
Abstract
This study aimed to assess the outcomes after simple trapeziectomy and trapeziectomy with ligament reconstruction and/or tendon interposition based on data in the Swedish national healthcare quality registry for hand surgery (HAKIR). Six-hundred and fifty thumbs were included, and 265 were assessed up to 12 months after operation. There was significant and clinically relevant improvement in patient-reported measures (pain on load, pain on motion without load, pain at rest, stiffness, weakness, and ability to perform activities of daily living and the Quick Disabilities of the Arm, Shoulder and Hand score) and objective measures (strength and thumb mobility) at 3 and 12 months for all procedures. The use of the abductor pollicis longus tendon had better improvement in some respects compared with the use of flexor carpi radialis or extensor carpi radialis tendons. However, overall, the use of a tendon adjuncts yielded no better outcomes than simple trapeziectomy.
Keywords
Background
Available evidence suggests that there are no certain differences in terms of patient-reported outcome measures (PROMs) or strength after simple trapeziectomy (TE) versus TE with a tendon-based adjunct (ligament reconstruction and/or tendon interposition) for trapeziometacarpal (TMC) arthritis (Ceruso et al., 2017; Gangopadhyay et al., 2012; Lane et al,. 2020; Li et al. 2011; Liu et al., 2021). Moreover, no tendon-based TE adjunct has proved better than others (Vermeulen et al., 2011).
Registry studies offer an opportunity to compare surgical methods in large samples in a real-life context yielding generalizable results. In the Swedish national healthcare quality registry for hand surgery – HAKIR, the majority of all operations performed at the seven specialist units for hand surgery in Sweden have been registered since 2010. For some surgical interventions, including TE with or without a tendon-based adjunct, an extended assessment has been performed in five hand surgical units since 2011.
The aim of this study was to perform a registry-based study to test the null-hypothesis that there were no differences in improvement of PROMs or objective functional variables between TE and TE with a flexor carpi radialis (FCR), extensor carpi radialis longus (ECRL) or abductor pollicis longus (APL) tendon adjunct.
Method
Data collection
This is an analysis of registry data from HAKIR for all patients operated with primary TE with or without a tendon adjunct for TMC arthritis (ICD-10 code M18) that were included in the extended HAKIR assessment from 2011 to 2019. Age, sex, operated side, Eaton class (Eaton and Glicker, 1987) are recorded. Surgical details, including type of tendon-based adjunct, if performed, resection of the scaphoidtrapezoid joint, arthrodesis or capsulodesis of the first metacarpophalageal joint are recorded by the surgeon. Temporary pinning of the first metacarpal is not registered.
Completeness of HAKIR registration is continuously compared with hospital statistics with the goal to include >80% of all operations. Patients who lack a Swedish social security number or have a protected identity cannot be registered for legal reasons and hence completeness cannot be 100%. Completeness exceeded 80% for the studied period. Inclusion criteria were primary surgery for TMC osteoarthritis with TE with or without a FCR, ECRL or APL tendon adjunct. In HAKIR, a drop-down list gives the alternatives for tendon interposition (APL, ECRL, FCR, etc.), but the exact techniques are not registered (e.g. if a ligament reconstruction and interposition together or only one was performed). Exclusion criteria were concomitant major surgical procedures and secondary procedures (reoperations). Minor simultaneous surgeries, such as trigger finger, carpal tunnel release, ganglion excision or arthrodesis of the metacarpophalangeal joint of the thumb, were not exclusion criteria. In patients operated on bilaterally on different occasions, the second contralateral operation was excluded if it was performed within a year of the first operation. If the type of tendon adjunct was not defined, or none of the methods described above were used, patients were excluded. Figure 1 describes a flow chart of the patients. The study was approved by the Regional Ethical Board D.nr 2017/2023-31.
