
Abstract
We evaluated the frequency of absence of the palmaris longus tendon in the heterogeneous Israeli population. Nine hundred and fifty wrists were evaluated using a modified Mishra/Schaeffer technique (thumb/little-finger opposition with resisted wrist flexion), which was validated by ultrasound scanning. The geographical and ethnic origin of volunteers was documented. When physical examination was equivocal, any vague, superficial structure was subsequently identified as the median nerve by ultrasound. Physical examination reliably identified palmaris longus only when a structure was clinically obvious (visually or by palpation). There was bilateral absence of the palmaris longus in 21% and unilateral absence in 15% of participants. Frequency of bilateral absence varied between 4.5% and 30%, depending on geographical origin (p = 0.0007). The incidence of palmaris longus tendon varied significantly by geographical, but not by ethnic origin.
Introduction
The palmaris longus (PL) tendon is the preferred donor tendon for reconstruction in hand surgery. Tendons and ligaments are both composed of linearly arranged Type-I collagen and thus, a tendon graft can be used to reconstruct either. The PL tendon lends itself to this role due to its length, relative width and expendability. The presence of two other strong wrist flexors, the flexor carpi ulnaris and radialis mean that removing this third, weak flexor does not result in impairment of hand function. The PL tendon, however, is not always present.
Reimann et al. (1944) first reported a cadaveric study involving 1600 extremities and found the absent rate of PL to be 13%. They concluded that PL is one of the most variable muscles in the human body. Subsequently it has been determined that the rate of absence is dependent on geographic location (Gangata, 2009; Raouf et al., 2013) and that the rate varies from 1.5% to 64%.
Various clinical examinations exist for evaluating the presence of the PL and these vary in their accuracy. In one study, 2.6% of PL tendons were missed when using the standard Shaeffer’s test, but found to be present when using Mishra’s method (Kose et al., 2009). The unreliability of clinical examination has been highlighted by reports of median nerve harvest instead of the apparently absent PL (Geldmacher, 1972; Kovacsy, 1980; Vastamaki, 1987; Weber and Mackinnon, 2007).
Israel is a heterogeneous society with populations from diverse geographic and ethnic origins, affording an opportunity to evaluate the incidence of the PL and its correlation with geographic and ethnic origins. The aim of this study is to describe the incidence of PL in the heterogenous Israeli population and investigate potential correlation of incidence to geographical and ethnic origin. A secondary aim is to validate a modified clinical examination that we developed to detect the presence of the PL tendon.
Methods
Study design
This was a prospective cross-sectional study conducted after receiving approval from the local ethics committee according to guidelines from the Helsinki declaration. The inclusion criteria included participants recruited from within our medical centre (staff, patients and visitors) aged 18 years and older. Exclusion criteria were those who are younger and with a history of previous injuries or hand surgery.
Examination for the PL tendon
All examinations were performed by a fellowship-trained hand surgeon who combined two techniques (traditional Schaeffer test and Mishra’s method) by simultaneous opposition of little finger and thumb, together with resisted flexion of the wrist. Using this method, the PL becomes clinically obvious, either visibly or by palpation (Figures 1 and 2).
