
Abstract
Surgical A1 pulley release can considerably reduce pain and improve hand function, but individual outcomes are highly variable. This study aimed to identify factors contributing to self-reported pain and hand function 3 months postoperatively. We included 2681 patients who had received surgical treatment for a trigger finger or thumb and who completed the Michigan Hand outcomes Questionnaire (MHQ). Hierarchical linear regression models were used to investigate patient and clinical characteristics associated with postoperative pain and hand function. For both pain and hand function, the most influential factors associated with worse outcomes were worse MHQ scores at baseline (β 0.38 and 0.33, respectively) and ≥3 preoperative steroid injections (β –0.36 and –0.35). These factors indicated that patients with severe preoperative symptoms represent a group with a more advanced disease that is more difficult to treat. These findings can assist clinicians in patient counselling, expectation management and decision-making about the timing of the intervention.
Keywords
Introduction
Release of the A1 pulley on average results in a considerable reduction in pain and improvement in hand function, but also demonstrates a large variability in individual outcomes (Callegari et al., 2011; Kloeters et al., 2016; Nikolaou et al., 2017; Xie et al., 2019). Yet, there is a paucity of literature evaluating factors that may influence functional outcomes following A1 pulley release. Baek et al. (2019) evaluated risk factors for prolonged postoperative symptoms and found that 19% of patients experienced discomfort or a limited range of motion for longer than 8 weeks postoperatively. They showed that a longer symptom duration and a preoperative flexion contracture were associated with prolonged postoperative symptoms. However, their sample with a relatively small number of only 109 patients prevented them from assessing a large number of factors. Further insight into factors that affect postoperative outcomes could aid surgeons in patient counselling, especially regarding expectation management on the outcomes after surgery. This study evaluates the relative contribution of patient characteristics, clinical characteristics and preoperative patient-reported outcome measurement scores to self-reported pain and hand function determined 3 months following A1 pulley release in a large cohort of patients.
Methods
Study design and setting
This is a cohort study of patients who underwent surgical A1 pulley release using data from the Hand Wrist Study Cohort (Selles et al., 2020), reported following the STROBE guideline (von Elm et al., 2007). Between January 2013 and May 2020, we collected data at Xpert Clinics Hand and Wrist Care, currently comprising 25 locations, 23 hand surgeons and over 150 hand therapists. This cohort and data collection were previously described (Selles et al., 2020). The study was approved by the local medical research ethics committee. All patients provided written informed consent.
Participants
All patients who underwent surgical release of a trigger finger or trigger thumb were screened for eligibility. We excluded patients (1) younger than 18 years, (2) if they had prior A1 pulley release of the same digit, (3) if they underwent any surgical treatment of the same hand within 3 months prior to the A1 pulley release, (4) if they were treated for multiple trigger fingers in the same session, (5) if there was an additional treatment of the affected hand during the same session (e.g. carpal tunnel release), (6) if there were missing data in baseline questionnaires or for the number of prior steroid injections, or (7) if there was missing data in the MHQ at baseline or 3 months postoperatively.
Treatment
All surgeries were performed by Federation of European Societies for Surgery of the Hand certified hand surgeons with experience levels ranging from two to five (Tang and Giddins, 2016). Patients underwent open A1 pulley release under local anaesthesia followed by standardized postoperative care, which consisted of a dressing for 3 to 5 days and hand therapy (Huisstede et al., 2014). In general, patients were offered three sessions of hand therapy, although therapists could deviate from the protocol based on clinical considerations and patient preferences. Sutures were removed between 10 and 14 days postoperatively. All patients had a follow-up appointment with their hand surgeon 3 months following surgery.
Variables and measurements
Patients completed the Michigan Hand outcomes Questionnaire (MHQ) (Chung et al., 1998) before surgery and 3 months afterwards (Selles et al., 2020; Wouters et al., 2021). The MHQ is a validated patient-reported outcome comprising six subdomains: overall hand function, activities of daily living, work performance, pain, aesthetics and satisfaction with hand function. In the present study, we only evaluated the pain and hand function subdomains of the MHQ, where the scores range from 0 to 100. For interpretability, scores on the pain subdomain were reverted so that higher scores on both subdomains indicate better performance. We previously demonstrated a minimally important change of 15.7 points for the pain subdomain and 7.7 points for the hand function subdomain in patients undergoing A1 pulley release (Koopman et al., 2021).
Baseline characteristics that were routinely collected included age, sex, systemic comorbidity (i.e. diabetes, rheumatic autoimmune disease, hypothyroidism), body mass index, smoking, type of work, hand dominance, treatment side and symptom duration. In addition, relevant information not included in the routine outcome measurements was extracted from the medical records. This included the presence of a preoperative flexion contracture, prior treatment with one or more steroid injections, and a medical history of hand comorbidity. Comorbidities that were present in less than 1% of patients are not reported.