Flow chart of the patient selection.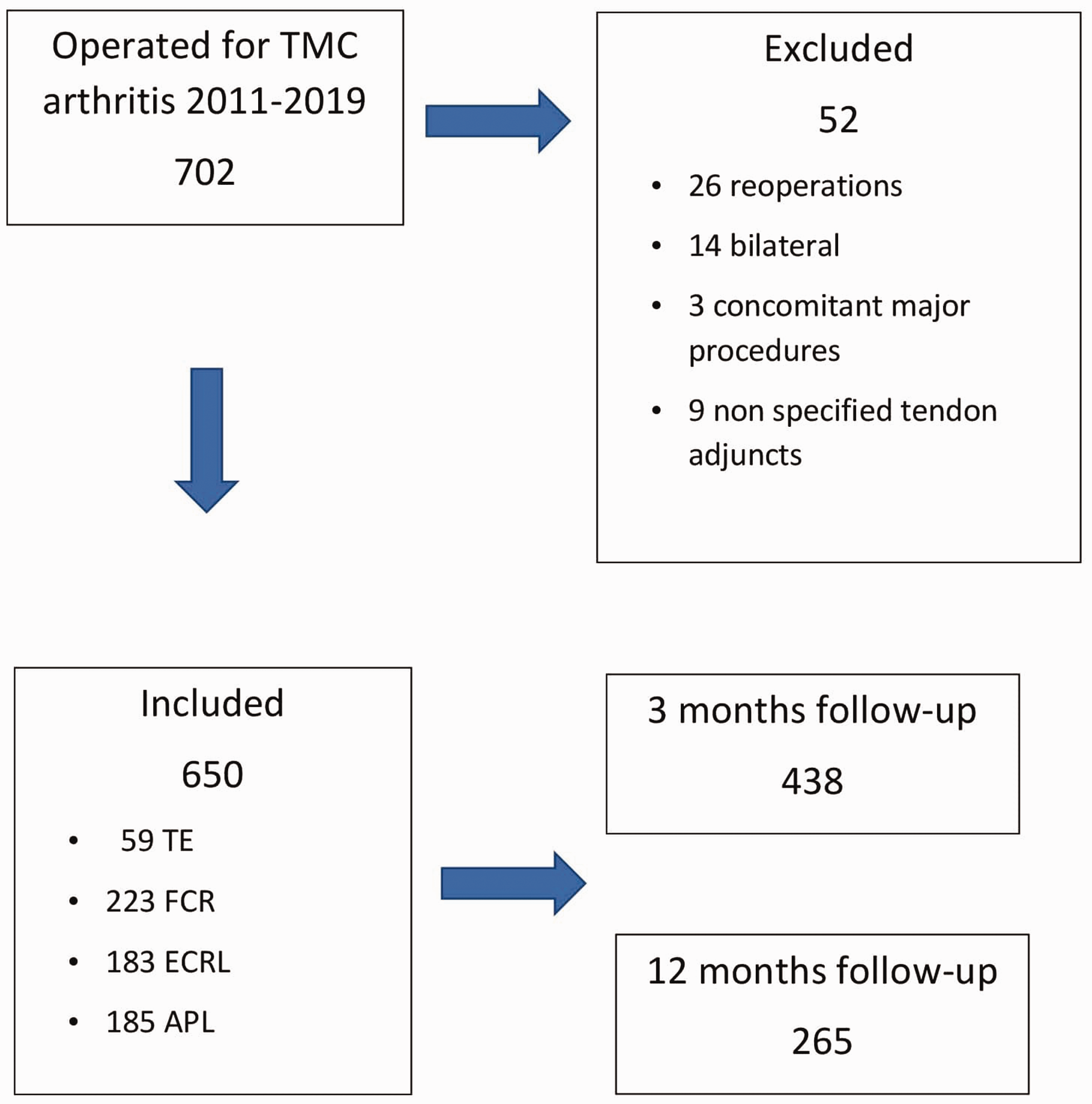
PROMs
Questionnaires are issued to all operated patients before and 3 and 12 months after surgery. The PROM questionnaire in HAKIR (HQ-8) includes eight questions concerning seven symptoms: pain on load, pain on motion without load, pain at rest, stiffness, weakness, numbness, cold sensitivity and the ability to perform activities of daily life (ADL) that are scored with a Likert scale in 10 points increments ranging from 0 (no problem) to 100 (worst problem imaginable) (Supplemental Figure S1). In all variables, higher values mean worse symptoms and disability. The responses are used as single items and are not computed into a total score. The HQ-8 questionnaire has shown good construct validity and ability to detect changes over time (Carlsson et al., 2020). In addition, scores of the Quick Disabilities of the Arm, Shoulder and Hand (qDASH) questionnaire are registered at the same time points (Beaton et al., 2005). The proportion of responses of issued questionnaires in HAKIR have varied from 37% to 50% between 2014 and 2019 (www.HAKIR.se).
Objective physical measurements
Grip, key pinch and tip pinch strengths and radial and palmar abduction of the first metacarpal are assessed by physiotherapists preoperatively, and 3 and 12 months after surgery. A standardized HAKIR-manual for these measurements is used (www.HAKIR.se).
