
Abstract
Skeletally immature wrists are considered at risk of injury due to increased axial loading through a relatively shorter ulna. The aim of this study was to determine whether triangular fibrocartilage thickness relates to ulnar variance and age in adolescents. The radiographs and MRIs of 24 healthy adolescents were retrospectively assessed. Four observers assessed bone age and ulnar variance on radiographs and measured triangular fibrocartilage thickness on MRIs. Median calendar and bone age was 13 years and ulnar variance was −0.7 mm. Median triangular fibrocartilage thickness was 1.4 mm, with excellent inter-observer agreement (r = 0.86). It was moderately correlated with ulnar variance (ρ = −0.46) as well as with bone age (ρ = −0.49). Both variables were statistically significant predictors in a multivariate analysis. This suggests that triangular fibrocartilage thickness changes during skeletal maturation, which might influence axial load distribution in skeletally immature wrists.
Keywords
Introduction
Dynamic variation in ulnar variance (UV) during pronation and supination, as well as structural changes in UV as a result of ulnar-shortening osteotomy or trauma, drastically change axial force transmission (Palmer and Werner, 1984; Werner et al., 1992). Although it has not been statistically proven, the radius in young wrist-loading athletes is considered to bear substantially higher loads than in skeletally mature wrists because of the more negative UV during skeletal maturation, contributing to or even inducing distal radial growth plate injury (Amaral et al., 2014; DiFiori et al., 2006, 2002). The triangular fibrocartilage (TFC) enables approximately 12% of the axial load to be distributed from the radius to the retracted ulna, which bears around 18% of the total load (Palmer and Werner, 1984). In adult wrists with a physiologically positive or negative UV, the biomechanical force transmission to the ulna appears to be similar in wrists with a neutral UV (Harley et al., 2015; Werner et al., 1992). This phenomenon can be explained by the frequently demonstrated negative correlation between UV and TFC thickness; the more positive the UV, the thinner the articular disc in order to maintain similar force distribution (Fortems et al., 1994; Harley et al., 2015; Iordache et al., 2012; Palmer et al., 1984; Sugimoto et al., 1994; Yoshioka et al., 2007). In adults, UV generally appears slightly positive (Sayit et al., 2018). In paediatric wrists however, UV is generally more negative than in adults and tends to become less negative during maturation (DiFiori et al., 2006; Sallam et al., 2020; Sanderson et al., 1997). A rapid increase in relative ulnar length is observed in boys as well as girls between the age of 14 and 15 years (Sallam et al., 2020). UV therefore appears to be dynamic and to become more positive over time.
With the ongoing increase of sports performance in children, it has become important to increase our understanding of their biological characteristics in order to discuss pathological pathways and injury risks (Caine et al., 2008). This is especially true since TFC thickness is currently not taken into consideration when deciding upon ulnar shortening and determining the amount of shortening (Trehan et al., 2019; Wu et al., 2020). The aim of this study was therefore to determine whether TFC thickness relates to UV and age in the skeletally immature wrists of healthy adolescents.
Material and methods
This observational cross-sectional study was based on the strengthening the reporting of observational studies in epidemiology guidelines for reporting observational studies (von Elm et al., 2007). The study is a retrospective analysis of prospectively collected data from adolescents involved in the Physeal MRI study that selected gymnasts with wrist pain, asymptomatic gymnasts and healthy participants aged 12 to 18 years in Amsterdam University Medical Centre, Location AMC, between June 2015 and November 2017 (Kox et al., 2018). The study was performed in accordance with the Declaration of Helsinki and approved by the institution’s Medical Review Ethics Committee (reference no. 2014_382). Written informed consent was given by each participant as well as the parent or legal guardian.
Population
From the Physeal MRI study, this study included girls and boys aged 12 to 18 years without wrist pain over the last 6 months. Participants were not eligible if they had participated in gymnastics, performed wrist-loading sports over two times a week, had fused distal radial physes, were diagnosed with growth disturbance or musculoskeletal diseases, or had a history of wrist fracture, surgery or infection. The participants filled out a questionnaire on demographic information, wrist pain and their weekly amount and duration of sport activity.
Imaging
Conventional posteroanterior radiographs of all participants were obtained in a standardized protocol with 90° shoulder abduction, 90° elbow flexion and neutral forearm position (focus-detector distance 1.30 m). Bone age was determined using validated BoneXpert software (v2.0.1.3; Visiana, Holte, Denmark). UV was assessed by one specialized musculoskeletal radiologist (SJ) using the recommended adapted perpendicular method for this age group (Kox et al., 2020). A negative value for UV indicated a relatively shorter ulna.
