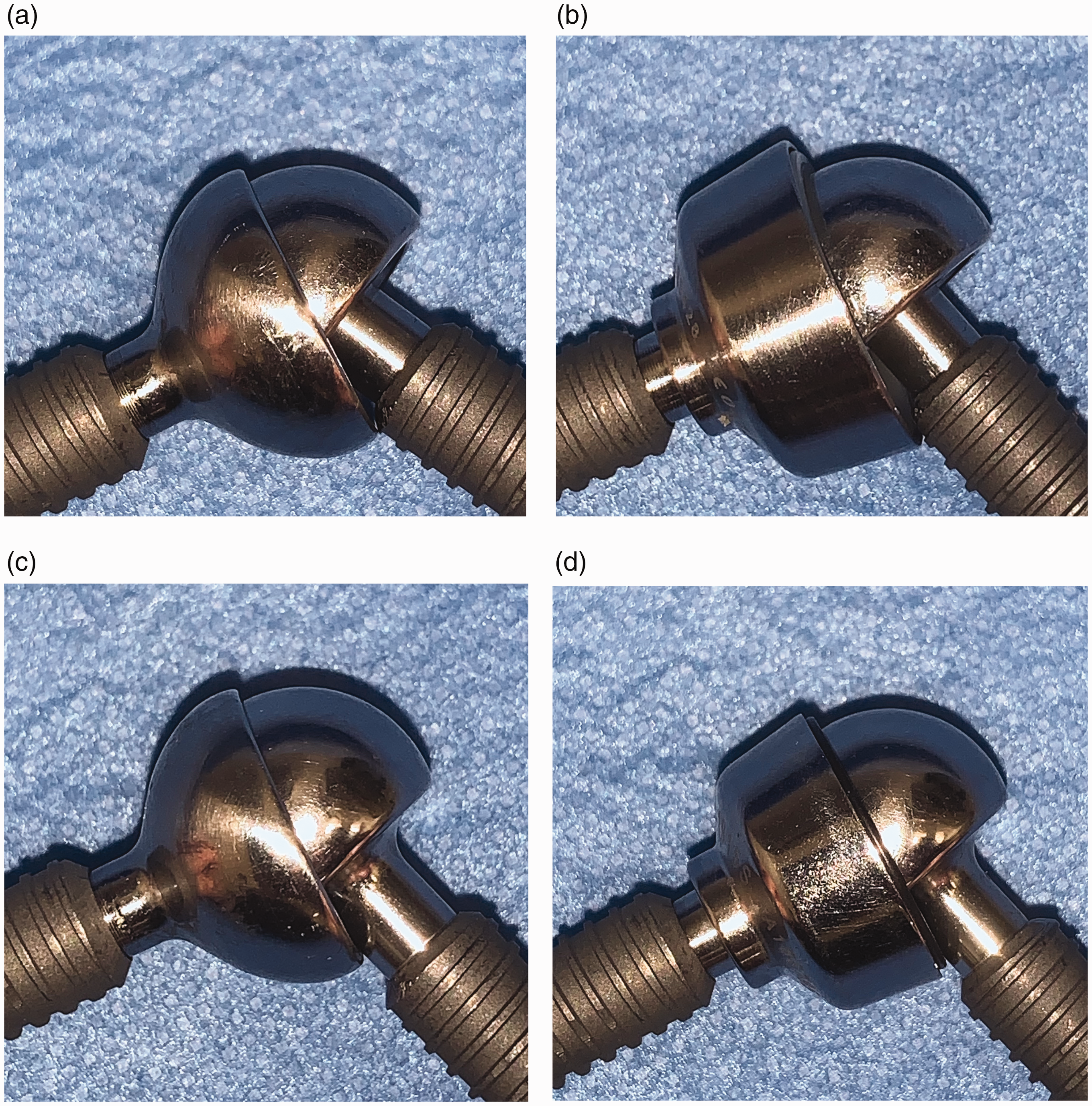
With the short neck, the titanium threaded metacarpal screw impinges on hard CoCr (a) or softer PEEK (b) cup. Note that as the PEEK cup sits proud of the CoCr shell it is the PEEK that impinges against the screw. With the medium neck, the CoCr neck contacts with CoCr (c) or the PEEK (d) cup.