Statistics
In this study, the primary outcome was pain on load 12 months postoperatively. Secondary outcomes were pain on motion without load, pain at rest, stiffness, weakness, ability to perform activities of daily living, qDASH, grip strength (Jamar), key pinch and pinch strength, and radial and palmar abduction of the first metacarpal 3 and 12 months postoperatively. Results for PROMs are presented as median values (IQR) and for objective physical measurements as mean (SD). P < 0.05 was considered significant. The overall improvement of PROMs from preoperatively to 3 and 12 months was analysed with Wilcoxon signed rank test. The surgical methods were compared pairwise regarding postoperative improvement of the PROM variables by ordinal regression, and the pairwise differences are presented as odds ratios (95% CI) with p-value adjusted for age, operated side and hand surgical unit. The ordinal regression does not define the size of the improvements. Residuals showed a slight tendency of overdispersion but no skewness, so the results should be reliable. The improvement of the objective physical measures (grip and pinch strengths, radial and palmar abduction) was compared pairwise between the surgical methods by linear regression adjusted for age, operated side and hand surgical unit. The overall improvement of the objective physical measures from preoperatively to 3 and 12 months was analysed with paired t-test. The risk of missing values at 3 and 12 months with respect to the value at baseline for each variable was analysed with logistic regression.
Confidence intervals and p-values of pairwise comparisons were adjusted using the Tukey–Kramer method to account for multiple testing. Only complete datasets were analysed.
Results
Characteristics
Characteristics of the total sample and of the single surgical procedures.
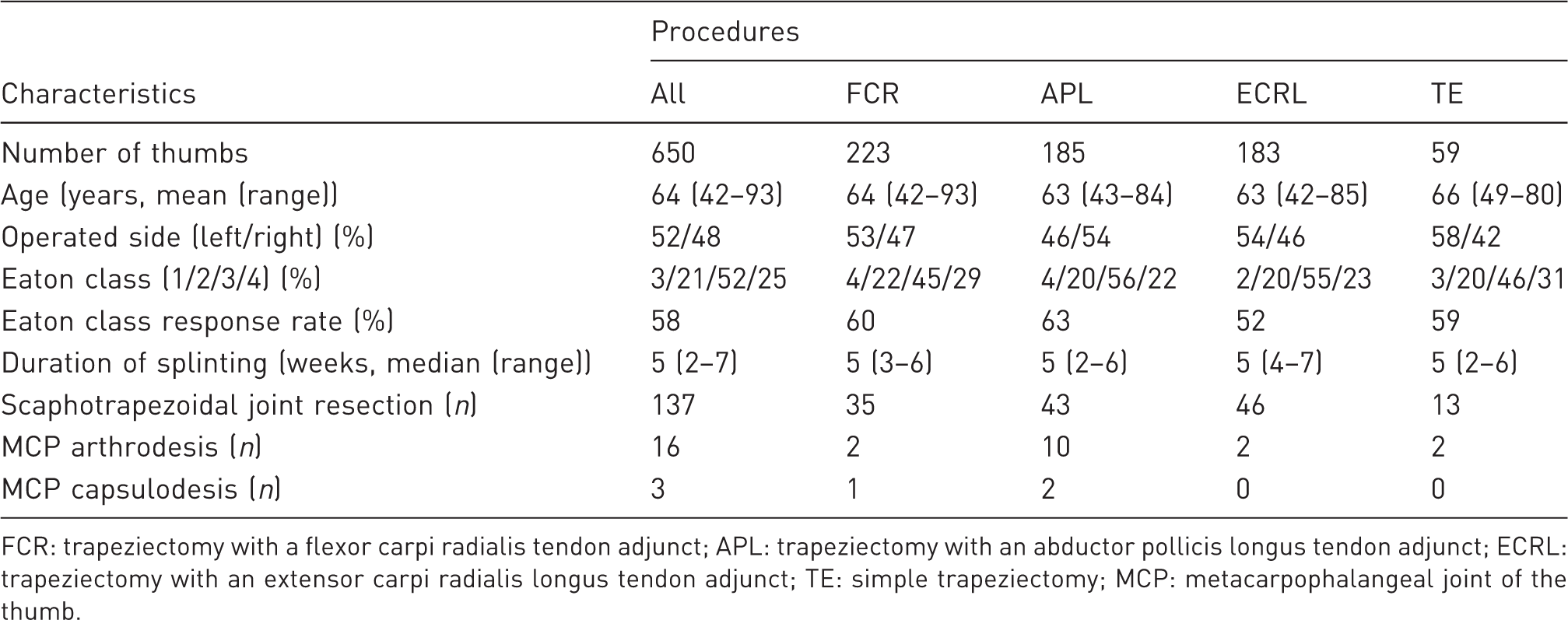
FCR: trapeziectomy with a flexor carpi radialis tendon adjunct; APL: trapeziectomy with an abductor pollicis longus tendon adjunct; ECRL: trapeziectomy with an extensor carpi radialis longus tendon adjunct; TE: simple trapeziectomy; MCP: metacarpophalangeal joint of the thumb.