MRIs were obtained with a 3T MRI scanner using a dedicated wrist coil (eight channel, receive-only) (Ingenia, Philips Healthcare, Best, the Netherlands) in a feet-first, supine position with the wrist placed neutral, alongside the body. The MRI sequences that were assessed included a coronal proton density turbo spin echo (PD TSE) (echo time, 20 ms; repetition time, 2000 ms; flip angle, 90°; slice thickness, 2.5 mm; field of view, 100 × 88 × 44 mm matrix, 600 × 579 × 22; spatial resolution, 0.30 × 0.32 mm) and a PD TSE with spectral attenuated inversion recovery (echo time, 30 ms; repetition time, 2000 ms; flip angle, 90°; slice thickness, 2.5 mm; field of view, 100 × 88 × 44 mm matrix, 600 × 587 × 22; spatial resolution, 0.30 × 0.32 mm).
Three musculoskeletal radiologists (MM, FS and SJ with 26, 5 and 1 years of experience, respectively) and one hand surgeon (MO with 15 years of experience) from a single centre, individually assessed TFC thickness. Each observer assessed the blinded MRI scans in a randomized order. The observers selected the mid-coronal slice, where the TFC appeared the thinnest. In this slice, the shortest distance between the two articular surfaces of the disc was measured, similar to earlier reported methods (Iordache et al., 2012; Yamanaka et al., 2014; Yoshioka et al., 2007) (Figure 1(a)). In case central TFC thickness could not be assessed due to a hyperintense signal intensity disrupting the disc at its thinnest point, observers were instructed by the score form to report a value of zero (Figure 1(b)). Each observer was blinded for other observers’ measurements. All observers were aware that participants were asymptomatic. They used a diagnostic personal computer workstation with high resolution monitor using IMPAX software version 6.6.1.4024 (AGFA HealthCare N.V., Mortsel, Belgium). The observers were allowed to window and zoom in on the MRIs.