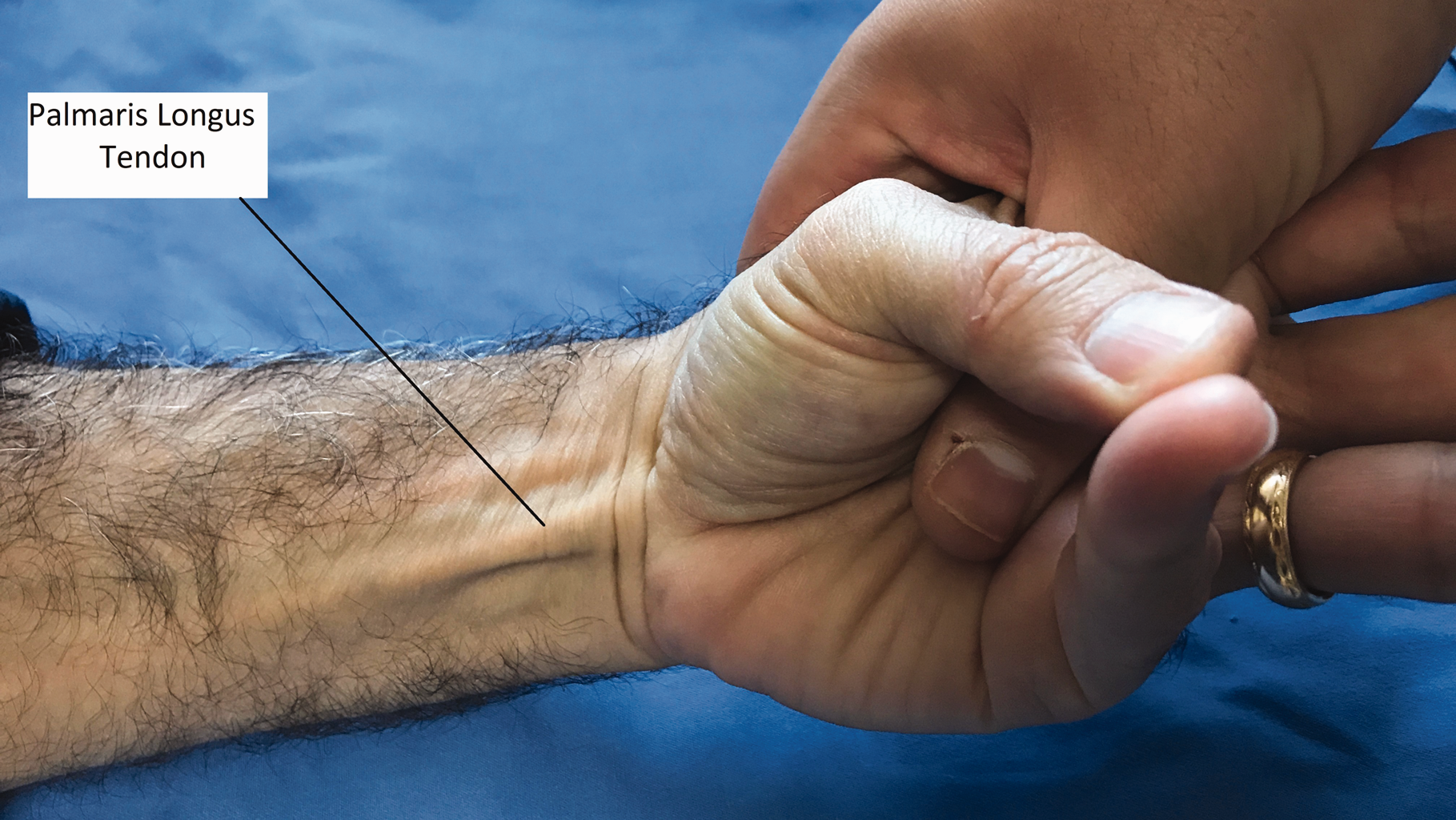
Examination for the presence of the palmaris longus tendon using combined Schaeffer and Mishra tests showing a clinically obvious tendon.

Examination for palmaris longus presence using combined Schaeffer and Mishra tests showing structure (solid line) palpable but not an obvious palmaris longus. (Dotted line indicating FCR tendon).
To validate the examination technique, the modified clinical examination was validated by high-frequency ultrasound (US) in a pilot study involving 100 wrists. Volunteers with PL tendon present according to the modified examination underwent US examination. In all cases the US confirmed presence of PL, thereby establishing the reliability of clinical examination in diagnosing the presence of PL. Volunteers examined during the pilot study were not consented for participation in this study and therefore were not included.
Ultrasound technique
US was performed using Phillips Affinity 70G with an 18 MHz probe to visualize the PL (Figure 3). In wrists with no obvious PL on clinical examination, an US was performed to determine if it was indeed absent or was present but had gone undetected. This approach was changed following 136 US examinations, as the clinical examination was deemed reliable both for confirming and excluding the presence of PL. In all but one of the 136 wrists examined, the clinical examination had proved to be accurate in confirming the absence of a PL. The one exception was in a volunteer where clinical examination did not reveal a PL, but a small, insubstantial tendon (2 mm wide) as demonstrated by US. This hypoplastic tendon was not clinically observable and was not considered to be of clinical significance.