PROMs
Patient-reported measurements preoperatively and at 3 and 6 months postoperatively (all patients).
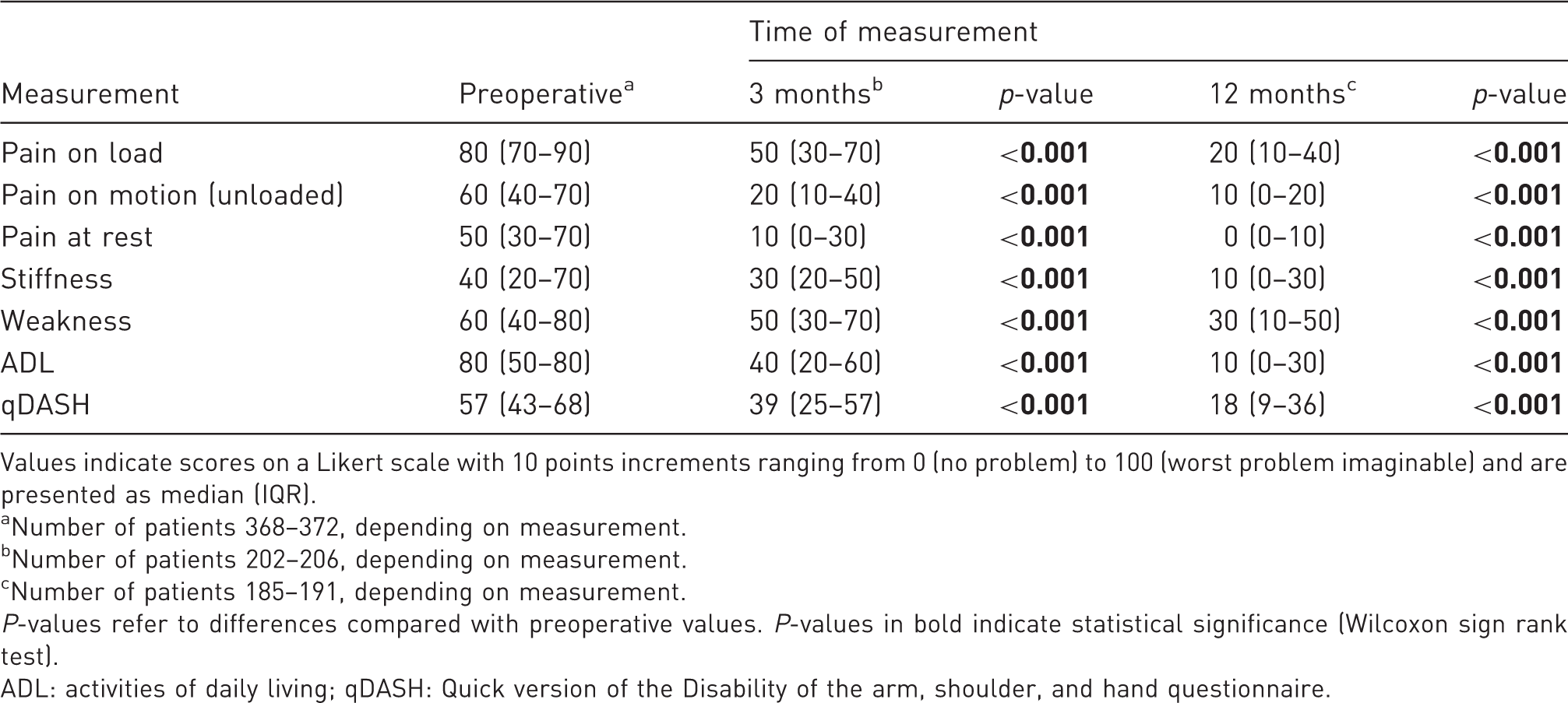
Values indicate scores on a Likert scale with 10 points increments ranging from 0 (no problem) to 100 (worst problem imaginable) and are presented as median (IQR).