(a) Measurement of TFC thickness on a proton density fat saturated MRI. (b) In this case, TFC thickness could not be measured due to hyperintense signal intensity disrupting the disc at its thinnest point (arrowhead), and a thickness value zero was assigned.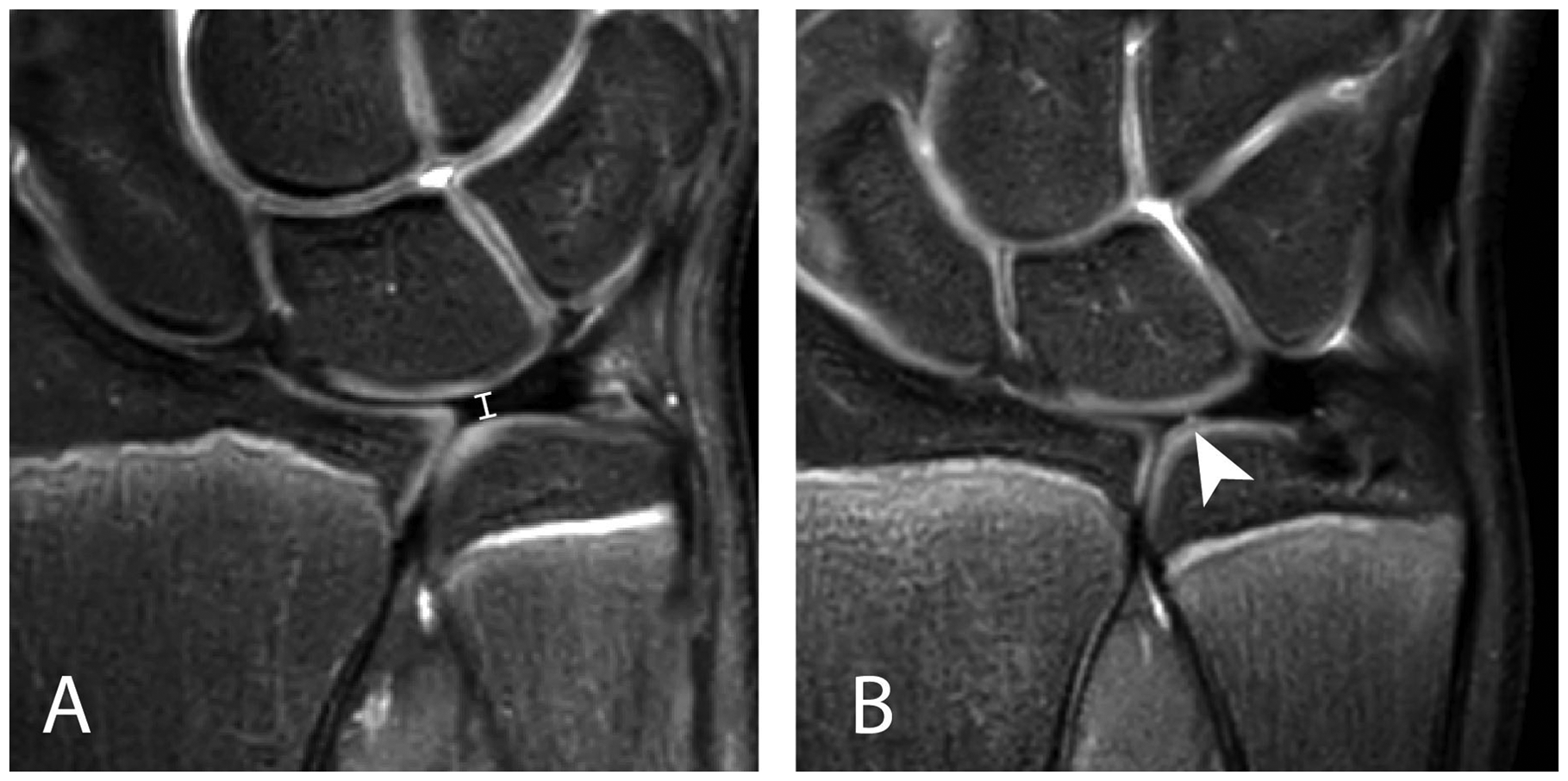
Statistical analysis
All data were entered into Castor Electronic Data Capture (Ciwit BV, Amsterdam, the Netherlands, 2018) and directly imported for analysis in RStudio (RStudio, Inc., Boston). Descriptive statistics were illustrated as medians with interquartile ranges (IQR). Median TFC thickness was calculated by using the average TFC thickness per participant of all observers and further specified by observer. TFC thickness measurements of zero (indicating disc injury, see above) were excluded from median TFC thickness calculation. An intraclass correlation coefficient (ICC) (r) with 95% confidence interval (CI) for inter-observer reliability on TFC thickness measurement of all observers and of all possible observer pairings was calculated using a two-way random-effects (absolute agreement, average measures) model. All TFC thickness measurements were included in these analyses.
Spearman’s correlation coefficient (ρ) with 95% CI between continuous variables (calendar age, bone age, UV and TFC thickness) were calculated using the average TFC thickness per participant of all observers. TFC thickness measurements of zero were excluded from these analyses. Potentially associated variables with the TFC thickness in univariate analysis (p-value <0.10) were included in a multivariate analysis with backwards stepwise elimination. P-values <0.05 were considered statistically significant. All correlation coefficients were interpreted based on the interpretations by Landis and Koch and were structured as poor (≤0.20), fair (0.21 to 0.40), moderate (0.41 to 0.60), substantial (0.61 to 0.80) and excellent (0.81 to 1.00) agreement (Landis and Koch, 1977).
Results
Participant characteristics.
The number of measurements vary between observers due to an inconsistency in determining whether measurement was possible.