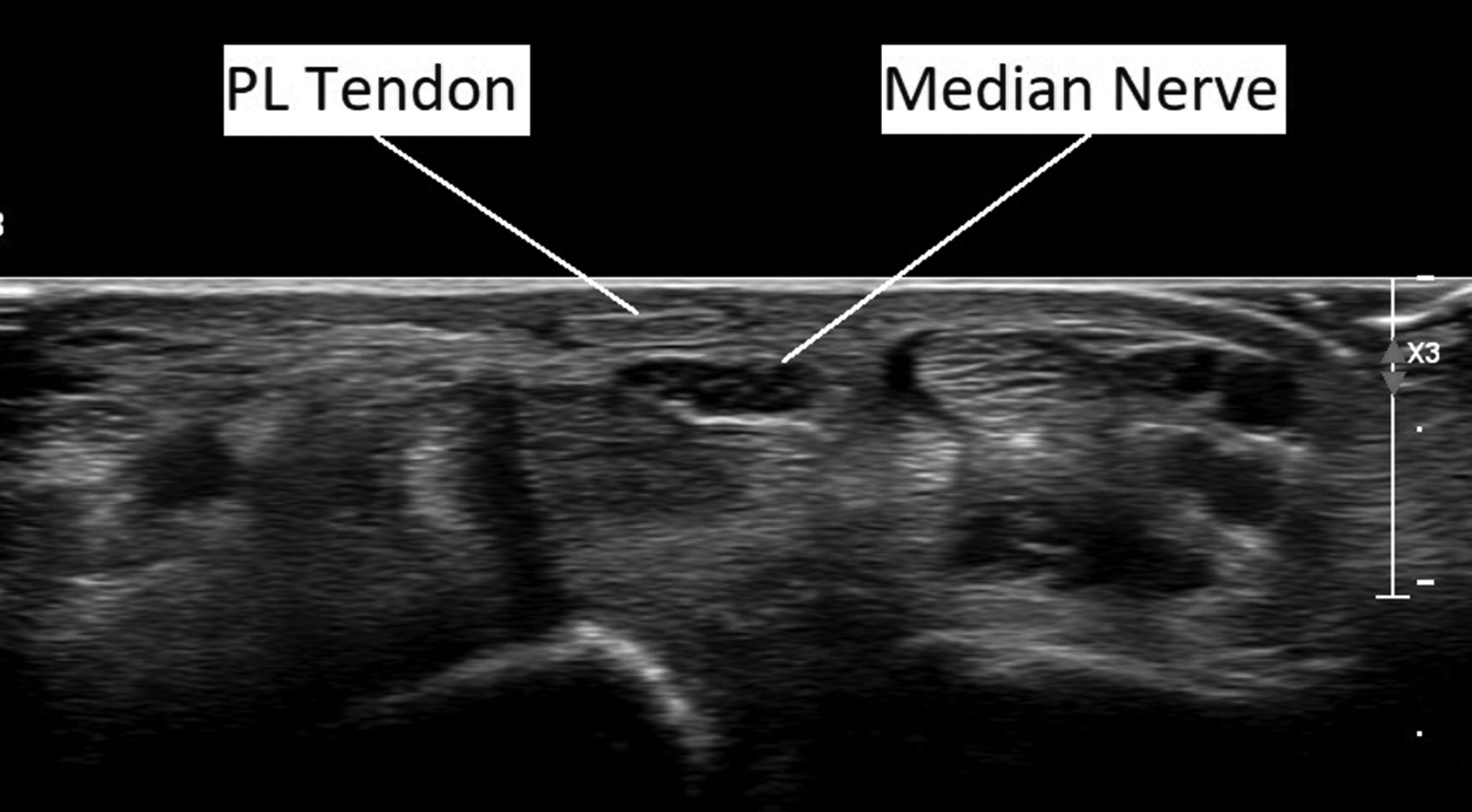
Palmaris longus tendon demonstrated on ultrasound exam. Note its location immediately anterior to the median nerve at the level of the wrist.