Statistical methods
We performed two hierarchical multivariable linear regression analyses to examine which baseline characteristics were independently associated with pain (primary outcome) and hand function (secondary outcome) 3 months postoperatively. The variables were added to the hierarchical model in three consecutive steps to evaluate the contribution of a group of variables to the explained variance. First, we included patient characteristics, including age, sex, body mass index, comorbidity and type of work. In the second step, we added clinical characteristics (i.e. treatment of the dominant hand, affected digit, symptom duration, a preoperative flexion contracture and prior steroid injections). In the third step, we also included the baseline MHQ pain or hand function score. Power analysis for a multivariable linear regression with 2681 patients and 26 independent variables showed that our analysis yielded a power larger than 0.95 to detect a small effect size of 0.02 according to Cohen (1988) using an alpha of 0.05.
Results are reported as regression coefficients (B), which represent the increase in the dependent variable for one unit increase in the independent variable when all other variables remain constant. We also reported the standardized regression coefficients (β) to compare the relative contribution of each explanatory variable to the dependent variable. The multiple explained variance (R2) and explained variance adjusted for the number of independent variables (adjusted R2) were calculated for each step. The assumptions of linearity, homoscedasticity, normality and independence were checked by plotting fitted values and residuals, QQ plots, and variance inflation factors (VIF). A VIF of >5 was considered an indication for multicollinearity (James et al., 2013).