Discussion
This study supports the suggestion of Reigstad and Røkkum (2018) that when the short-necked head is used, impingement occurs between the rim of the cup and the proximal end of the metacarpal screw, causing wear debris and subsequent osteolysis. With the CoCr cup, this means that the harder CoCr will damage the softer titanium screw, releasing titanium alloy debris into the articulation, which may adhere to the head. Titanium has previously been implicated in osteolysis (Taki et al., 2005).
With a medium- or longer necked head, the CoCr cup hits the CoCr neck and causes minimal damage. This is supported by the finding that osteolysis was not seen in any patient in the series with a medium-necked prosthesis.
With the PEEK cup and short-necked head, the harder titanium screw is likely to damage the softer PEEK cup, releasing polymer debris. The explanted cups showed no surface damage that would release detectable amounts of CoCr particulate debris, as evidenced by the normal blood Co and Cr levels. Instead, the heads of cases C and E had adherent titanium alloy debris from the damaged metacarpal screw. The lack of Ti debris on the head of case D can be explained by the smaller defect in the metacarpal screw (and the lack of damage to the cup), which, although releasing a smaller volume of titanium, was likely to have caused osteolysis due to the longer time the implant was in situ before revision.
We believe that this hypothesis of impingement-related osteolysis can also explain the three previously published cases of osteolysis in Motec wrist replacements. Karjalainen et al. (2018) described two cases of Motec TWA failure requiring revision surgery and postulated that both cases were articulation-related failures resulting in adverse reactions to metal and PEEK debris. Their first case was a patient with a MoM articulation who developed osteolysis. The lateral radiograph confirmed a short-necked head and showed identical findings to our series with notching at the proximal edge of the metacarpal screw.
Their second case was of a short-necked metal on PEEK Motec prosthesis. At revision, macroscopic wear scratches and damage were observed on one quarter of the rim of the PEEK cup. The arthroplasty was converted to an arthrodesis. The authors hypothesized that subluxation of the head caused abrasion of the PEEK cup.
Rothe et al. (2022) described a case where osteolysis occurred with a short-necked MoM prosthesis. There was no lateral view to confirm notching. At revision, the short neck was exchanged for a medium one, and the CoCr cup was exchanged for a PEEK one. The authors hypothesized that the cause for the osteolysis was impingement in terminal extension resulting in edge loading and accelerated wear on the MoM articular surfaces.
Our explant analysis does not support this theory of articular wear, and instead supports the suggestion of Reigstad and Røkkum (2018) that it is the result of non-articular wear debris.
Our explant analysis showed clear evidence of damage to the metacarpal screws, adherent titanium debris on the heads and little evidence of articular surface wear. It also confirms that the problem was seen only with the short-necked implant.
A weakness of our study is the relatively small number of explants. Future research will focus on explant analysis of MoM Motec explants where there is no evidence of impingement to further investigate articular surface wear.
As a result of Reigstad and Røkkum’s earlier statement on this issue, the implant manufacturer is aware of this problem and has attempted to address it. Swemac has published a warning in the Motec Wrist Replacement Surgical Technique stating that ‘the short neck prosthesis should only be used in cases of failed proximal row carpectomy (or similar) where the presented space is narrow and the soft tissue tension must be sufficient to ensure that the patient does not have excessive range of motion and therefore an increased risk of impingement’ (Swemac, 2019). They have also increased the length of the medium neck to ensure that it does not impinge on any size of metacarpal screw.
We suggest that surgeons who have used short-neck prostheses in the past keep these patients under close observation, and, if there is any evidence of progressive osteolysis, consider revising the joint components to a medium neck to prevent further progression of osteolysis.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The senior clinical author (DJB) has a paid consultancy role with Swemac for education. He receives no royalties for the use of the products contained in this submission.
Funding
The authors received no financial support for the research, authorship, and/or publications of this article.