Determining geographical and ethnic origin
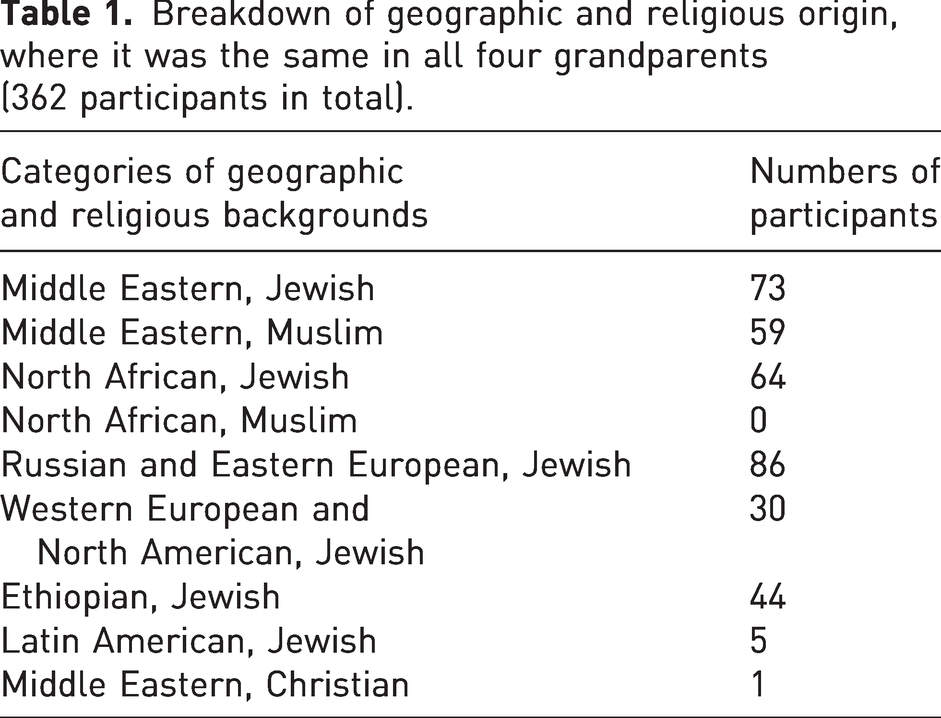
Participants were asked to fill out a de-identified demographic data sheet, which included date of birth, gender, hand dominance, and geographic and ethnic background of all four grandparents. Israel’s high immigration rate since its founding in 1948 has meant that it has a particularly heterogenous population. We attempted to ensure an accurate description of ethnicity by recording the demographic data of participants’ grandparents, as it was unknown to what extent differing degrees of heterogeneity would affect PL incidence. The results in fact demonstrated that the majority of participants (75%) had an entirely homogenous ancestry, with all four grandparents of the same ethnic origin. While this meant that we had more confidence about the influence of ethnic and geographical origin on PL incidence, it did not allow for subgroup analysis of differing levels of heterogeneity, as these groups were too small. We recorded nine categories of ethnic and geographic background (Table 1). Ethnic background for this study was defined as the religious identity of the participants. In recent published guidance for reporting or race and ethnicity in medical journals, ethnicity is classically defined as a person’s cultural identity, for example language, customs or religion (Flanagin et al., 2021).
Breakdown of geographic and religious origin, where it was the same in all four grandparents (362 participants in total).
Results
A total of 475 people (950 wrists) with average age of 44 (18–91) were examined. Fifty-two per cent were female and 86% were right handed. Of the 950 wrists examined, the PL was absent in 268 volunteers (28%), bilaterally in 98 (21%) and unilaterally absent in 72 (15%). There was no significant difference in incidence between those who were right handed (28% absent) and left handed (27% absent) (p = 0.79).
Three hundred and fifty-six participants (75%) stated that all four grandparents originated from the same geographic and ethnic origin (Table 1). Six participants were excluded from statistical analysis, due to the small sample size (Jewish Latin America – 5, Christian Middle Eastern – 1 and Muslim North African – 0). All other participants were included. Bilateral absence varied from 4.5% in the Ethiopian Jewish population to 30% in the Middle Eastern Muslim population (Figure 4). Unilateral absence varied from 0% in the Ethiopian Jewish population to 19% in the Middle East Muslim population (Figure 4).
