
Abstract
This study aimed to determine normal values of three parameters commonly used to determine malunion by investigating intact scaphoids on sagittal computed tomography images from healthy individuals. We analysed 62 normal scaphoids and found the mean height–length ratio, lateral intrascaphoid angle and dorsal cortical angle to be 0.58, 27° and 128°, respectively. These measurements had good-to-excellent, poor-to-moderate and moderate-to-good inter- and intra-rater reliabilities, respectively. This study provides information on normal parameters of the scaphoid that may inform clinical decision making when assessing malunion. We suggest that the lateral intrascaphoid angle should be used with great caution as a measure of deformity.
Introduction
Scaphoid waist fractures are not often displaced, but they can be complicated by extension, supination and anterior translation of the proximal fragment relative to the distal fragment, creating a so-called ‘humpback deformity’ with or without union (Schwarcz et al., 2017; Schweizer et al., 2012; Weber, 1980). Humpback deformities disrupt carpal kinematics of the entire wrist and, in some cases, result in dorsal intercalated segment instability (DISI) deformity that causes decreased range of motion of the wrist, pain and osteoarthritis (Amadio et al., 1989; Burgess, 1987; Gillette et al., 2017; Nakamura et al., 1991; Smith et al., 1989). Currently there is no consensus on reliable measurements of scaphoid deformity; various measurements are currently applied and their influence on patient outcomes is a subject of considerable research. The lateral intrascaphoid angle (LISA) has been suggested to be a good predictor of outcome by some studies, while others have indicated it to be a poor predictor of outcomes, including restoration of motion, relief of pain and regain in function (Afshar et al., 2015; Amadio et al., 1989; Bain et al., 1998; Gillette et al., 2017; Jiranek et al., 1992). The LISA is also suspected to have poor inter- and intra-rater reliability; however, it is commonly used when determining malunion (Bain et al., 1998). The height–length ratio (H/L ratio) has been shown to have a high intra- and inter-rater reliability but is a poor predictor of outcome (Lee et al., 2015). The dorsal cortical angle (DCA) appears less prone to observer bias than the LISA, but is a poorer predictor of outcome. However, the DCA is not as well studied as other measurements of scaphoid deformity (Forward et al., 2009; Megerle et al., 2012; Ring et al., 2005).
To the best of our knowledge, normal ranges for H/L ratio, LISA and DCA have not been reported from a large group of normal individuals. For these measurements to be studied and used for the prediction of patient outcomes, the normal ranges must first be determined. The present study aimed to determine the normal values of the most commonly used measurements (H/L ratio, LISA and DCA) from sagittal computed tomography (CT) scans of the scaphoid bone. The second aim was to investigate whether these parameters can be reliably measured by different observers.
Methods
We searched our database for all available CT scans of hands and wrists taken with a Toshiba Aquilion One 320 scanner (Toshiba, Tokyo, Japan) in our institution between 1 January 2016 and 31 May 2019. We included CT scans of wrists with no disorders and CT scans with disorders that were not related to the carpus. Exclusion criteria were: patient age of <18 years; any type of scaphoid pathology (e.g. fractures, osteoarthritis, arthritis, enostoses, cysts); signs of carpal instability (e.g. intercalated segmental instability configurations, scapholunate widening); osteoarthritis or arthritis of the wrist and/or carpal bones; fractures of the radius and/or carpal bones; and signs of diseases in the carpus (e.g. Kienböck’s disease, congenital disorders). All CT scans were reformatted along the long axis of the scaphoid using IMPAX Client 6.6.1.8006 software (AFGA Healthcare, Mortsel, Belgium) and images of 0.5–2 mm thickness were obtained. A single central image was then selected, in which the scaphoid appeared to have the greatest length. Three observers; a musculoskeletal radiologist (DIR), a hand surgeon (RG) and an orthopaedic resident (CWG); carried out measurements. The observers were blinded to other clinical information and the other observers’ measurements. Each observer repeated all measurements after at least 2 weeks.