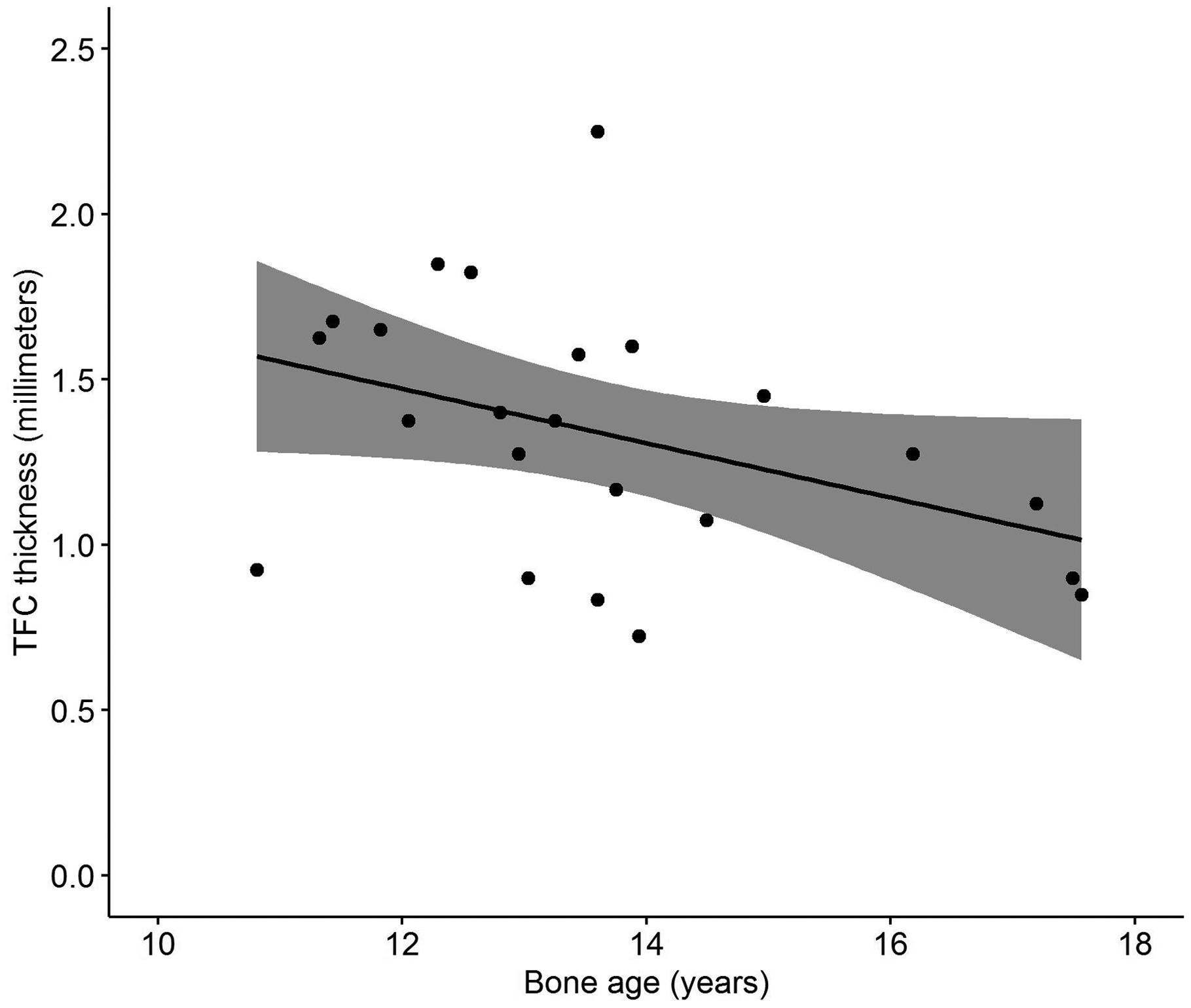
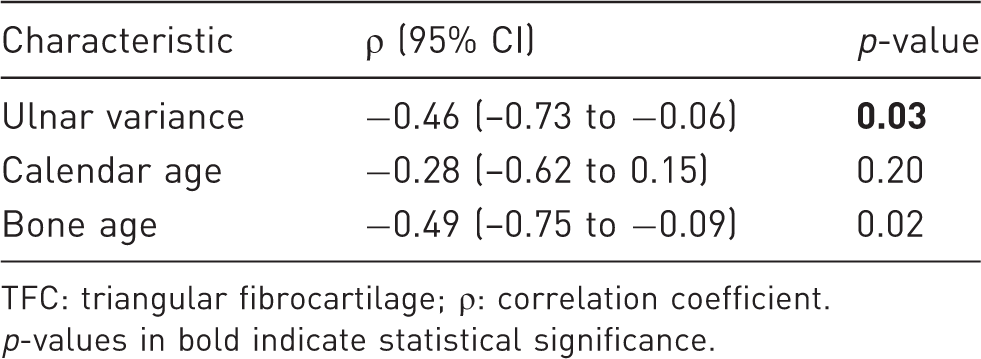
Correlations with TFC thickness are shown in Table 2. There was a moderate correlation between TFC thickness and UV (ρ = −0.46, 95% CI = −0.73 to −0.06, p = 0.03) (Figure 2). Also, there was a moderate correlation between TFC thickness and bone age (ρ = −0.49, 95% CI = −0.75 to −0.09, p = 0.02) (Figure 3). No statistically significant correlation was found between TFC thickness and calendar age (p = 0.20). The correlation coefficient between individual measurements of TFC thickness and UV was statistically significant for all observers, except for Radiologist 1. For bone age, the correlation coefficient with individual TFC thickness measurements was not statistically significant for any individual observer.