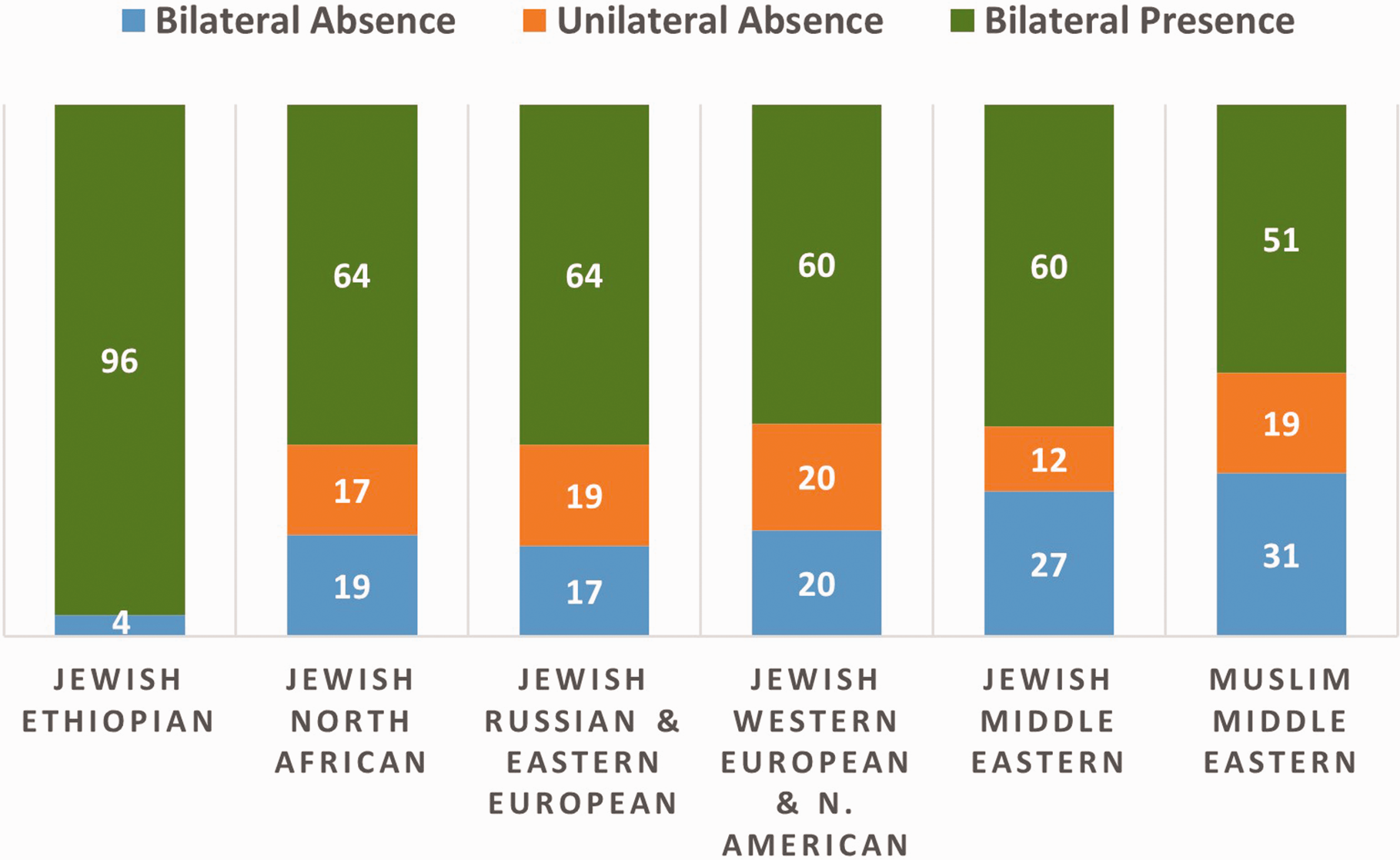
Percentage of the absence and presence of palmaris longus in different religious and ethnic origins.
When analysing geographical origin in isolation, the rate of bilateral absence was 4.5% in the Ethiopian group, 18% in the European and 29% in the Middle Eastern groups (Figure 5). These differences were significant when comparing the Ethiopian and European groups (p = 0.041) and the Ethiopian and Middle Eastern groups (p = 0.0007).