Measurement techniques
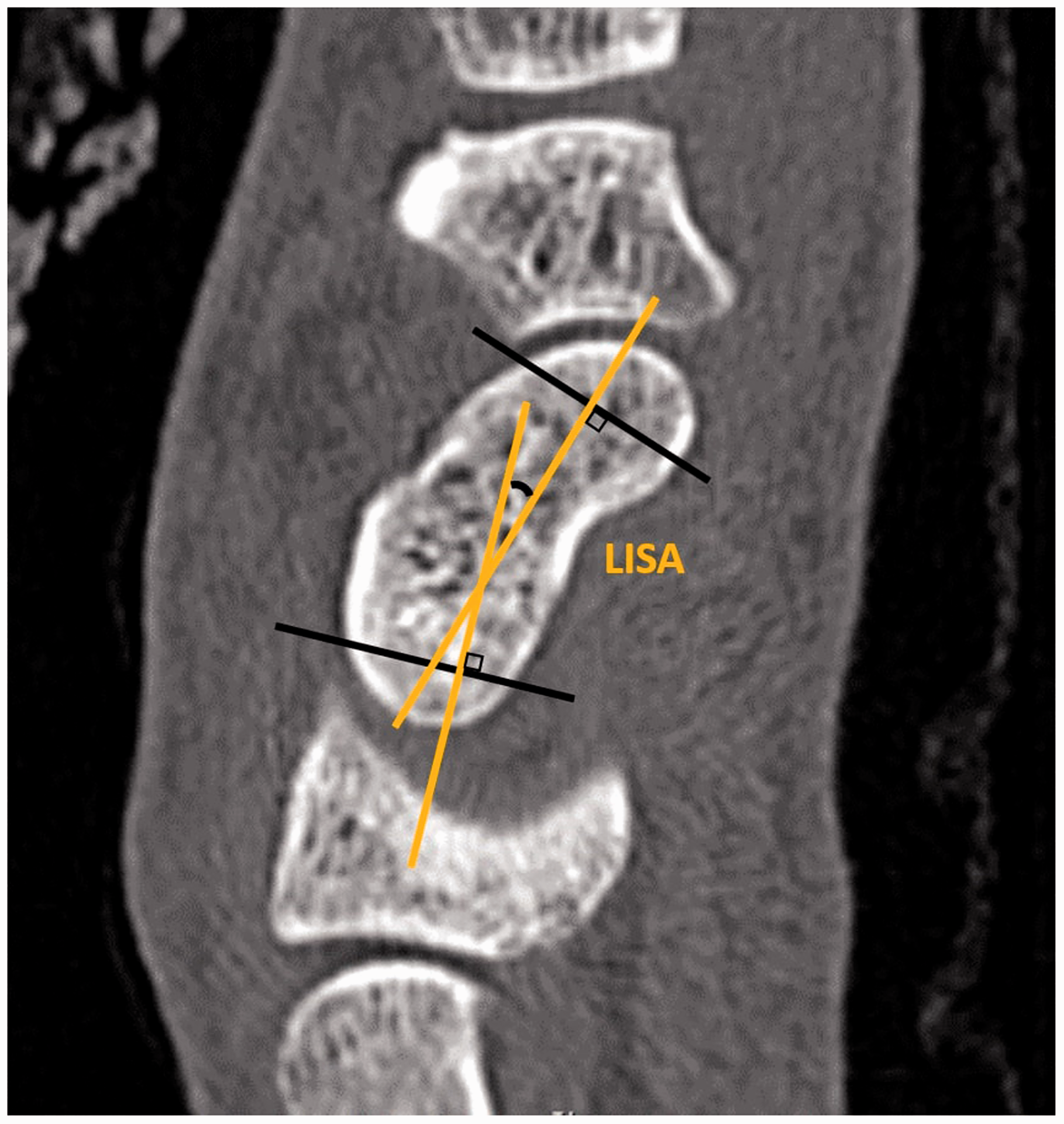
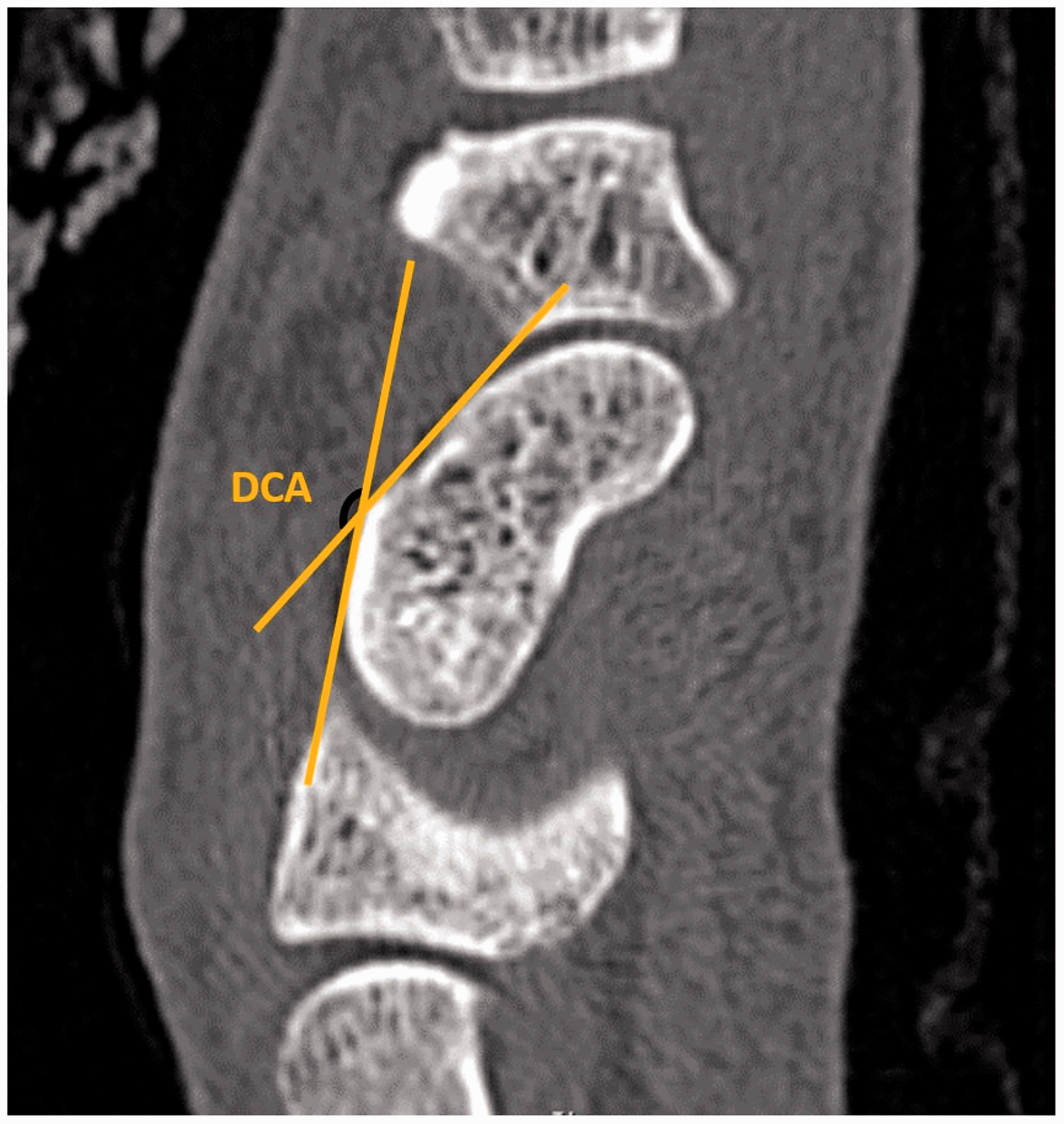
All measurements were made using the IMPAX Client software. The H/L ratio was calculated by dividing scaphoid height by scaphoid length. Scaphoid length was measured from the most proximal to the most distal aspect of the scaphoid using a baseline drawn along the anterior facet. The height was measured using a perpendicular line from the dorsal cortex to the baseline (Figure 1). The LISA was measured according to the previously described method (Amadio et al., 1989) by drawing perpendicular lines drawn on the proximal and distal articular surfaces and measuring the angle between (Figure 2). The DCA was measured as the angle between two tangential lines drawn on the two flattest parts of the dorsal cortex (Figure 3).