Number of patients 368–372, depending on measurement.
Number of patients 202–206, depending on measurement.
Number of patients 185–191, depending on measurement.
P-values refer to differences compared with preoperative values. P-values in bold indicate statistical significance (Wilcoxon sign rank test).
ADL: activities of daily living; qDASH: Quick version of the Disability of the arm, shoulder, and hand questionnaire.
Objective physical measurements
Physical objective measurements preoperatively and at 3 and 6 months postoperatively (all patients).
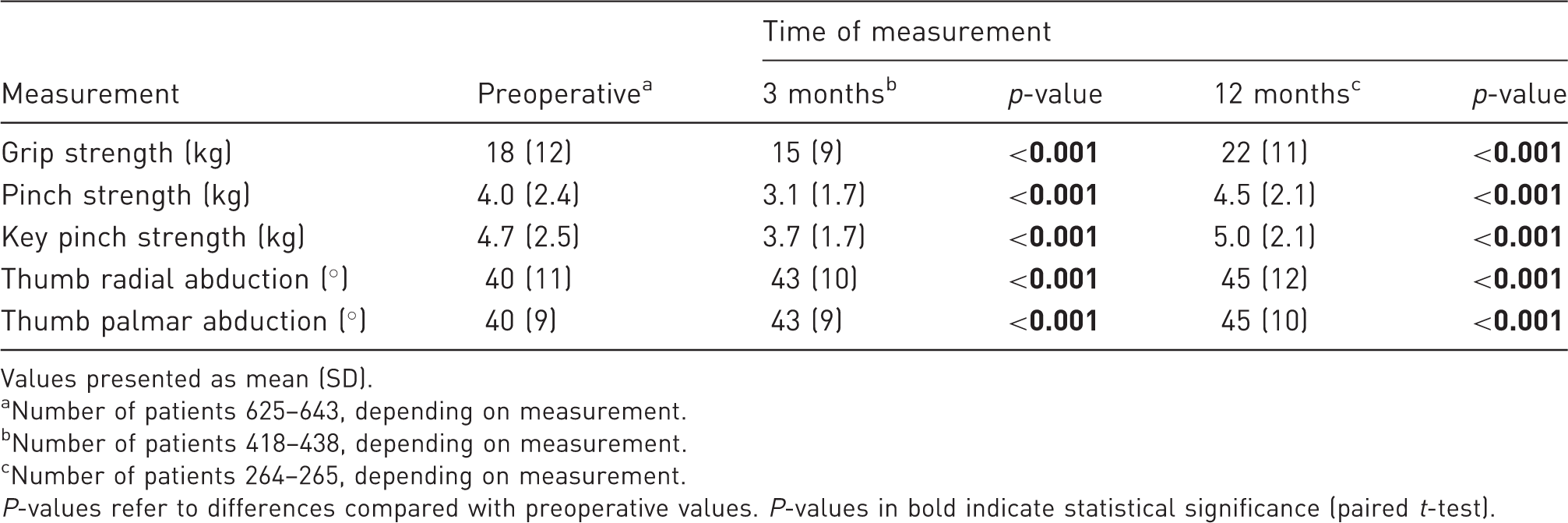
Values presented as mean (SD).
Number of patients 625–643, depending on measurement.
Number of patients 418–438, depending on measurement.
Number of patients 264–265, depending on measurement.
P-values refer to differences compared with preoperative values. P-values in bold indicate statistical significance (paired t-test).
Discussion
This registry-based comparison of TE and different tendon-based TE adjuncts for TMC osteoarthritis at 3 and 12 months postoperatively showed that all methods yielded clinically relevant improvement in PROM scores, but pairwise comparisons implied that APL seemed to have an advantage over FCR, ECRL and TE. There were no differences between TE, FCR or ECRL. Pairwise ordinal regression enables adjustment for covariates but does not define the size of the difference in improvement, thus it is not certain that the difference in odds ratio corresponded to a clinically relevant difference. Increases in strength were small but exceeded estimated minimal clinical important difference for women with TMC osteoarthritis for all methods (Villafañe et al., 2017), and there were no differences between methods. TE had statistically better range of motion than ECRL at 12 months, but the difference was small, and we consider it irrelevant. Comparisons between TE versus TE with tendon adjuncts as entity or versus specific tendon adjuncts were impaired by the low number of TEs, and only differences with very small p-values can be considered as significant. Hence, the lack of differences can at least partly be explained by a lack of power in the statistical analyses.