We performed a non-responder analysis to compare baseline characteristics of patients who completed (responders) and those who did not complete (non-responders) the MHQ at 3 months postoperatively using t-tests, Wilcoxon tests and chi-squared tests. In addition, we calculated effect sizes for the differences using Cohen’s d for continuous variables and Cliff’s delta for categorical variables. We found differences in age, current smoking status and a history of osteoarthritis, with effect sizes ranging from –0.05 to 0.11 (Online Table S1). A p-value smaller than 0.05 was considered statistically significant.
Results
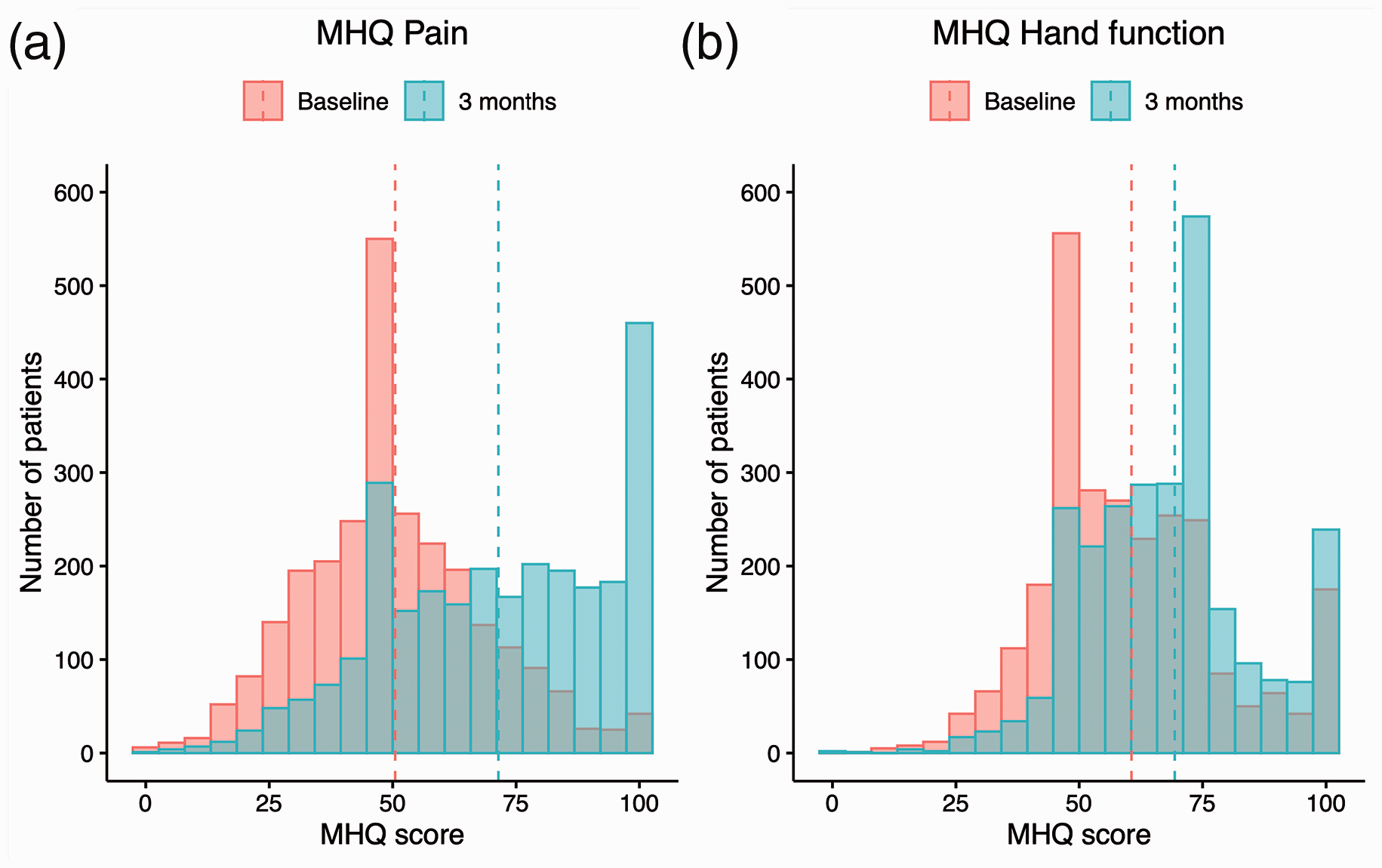
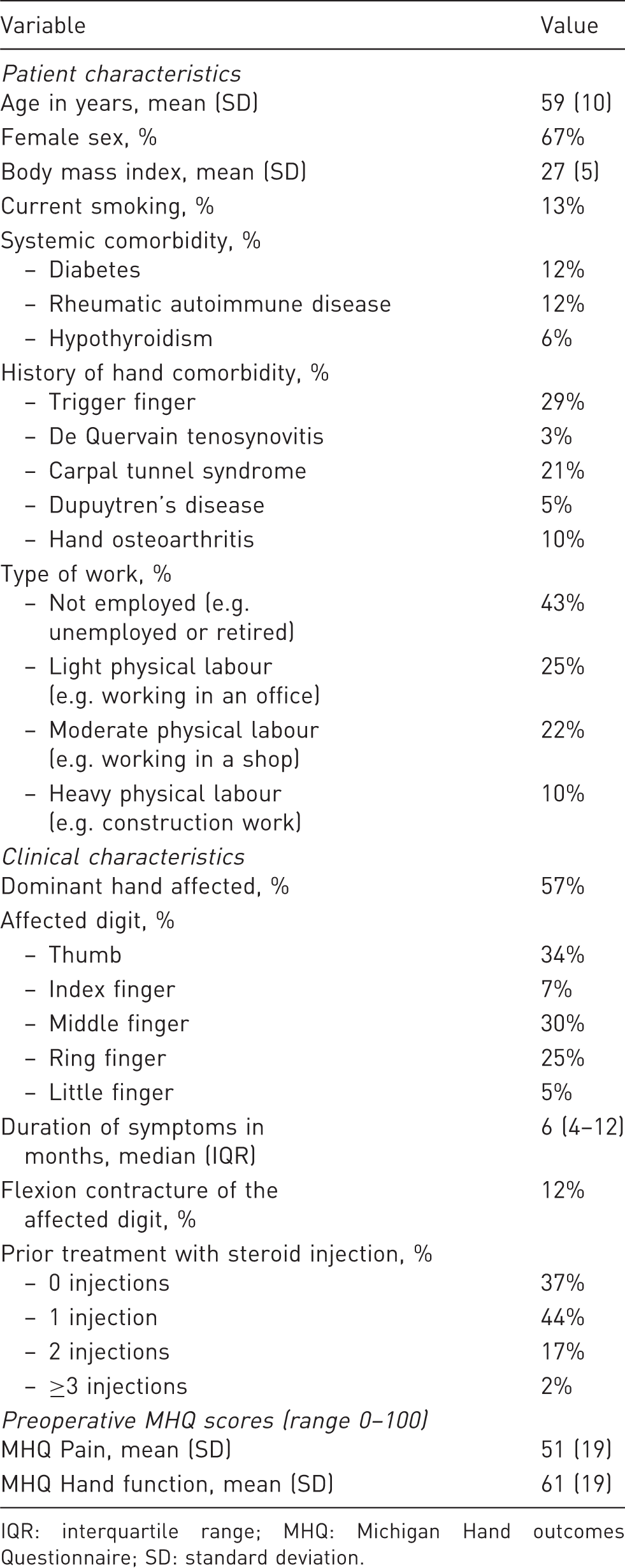
We included 2681 patients in this study (Figure 1). Patients had a mean age of 59 years, and 67% were women (Table 1). The most commonly affected digits were the thumb (34%), middle finger (30%) and ring finger (25%). Figure 2 shows the distribution of the MHQ pain and hand function scores at baseline and at 3 months postoperatively. On average, the pain subdomain improved by 21 points (95% CI 20 to 22), and the hand function subdomain improved by 9 points (95% CI 8 to 10) compared with baseline. However, we found large variability in the distribution of scores and a considerable proportion of patients with low MHQ scores at follow-up (e.g. the proportion of patients with a MHQ score below 50 was 17% for pain and 8% for hand function).