The measurement of scaphoid height (H) and scaphoid length (L) from sagittal computed tomography images of the scaphoid. The height–length ratio is calculated by dividing scaphoid height by scaphoid length. The measurement of lateral intrascaphoid angle (LISA) as the acute angle between the yellow lines from sagittal computed tomography images of the scaphoid. The measurement of dorsal cortical angle (DCA) as the obtuse angle between the yellow lines from sagittal computed tomography images of the scaphoid.
Statistical analysis
A statistical power analysis for sample-size estimation was based on previously published data of scaphoid height and length (Bain et al., 1998). This revealed that, in order to identify the minimum possible difference in scaphoid bone length and height between genders, selected as 2 mm, with an alpha of 0.05 and power of 0.95, the required projected sample size was 66. Our study was limited to 62 CT scans owing to the poor quality of scans obtained before 2016, but was considered to be adequate to achieve the main aim of this study. Descriptive values were calculated using measurements from all three observers. Inter- and intra-rater reliabilities were estimated using the intraclass correlation coefficient (ICC), with an ICC <0.49 defined as poor, 0.50–0.74 as moderate, 0.75–0.89 as good and >0.90 as excellent (Koo and Li, 2016). Multiple regression analysis was used to investigate correlations between measurements and gender, hand laterality, age and patient height (if available).
Results
Patient demographics.

If available. NA: not available.
Normal values of radiographic measurements on sagittal CT scans of the scaphoid bone.
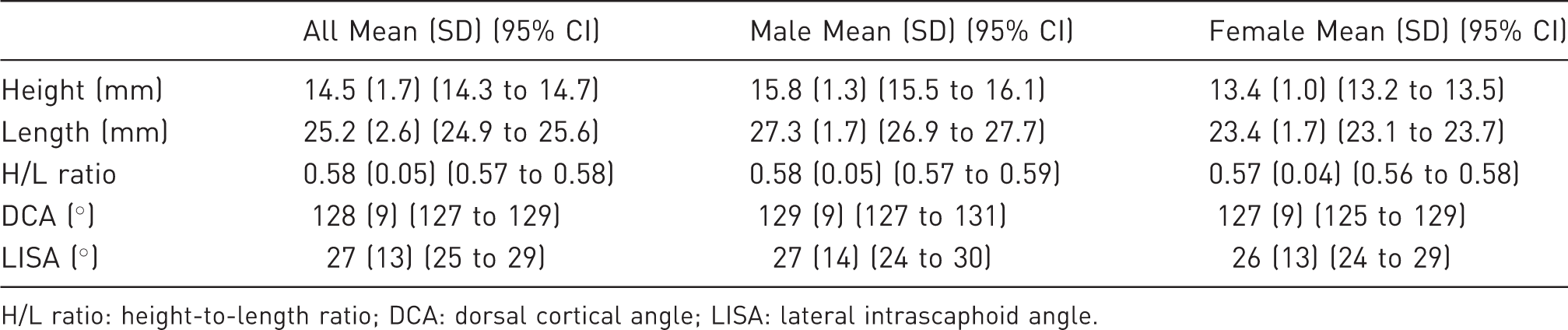
H/L ratio: height-to-length ratio; DCA: dorsal cortical angle; LISA: lateral intrascaphoid angle.
Reliability
Inter- and intra-rater reliabilities.