Distribution of UV and TFC thickness with the corresponding regression line in black and the confidence interval in grey. Distribution of average TFC thickness and bone age with the corresponding regression line in black and the confidence interval in grey. Correlation between participant characteristics and TFC thickness. TFC: triangular fibrocartilage; ρ: correlation coefficient. p-values in bold indicate statistical significance.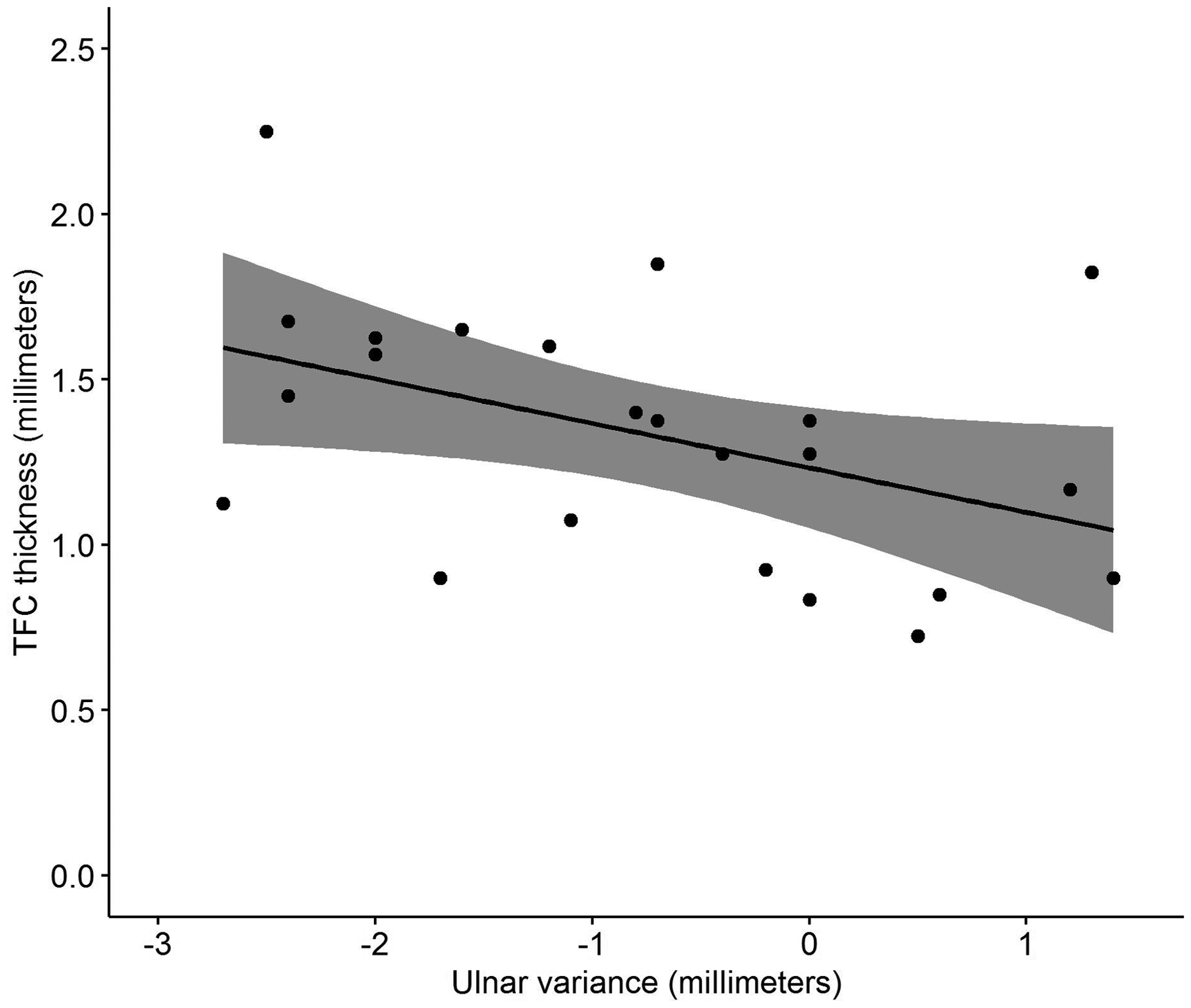
Linear regression analysis with TFC thickness as dependent variable.