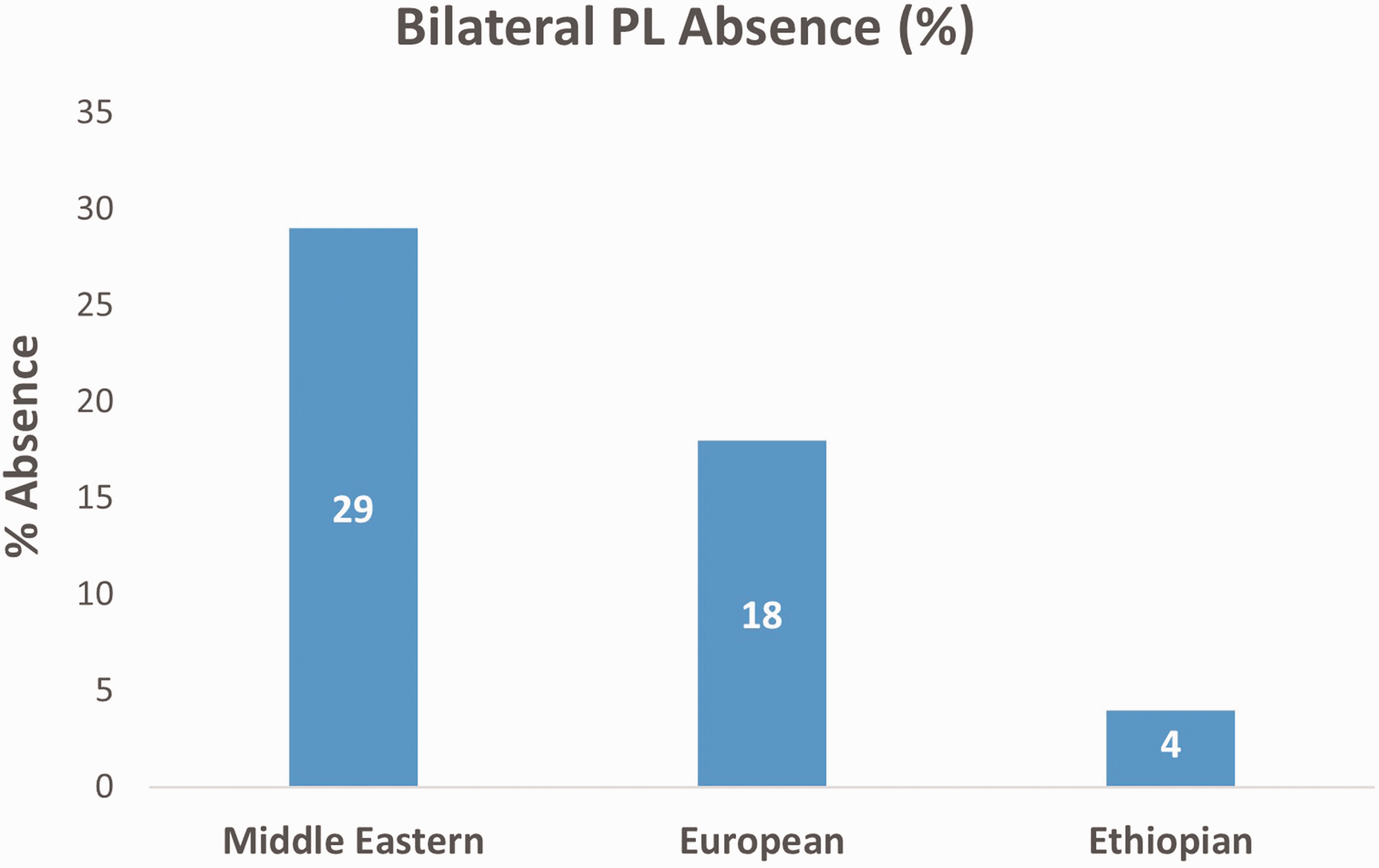
Percentage of bilateral absence different geographical regions.
The difference between European and Middle Eastern groups approached significance (p = 0.0532). There was also a significant difference in unilateral absence between the Ethiopian group and both the European (p = 0.0019) and Middle Eastern (p = 0.0061) groups.
Discussion
In this study, we studied the incidence of the PL tendon in the heterogenous Israeli population and its potential correlation of incidence to geographical and ethnic origin. We also validated our modified clinical examination to detect the presence of the PL tendon. We demonstrated the diverse incidence of PL among different populations and the variation is largely determined by geographical and not ethnic origin.