Efforts have been made to compile and analyse available evidence to identify a superior method for TMC osteoarthritis. Methodological flaws and heterogeneity of studies regarding population, intervention and outcome measurement have made this task challenging. Systematical reviews and meta-analyses have not found any relevant differences in PROMs or strength between TE and TE with tendon adjuncts (Ceruso et al., 2017; Lane et al., 2020; Li et al., 2011; Liu et al., 2021; Martou et al., 2004). A shortcoming in the literature is that the term ligament reconstruction and tendon interposition (LRTI), is often used for all adjunctive tendon procedures, but which tendon and how it has been employed is not described. Few studies have compared different methods of tendon adjuncts. No relevant differences in subjective or objective outcome have been reported between palmaris longus (PL) interposition and FCR–LRTI or between PL interposition and APL ligament reconstruction (Davis et al., 2004; Gangopadhyay et al., 2012; Pomares et al., 2016). The favourable results after APL-based arthroplasty found in this study could possibly be explained by the fact that the tendon is re-tensioned when used for metacarpal stabilization after being flaccid because of the TE. This could be more advantageous than involving an unaffected tendon as an adjunct. There is a lack of studies with long-term follow-up after TE with or without tendon adjuncts, and this study does not add information about potential long-term differences. However, available studies (Gangopadhyay et al., 2012; Kriegs-Au et al., 2004) do not indicate that the surgical method affects the long-term outcome.
Registry studies have the advantage of providing large samples and results reflecting the clinical reality. Conversely, registry studies are retrospective and heterogeneous and include different centres and surgeons with various level of expertise. Expertise level is not recorded in HAKIR and cannot be accounted for in this study. Many different observers have performed the assessments with risk for measurement errors. Another weakness is the lack of specific information of the surgical procedures. TE may include temporary pinning and/or a suture between volar and dorsal capsule structures. There is a myriad of various tendon adjunct techniques that may include a ligament reconstruction and tendon interposition with the possibility of a bone canal through the base of the first metacarpal. Inevitably, the tendon adjuncts in this study (FCR, APL and ECRL) will include different techniques. A surgical centre often has a predominant surgical method and possibly its’ own surgical variant. Therefore, analyses were adjusted for centre. Our perception is that in Sweden, for FCR, APL and ECRL tendon adjuncts, it is likely that both a ligament reconstruction and an interposition have been performed, but some surgeons might have done a ligament reconstruction without tendon interposition.
There are only women in this sample. Perhaps women are more prone to accept extra visits for the sake of the registry. The absence of men restricts the generalizability of the results. The high number of missed data due to low response rate is a problem. Missed data may result in loss of precision in the estimation of differences as well as in loss of power with risk for underestimation of differences. Missed data might also induce selection bias if the effect of the operation differs in non-responders. The results are adjusted for age, operated hand and surgical centre, and the ordinal regression analysis takes baseline pain-level into account. Thus, any difference regarding these factors in non-responders should not affect the results considerably. Although low, the response rate in this dataset is in accordance with other web-surveys (Nulty, 2008). Improving the response rates for PROMs is indeed a challenge of great importance for quality registries. Despite a large population, the low response rate resulted in a sample size about the same as the largest randomized controlled study (Davis et al., 2004). In comparison with registry studies, meta-analyses offer the advantage of a high number of cases from selected trial setting samples where the mixture of several samples might increase the generalizability.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934221086220 - Supplemental material for Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs
Supplemental material, sj-pdf-1-jhs-10.1177_17531934221086220 for Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs by Maria K. Wilcke, Kajsa Evans, Mikael Andersson Franko and Marianne Arner in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934221086220 - Supplemental material for Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs
Supplemental material, sj-pdf-2-jhs-10.1177_17531934221086220 for Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs by Maria K. Wilcke, Kajsa Evans, Mikael Andersson Franko and Marianne Arner in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934221086220 - Supplemental material for Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs
Supplemental material, sj-pdf-3-jhs-10.1177_17531934221086220 for Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs by Maria K. Wilcke, Kajsa Evans, Mikael Andersson Franko and Marianne Arner in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-4-jhs-10.1177_17531934221086220 - Supplemental material for Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs
Supplemental material, sj-pdf-4-jhs-10.1177_17531934221086220 for Trapeziectomy with or without a tendon-based adjunct: a registry-based study of 650 thumbs by Maria K. Wilcke, Kajsa Evans, Mikael Andersson Franko and Marianne Arner in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by AFA research fund.
Ethical approval
The study was approved by the Regional Ethical Board Dnr 2017/2023-31.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.