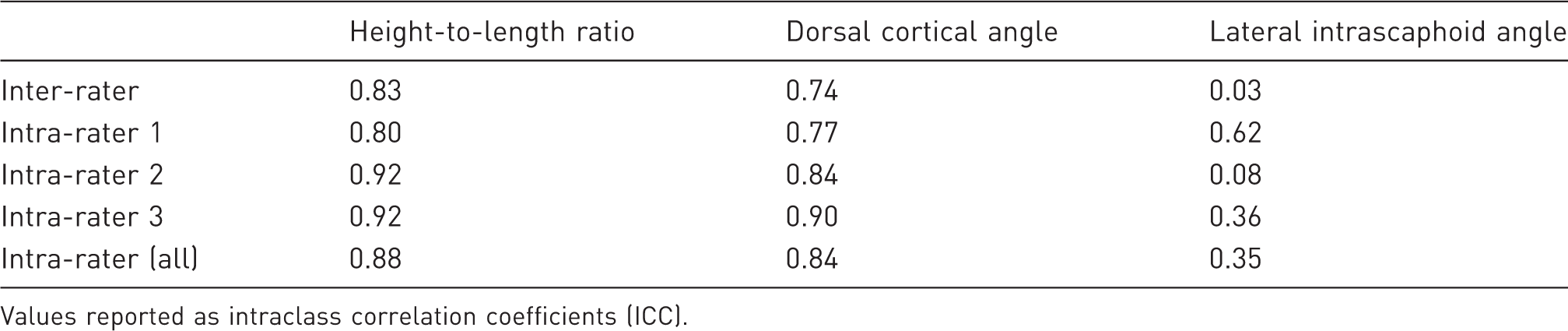
Values reported as intraclass correlation coefficients (ICC).
Discussion
The present study showed a positive correlation between age and scaphoid length suggesting that scaphoid length increases throughout adult life, which could indicate that other parameters of the scaphoid also may change over time. Normal anatomical variations like these contribute to the difficulties in obtaining reliable two-dimensional angular measurements of the scaphoid bone.
Measurements of carpal malalignment, particularly the radiolunate (RL) angle, have been used as indirect assessments of scaphoid malalignment because DISI deformity is frequently observed in scaphoid nonunion (Watanabe, 2011). The RL angle has been reported to be positively correlated with the H/L ratio as well as clinical outcomes (Kim et al., 2016; Megerle et al., 2012) and can be measured reliably (Döring et al., 2016; Larsen et al., 1991; Lee et al., 2018; Vaezi et al., 2017), however measurement of the RL angle is influenced by the position of the wrist on lateral radiographs (Koh et al., 2013). This parameter requires further investigation with regards to scaphoid malalignment; however, we believe that the normal range is well investigated and widely accepted and therefore did not include the RL angle in the present study.
Comparison of measurements from previous studies.
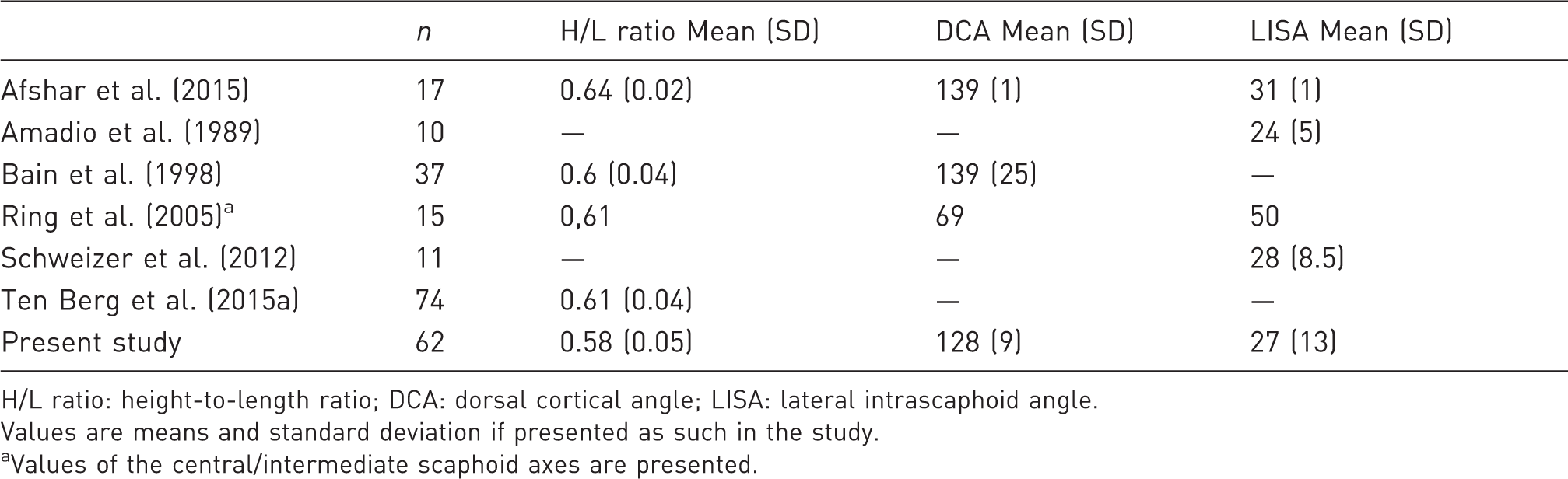
H/L ratio: height-to-length ratio; DCA: dorsal cortical angle; LISA: lateral intrascaphoid angle.