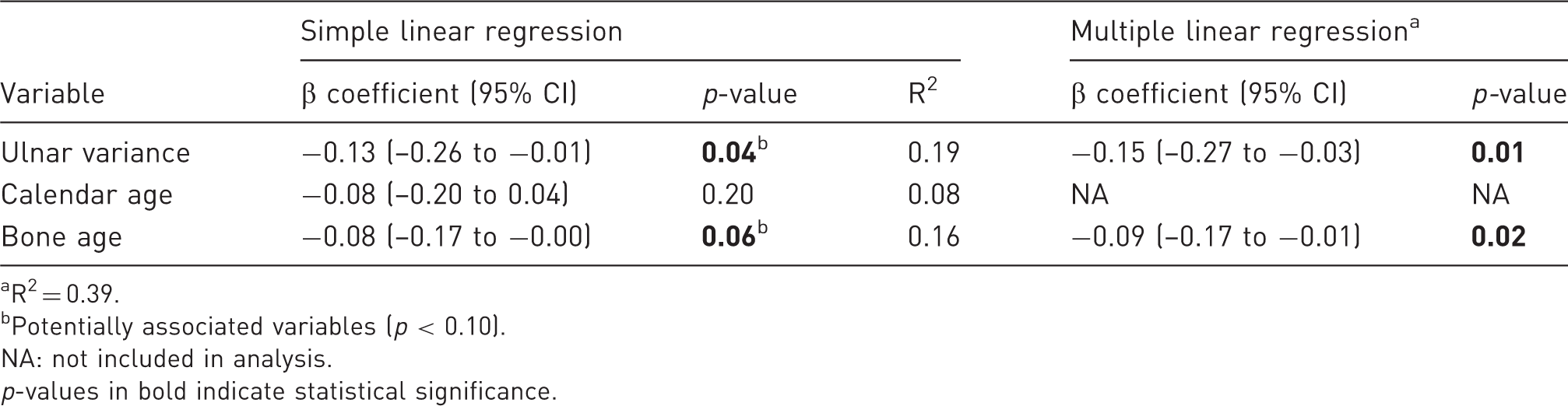
R2 = 0.39.
Potentially associated variables (p < 0.10).
NA: not included in analysis.
p-values in bold indicate statistical significance.
Discussion
In adults, a negative correlation between TFC thickness and UV has already been demonstrated (Fortems et al., 1994; Harley et al., 2015; Iordache et al., 2012; Palmer et al., 1984; Sugimoto et al., 1994; Yoshioka et al., 2007). In two large in vivo studies comprising around 100 wrists of asymptomatic volunteers with a mean age of 30 years, the strength of the correlation ranged from moderate (ρ = −0.56) to substantial (ρ = −0.71) (Iordache et al., 2012; Yoshioka et al., 2007). The present study showed a moderate negative correlation (ρ = −0.46, p = 0.03) between TFC thickness and UV in healthy adolescents. In adolescents, TFC thickness might thus be similarly correlated with UV. The slightly lower correlation coefficient could very well be explained by the substantially smaller sample size of the current study (Lemons, 2009).
The median UV of −0.7 mm is slightly more negative compared with a study on UV in 138 adolescents within the same age range (Goldfarb et al., 2011). These authors found a mean UV of −0.5 mm using the same perpendicular method as in the present study. In children, UV is generally more negative compared with adults and tends to become less negative during maturation (DiFiori et al., 2006; Sanderson et al., 1997). Yet, neither the present study nor the study by Goldfarb et al. (2011) found a correlation between UV and bone age. Possibly, greater numbers of participants are needed to demonstrate this correlation. However, Goldfarb et al. (2011) did find that UV was more negative in boys compared with girls at a bone age of 15 years or younger. Due to the small number of participants in the present study, we were not able to perform subgroup analyses.