Flow diagram of the study. Distribution of Michigan Hand outcomes Questionnaire scores (MHQ, 0–100, higher scores indicate better outcomes) at baseline and 3 months postoperatively for the (a) MHQ pain and (b) MHQ hand function subdomains. The dashed lines depict the mean MHQ scores. Both subdomains demonstrate an improvement in MHQ scores from baseline to 3 months postoperatively although there is considerable variability in the distribution of MHQ scores. Baseline characteristics of the included patients (n = 2681). IQR: interquartile range; MHQ: Michigan Hand outcomes Questionnaire; SD: standard deviation.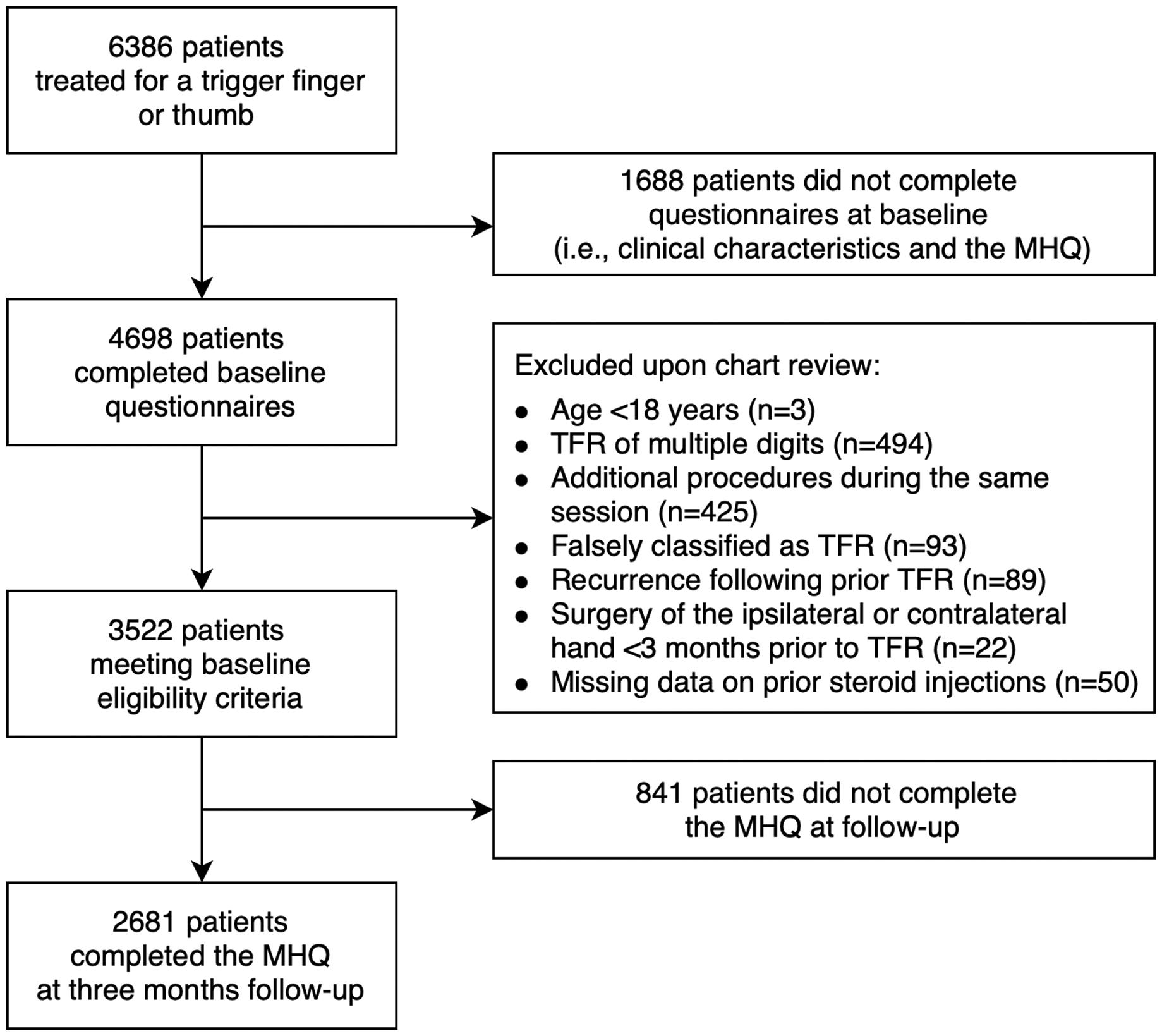
Prognostic factors for pain at 3 months
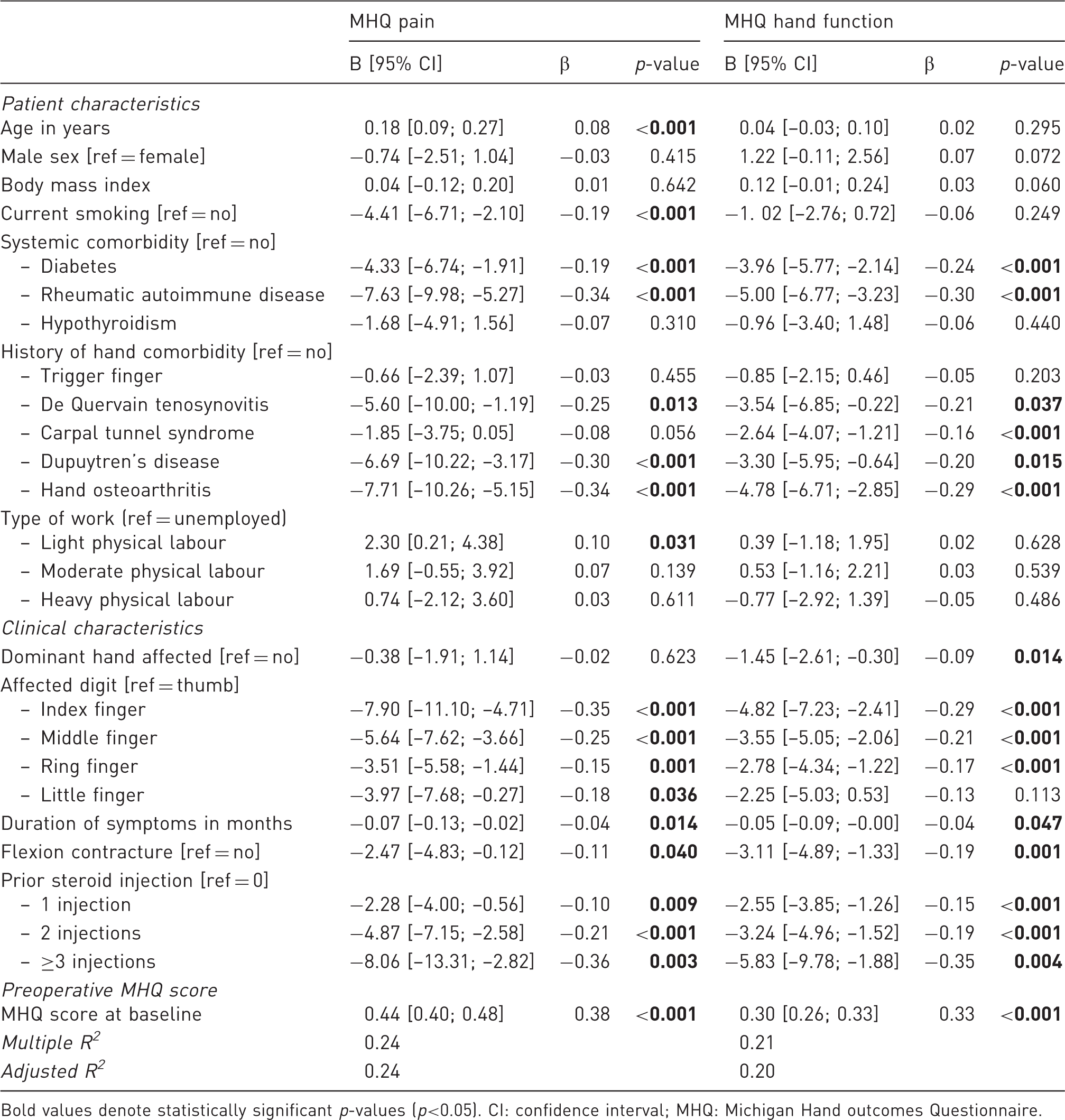
The hierarchical regression analysis indicated that 10% of the variance in postoperative pain could be explained by patient characteristics (Online Table S2). Patient and disease characteristics together accounted for 12% of the variance. Finally, after also including the preoperative MHQ pain score, the full model accounted for 24% of the variation in postoperative pain. The final multivariable model, including all consecutive steps of the hierarchical model, is presented in Table 2. A higher pain intensity was associated with current smoking, diabetes, rheumatic autoimmune disease, a history of various hand comorbidities, treatment of the fingers compared with the thumb, a longer symptom duration, a flexion contracture and one or more steroid injections. In contrast, older age, light physical labour and less pain at baseline were associated with less pain. Figure 3 provides an overview of the standardized regression coefficients of all variables that were significantly associated with postoperative pain, which indicate that pain intensity at baseline (β = 0.38) and receipt of three or more preoperative steroid injections (β = –0.36) were the most influential factors affecting postoperative pain intensity.