Values are means and standard deviation if presented as such in the study.
Values of the central/intermediate scaphoid axes are presented.
Amadio et al. (1989) was the first to report normal values for the LISA (mean 24° (SD 5°)) from measurement of ten scaphoids on trispiral tomography. Bain et al. (1998) applied this measurement technique to CT scans but normal values for LISA were not obtained due to poor intra- and inter-rater reliability. A confounder of their study was the inclusion of a variety of scaphoid pathologies, which reduces the reliability of the results. Consistent with the study of Bain et al. (1998), we found the inter-rater reliability to be poor and inconsistent for measurements of LISA. Nonetheless, the measurements of the radiologist (DIR) in the present study had a moderate ICC (0.62), suggesting that training may enable sufficient development of skill to obtain more reliable angular measurements as shown previously (Buijze et al., 2012).
We found the measurement of DCA to be more reliable than has been reported previously, with moderate bordering on good inter-rater reliability and good-to-excellent intra-rater reliability. Ring et al. (2005) studied 15 scaphoids and found intra- and inter-rater reliability for DCA to be poor, suggesting that this parameter cannot be measured reliably. However, their study was limited by the small sample size and exclusion criteria were not described. We found DCA to be a reliable measurement technique, but we recommend that angular measurements are always interpreted with care.
This study has some limitations. First, it was a retrospective study, and it was impossible to determine the race of any of the cases. According to The Danish Population Register, the Danish population consists of over 5.8 million people, the majority of whom are Caucasian and approximately 6.1% are mixed races from immigrants and their descendants. Therefore, we can assume that the majority of our cohort were Caucasian. Second, all CT scans were of either the right or left hand, making it impossible to comment on contralateral differences or to determine hand dominance. However, we identified no differences in measurements between the right and left hands, and multiple regression analysis showed no correlation between laterality and any of the measurements suggesting that laterality in itself is of minor significance. A study performed by ten Berg et al. (2015b) involving three-dimensional imaging identified a lack of perfect symmetry between the left and right scaphoids in 19 healthy adults; yet, on average, the articular surfaces of the left and right scaphoids were symmetrically aligned, suggesting that use of the contralateral scaphoid as a reference could be valuable for assessments of scaphoid fracture and malunion.
In summary, this study presents normal ranges for the H/L ratio, LISA and DCA on sagittal CT scans in the long axis of the intact scaphoid. This information may inform decision making and the assessment of malunion. We recommend that the H/L ratio and DCA are used as more reliable measurements, while the LISA should be used and interpreted with caution. Further studies on associations between the H/L ratio and DCA and the clinical outcomes of scaphoid fracture and nonunion are warranted.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Department of Hand Surgery, Herlev/Gentofte University Hospital of Copenhagen to cover the writing assistance expense.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article (Danish Patient Safety Authority, case number 3-3013-2917/1).