Various studies have reported on the absent rates of the PL, ranging from 1.5% to 64% (Table 2). These studies are mainly reported in homogeneous populations (Ioannis et al., 2015), but the heterogenous Israeli population provided a unique opportunity to compare volunteers from diverse backgrounds. We chose to include their ethnic background to determine if there was a difference within groups if they are from the same geographical origin. Although other studies have shown that PL incidence varies according to geographical origin, it was not known if ethnic factors also have an influence (Ioannis et al., 2015).
Rate of absence of PL in different geographical regions.
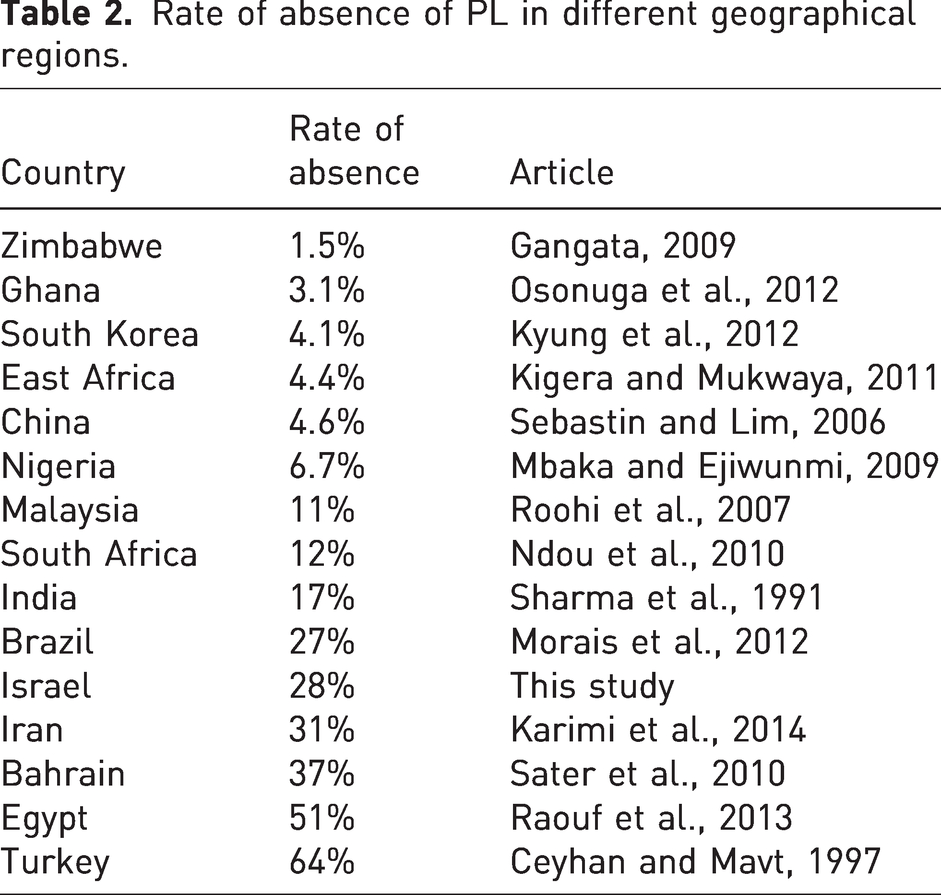
In this study, we found that it is the geographical origin that influences PL incidence, but not ethnic origin. For example, the Ethiopian Jewish population in this study was found to have very similar incidence to other African populations previously examined, but different from other Jewish populations studied. Similarly, Middle Eastern populations in this study had very similar bilateral absence rates irrespective of religion (Jewish Middle Eastern 27% and Muslim Middle Eastern 31%). This finding is somewhat surprising, given that individuals of the same ethnic origin would presumably have similar genetic characteristics and therefore similar anatomy. That geographic origin rather than other aspects of ethnic origin correlates with PL prevalence is therefore an unexpected outcome, as it may suggest that environmental factors are more important than genetic ones in determining PL prevalence. That said, environmental and genetic influences are closely linked to one another (Hand et al., 2015). Whatever the cause, in our study population a statistically significant difference was only demonstrated between participants of different geographical origin.