Forest plot of the standardized regression coefficients of all variables that were significantly associated with postoperative pain and hand function in the final multivariable regression models. Results are presented as standardized regression coefficients (dots) and 95% confidence intervals (horizontal lines). The vertical line represents the ‘no effect’ line. For both pain and hand function, the most influential variables associated with worse outcomes were a worse baseline severity and three or more preoperative steroid injections. Multivariable linear regression models for pain and hand function at 3 months postoperatively. Results are presented as regression coefficients (B) with corresponding 95% confidence intervals and standardized regression coefficients (β). A negative score indicates that the factor is associated with worse postoperative outcomes. Bold values denote statistically significant p-values (p<0.05). CI: confidence interval; MHQ: Michigan Hand outcomes Questionnaire.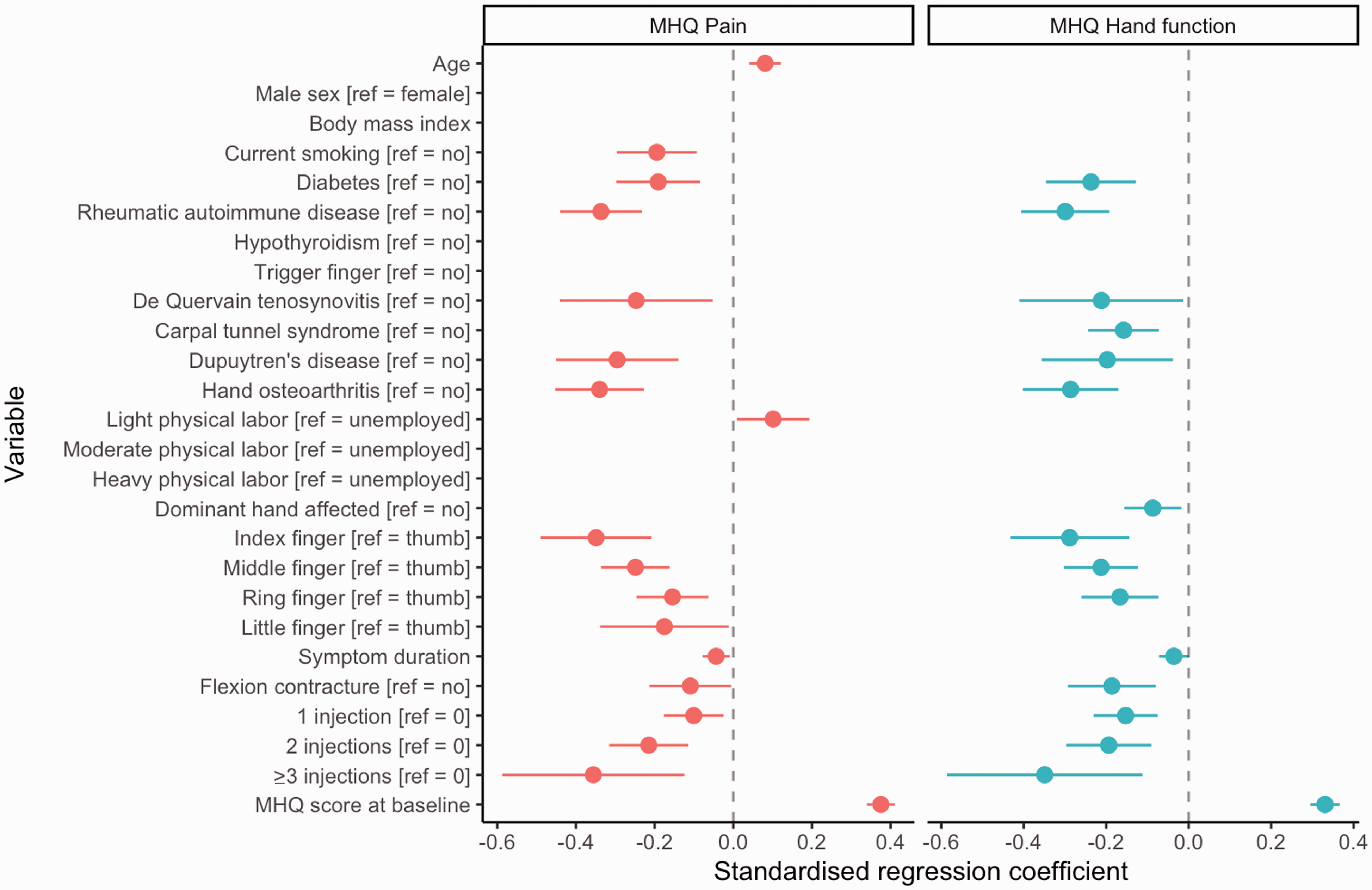
Prognostic factors for hand function at 3 months
The hierarchical regression analysis demonstrated that patient characteristics alone explained 7% of the variance in postoperative hand function (Online Table S3). Following the addition of clinical characteristics, the model accounted for 11%. Subsequently, by adding the baseline MHQ score, the final model explained 21% of the variance in hand function. In the final model, diabetes, rheumatic autoimmune disease, a history of various hand conditions, a longer symptom duration, a preoperative flexion contracture, prior treatment with one or more steroid injections and treatment of the dominant hand, index finger, middle finger and ring finger were associated with a worse postoperative hand function (Table 2). We found that three or more preoperative steroid injections (β = –0.35) and hand function at baseline (β = 0.33) were the most influential factors for postoperative hand function (Figure 3).