The median TFC thickness in the present study was 1.4 mm and the combination of the large number of observers (n = 4) with the excellent inter-observer reliability (r = 0.86) indicates a reliable reference TFC thickness. The TFC appears slightly thicker than observed by several MRI studies in adults with a mean TFC thickness ranging between 1.1 and 1.3 mm (Iordache et al., 2012; Sugimoto et al., 1994; Yoshioka et al., 2007). This thicker TFC in adolescents compared with adults suggests that TFC thickness is not only relatively but also absolutely thicker in skeletally immature wrists.
One study found that TFC’s of patients with a negative or neutral UV contained more cells positive for proliferating cell nuclear antigen than patients with a positive UV (Unglaub et al., 2010). As proliferating-cell nuclear antigen is indicative for potential mitotic cell division, we believe this might explain why a more ulnar negative wrist correlates with a thicker TFC in adolescents (Unglaub et al., 2010). Additionally, in the TFCs of patients with degenerative TFC tears, the number of cells related to apoptosis and necrosis appear more frequently in patients with positive UV than with neutral UV (Unglaub et al., 2008). This could contribute to a decrease in TFC thickness as UV becomes more positive during skeletal maturation. However, in order to demonstrate the UV and TFC thickness change during skeletal maturation, a larger and longitudinal study should be performed.
Compared with reports that included adults, the combination of a thicker TFC and a more negative UV with a comparable correlation coefficient suggests that UV and TFC thickness in adolescents are similarly correlated. Additionally, we found a moderate correlation between TFC thickness and bone age. Even though we did not take exogenous factors such as differences in wrist loading into consideration, this suggests that TFC thickness decreases during skeletal maturation. However, when we further analysed the TFC thickness measurements of the observers individually, no correlation was found with bone age for any observer. Hence, the meaning of this correlation remains questionable.
The present study had several limitations. First, a relatively small sample size might result in less accurate estimations of especially moderate correlations in true populations due to a stronger statistical influence of outliers (Lemons, 2009). However, delicate balancing of the number of healthy underaged participants being subjected to wrist radiographs and MRIs was ethically required. Moreover, even though no gross abnormalities were observed, the possibility of subtle growth abnormalities caused by previous trauma cannot be entirely excluded. Since the participants were all asymptomatic and did not participate in wrist loading-sports more than two times a week, we do believe the selection of participants closely represents the general adolescent population.
The major limitation, however, comprised the reliability of the recommended perpendicular UV measurement. The residual ossification of the ulnar and radial epiphysis in adolescents might inflict a discrepancy between measured UV and actual UV including the non-ossified cartilage (Goldfarb et al., 2011). The Hafner method, which uses the distance between both metaphyses and therefore is less susceptible to cartilage thickness, has proven increasingly unfeasible with bone age from the age of 12 and was therefore unsuitable (Kox et al., 2020). We are, unfortunately, unaware of studies that have determined the variation rates in radial and ulnar cartilage thickness changes through skeletal maturation, and therefore the measurement error for this specific age group remains unknown. Additional measurement of radial and ulnar cartilage thickness on MRI has not been validated in order to approximate actual UV, and we were unable to reliably do so.
Even though the study findings are not statistically conclusive, a negative correlation of TFC thickness with UV and bone age appears to exist. This correlation with UV and bone age suggests that a more negative UV might not necessarily lead to increased axial loading of the radius during skeletal maturation. Potentially, relative TFC thickness even functions as a protective variable in reducing axial loading of the radius in adolescents. Thus, for future studies on axial load distribution and UV in skeletally immature wrists, it appears important to include TFC thickness and bone age.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dutch Plastic Surgery Association Grant.
Ethical approval
Ethical approval for this study was obtained from the institution’s Medical Review Ethics Committee (reference no. 2014_382).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
A pilot study on magnetic resonance imaging of the distal radial growth plate: defining healthy and pathologic characteristics in a non-invasive manner: NL51814.018.14.
Guarantor
MM.
Author contributions
AP, SJ, MO and MM contributed to the conception and design of this study. AP, SJ, FS, MO and MM contributed to the acquisition of data. AP, SJ, MO, KJ and MM contributed to the analysis and interpretation of data. AP, SJ, KJ, FS, MO and MM were all involved in drafting the article and revising it critically for important intellectual content. AP, SJ, FS, MO and MM provided final approval of the version to be published and agree to be accountable for all aspects of the work if questions arise related to its accuracy or integrity.
Acknowledgements
We would like to acknowledge Professor R.J. Oostra for his engagement and contribution in preparing the manuscript.