In choosing how to define ethnicity for this study, several factors needed to be considered. Ethnicity is essentially a social construct and can be difficult to define, therefore it is important to be clear and consistent when discussing issues surrounding this. Flanagin et al, (2021) recommended that individuals should be given the freedom to define their own ethnicity. For this reason, we designed a questionnaire to facilitate this where participants reported their ethnic background by either selecting one of nine predetermined categories, or by specifying an alternative using free text, which also allowed individuals to identify themselves as having more than one ethnicity. For the sake of clarity and practicality it was important to keep the questionnaire simple and the number of options reasonable. Careful thought was given regarding which categories should denote ethnic origin and ultimately, a pragmatic approach was taken where we endeavoured to represent the most common local ethnic groups.
In Israel, the largest ethnic groups identify themselves primarily by religious affiliation and not by geographic origin alone. For example, there are several distinct cultural and religious populations that all have Middle Eastern origin and for this reason, religious affiliation was the primary factor chosen by them to represent ethnicity. Geographical origin was also recorded as an element of ethnicity but analysed as a separate factor. Only three participants elected to use free text for their ethnicity and this likely reflects appropriate ethnicity categories, as participants were able to self-identify using the predetermined categories.
As worldwide populations continue to become increasingly diverse, a patient’s geographical origin and its influence on their anatomy becomes more relevant. Europe, for example, has seen a large influx of Middle Eastern migrants in recent years and local physicians may not be aware of the lower incidence of PL in these populations.
The examination of the PL tendon remains an interesting area of research. A few studies have found Schaeffer’s test to be the most sensitive clinical examination (Johnson et al., 2020; Sadeghifar et al., 2018; Sebastin and Lim, 2006), while others have found Mishra’s first test to be the most sensitive (Kose et al., 2009; Sebastin and Lim, 2006). We found that combining the two techniques into one manoeuvre with simultaneous opposition of little finger and thumb, together with resisted flexion of the wrist, may prove to increase the accuracy of PL detection. When palpating the forearm from distal to proximal, the PL remains superficial. In contrast to this, the median nerve lies superficial to the flexor digitorum superficialis (FDS) tendons at the wrist but courses deep, around the radial side of the FDS tendons to lie between the FDS and flexor digitorum profundus (FDP) in the mid-forearm. Therefore, when palpating at the wrist, the PL can be followed proximally into the forearm, and will always remain superficial.
Prior to this project, a pilot study with the use of US was conducted to establish the reliability of the modified clinical examination in diagnosing PL, as it was initially thought that physical examination alone would be insufficient to rule out PL. Experience early in the study however, showed that physical examination, when carried out using the combined technique, was extremely reliable in demonstrating the absence or presence of PL. We found that no clinically significant PL was missed in 136 patients as proven by US and for this reason, the modified combined physical examination was deemed reliable for the main study. An important caveat is that on occasions, physical examination was equivocal; an indeterminate, vague impression of a superficial structure made it difficult to rule out PL definitively. In all these cases US showed that the vague structure was in fact the median nerve. This led us to conclude that physical examination reliably identified PL only when a structure was clinically obvious (visually or by palpation). In all other circumstances (equivocal cases included) it could be confidently determined that PL was absent.
There are limitations in this study. Despite its reliability, the reliance on physical examination alone to determine the presence of PL rather than US as well, may still be considered a limitation as US is generally recognized as the gold standard for identifying PL. Holzgrefe et al. (2019) recently compared physical examination to US and found it to be only 93% accurate, although they concluded that any clinically obvious PL could be determined by physical examination alone (Holzgrefe et al., 2019). Another limitation was that some demographic groups were under represented (Jewish Latin American, Christian Middle Eastern and Muslim North African) and were thus excluded from the analysis. Further research is necessary to determine the PL incidence in these and other populations. An additional problem caused by the exclusion of these groups is that only six ethnic/geographical groups remained for analysis, with the majority of them constituting participants of Jewish ethnic backgrounds (84%). This variation between the different ethnicities is representative of our medical institution and the wider Israeli population, but does constitute a selection bias, inherent to observational cross-sectional studies.
In conclusion, we found that the incidence of PL varied as a result of geographical instead of ethnic diversity. This study provides further information on the definition of ethnicity and also the need to take into account the increasing heterogeneous nature of our societies when studying anatomical variations.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Obtained from the local ethics Helsinki Commission. 0104-17-SZMC.
Informed consent
There was no need to obtain written informed consent for this study, verbal consent from each participant was obtained according to the guidelines of local ethics Helsinki Commission.