Discussion
For both pain and hand function, the most influential factors associated with worse outcomes were a worse baseline MHQ score and three or more preoperative steroid injections, indicating that patients with more severe preoperative symptoms may represent a different group with more advanced disease that is more difficult to treat. These findings can assist clinicians in patient counselling, especially regarding expectation management on pain and hand function after surgery, and may aid surgeons during decision-making about the timing of the intervention.
Of all included patient characteristics, systemic and hand comorbidities were the most influential factors for a higher pain intensity and worse hand function at 3 months. The presence of rheumatic autoimmune disease or hand osteoarthritis resulted in the worst outcomes. This might result from a more severe baseline profile as both disorders can lead to pain and impaired hand function. However, these comorbidities still yielded a considerable negative impact on postoperative outcomes after correcting for several baseline characteristics, including baseline MHQ scores. Hence, another explanation may be that the presence of these comorbidities negatively affects functional recovery following A1 pulley release. We also found that a history of de Quervain tenosynovitis and carpal tunnel syndrome were associated with worse outcomes. It is plausible that these patients are more susceptible to (persistent) tenosynovitis, which may impede recovery following A1 pulley release.
We found that a longer symptom duration, a preoperative flexion contracture, and a worse baseline MHQ score were independently associated with a higher pain intensity and worse hand function at 3 months, indicating that patients with more severe preoperative symptoms may represent a different group with a more advanced disease that is more difficult to treat. Baek et al. (2019) evaluated risk factors for prolonged symptoms following A1 pulley release and also showed that a longer symptom duration and a preoperative flexion contracture were associated with prolonged postoperative symptoms. Future studies may examine if there is a role for preoperative hand therapy or fitting of an extension orthosis to target a preoperative flexion contracture in order to optimize postoperative outcomes. This study also shows that a higher number of steroid injections was associated with a higher pain intensity and worse hand function. Although it is well-known that steroid injections can be highly effective in the treatment of trigger fingers, several studies have shown that the efficacy decreases with repeated injections (Dala-Ali et al., 2012; Newport et al., 1990). Newport et al. (1990) demonstrated that 49% of patients experienced resolution or notable improvement of symptoms following one injection, whereas the success incidence decreased to 23% after two injections and 5% after three injections. In addition, Kang et al. (2021) found that patients requiring multiple steroid injections are more likely to undergo surgical release. An explanation for these findings may be that these patients represent a group with a more advanced disease that is more difficult to treat. Alternatively, as we found that multiple steroid injections were independently associated with worse outcomes after correcting for the symptom duration, baseline symptom severity and the presence of a flexion contracture, these results suggest that steroid injections may also negatively impact postoperative outcomes. Hence, further insight into factors associated with a low efficacy of steroid injections could aid clinicians in identifying patients that may benefit from earlier surgical release. This could have benefits from both patient and societal perspectives, as a reduced number of steroid injections and better surgical treatment outcomes are also cost-effective.
Our study also determined that treatment of the fingers compared with the thumb was associated with worse postoperative outcomes. This is in line with the findings of Moriya et al. (2005) demonstrating that the duration until the symptoms subsided was shorter for patients surgically treated for a trigger thumb (2 weeks) than for a trigger finger (5 weeks). These findings may be explained by the differences in functional anatomy. For example, our finding that the index and middle finger yielded the worst outcomes may be explained by their large contribution to the fine motor skills of the hand. Hence, these fingers may be more susceptible to overloading and persistent tenosynovitis, resulting in prolonged pain and functional difficulties.
Although some of the effects may seem small, several of the aforementioned characteristics often coexist in patients. For example, compared with patients with a favourable profile (healthy patients undergoing A1 pulley release of the thumb as primary treatment), patients with a less favourable profile (patients with rheumatic autoimmune disease undergoing A1 pulley release of the index finger following two preoperative steroid injections) yield a considerably higher pain intensity of 21 points. This illustrates the substantial impact that a combination of characteristics may have on the postoperative outcomes. Future studies may focus on predictive modelling to further optimize expectation management for individual patients.
This study has several limitations. First, the observational design of this study was associated with a large proportion of missing data. In the non-responder analysis, we found that non-responders were younger, more often smokers and less often had a history of osteoarthritis. However, the effect sizes ranged from –0.05 to 0.11, indicating very small effects, and may therefore not affect our findings (Cohen, 1988). Second, we retrospectively reviewed all medical records to collect information on a history of hand comorbidity, the presence of a flexion contracture and prior treatment with one or more steroid injections, which may have resulted in an underestimation. To account for this, we excluded patients with an unknown number of prior steroid injections. However, as the absence of a preoperative flexion contracture or a history of hand comorbidity is often poorly reported, we did not exclude these patients as this could have led to selection bias. This possible underestimation may have resulted in an underestimation of the regression coefficients. Third, we excluded patients undergoing revision surgery following prior A1 pulley release in this study as these patients only comprised a very small proportion of our sample. Previous studies have shown that approximately 1% of patients require revision surgery (Bruijnzeel et al., 2012; Everding et al., 2015). Therefore, further insight into postoperative outcomes and prognostic factors for outcomes following revision surgery is required. This should aid clinicians during patient counselling and surgical decision-making in patients who do not benefit from a primary A1 pulley release.
The factors that influence postoperative pain and hand function in the present study only partially explain the variance in postoperative outcomes, indicating that there may be additional factors. Previous studies suggest that the extent of tenosynovitis (Freiberg et al., 1989) and the condition of the tendon (Baek et al., 2019) may also influence postoperative outcomes. It would therefore be interesting to examine to what extent the clinical staging of the disease contributes to postoperative outcomes and to compare these results with outcomes following conservative management. Furthermore, investigators have also demonstrated that treatment expectations and psychological factors play an important role in postoperative outcomes following surgical decompression of carpal tunnel syndrome (Sun et al., 2021) and De Quervain tenosynovitis (Blackburn et al., 2021). Future studies may examine other factors contributing to postoperative pain and hand function. This may optimize patient counselling and clinical decision-making about preoperative management and timing of the intervention to improve outcomes following surgical A1 pulley release.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934221085401 - Supplemental material for Factors associated with self-reported pain and hand function following surgical A1 pulley release
Supplemental material, sj-pdf-1-jhs-10.1177_17531934221085401 for Factors associated with self-reported pain and hand function following surgical A1 pulley release by Jaimy E. Koopman, Caroline A. Hundepool, Robbert M. Wouters, Liron S. Duraku, Jeroen M. Smit, Ruud W. Selles, the Hand-Wrist study group J. Michiel Zuidam in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934221085401 - Supplemental material for Factors associated with self-reported pain and hand function following surgical A1 pulley release
Supplemental material, sj-pdf-2-jhs-10.1177_17531934221085401 for Factors associated with self-reported pain and hand function following surgical A1 pulley release by Jaimy E. Koopman, Caroline A. Hundepool, Robbert M. Wouters, Liron S. Duraku, Jeroen M. Smit, Ruud W. Selles, the Hand-Wrist study group J. Michiel Zuidam in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934221085401 - Supplemental material for Factors associated with self-reported pain and hand function following surgical A1 pulley release
Supplemental material, sj-pdf-3-jhs-10.1177_17531934221085401 for Factors associated with self-reported pain and hand function following surgical A1 pulley release by Jaimy E. Koopman, Caroline A. Hundepool, Robbert M. Wouters, Liron S. Duraku, Jeroen M. Smit, Ruud W. Selles, the Hand-Wrist study group J. Michiel Zuidam in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
The authors thank all patients who participated and allowed their data to be anonymously used for the present study. Hand-Wrist Study Group collaborators: DJJC van der Avoort, RAM Blomme, HL de Boer, GM van Couwelaar, J Debeij, R Feitz, A Fink, KP de Haas, K Harmsen, L Hoogendam, SER Hovius, R van Huis, R Koch, YE van Kooij, A Kroeze, TM Moojen, MJW van der Oest, PY Pennehouat, WA de Ridder, JP de Schipper, K Schoneveld, HP Slijper, BJR Sluijter, J Smit, X Smit, JS Souer, M ter Stege, JFM Temming, JS Teunissen, JH van Uchelen, JJ Veltkamp, GM Vermeulen, ET Walbeehm, OT Zöphel.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Medical Ethics Review Committee of the Erasmus Medical Centre (MEC-2018-1088).
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.