
Abstract
Hypothesis:
When the distal fracture fragment in distal radius fractures displaces, it commonly rotates as well as shortens and angulates.
Aim:
The aim of this study was to assess the frequency and magnitude of malrotation of the distal fracture fragment using computed tomography (CT).
Methods:
A retrospective radiological assessment of 85 CT scans of the distal radius, 35 following fracture and 50 normal radii, was carried out. We developed and applied a simple method for measuring rotation of the distal radius relative to the diaphysis using routine CT scans of the wrist. A Mann–Whitney analysis was used to identify differences in radial rotation between fractures and controls. Intra- and inter-observer reliability were analyzed using intra-class correlation coefficients (ICCs) and Bland–Altman plots.
Results:
The articular surface of the distal radius is normally rotated in the long axis of the forearm relative to the diaphysis, either into pronation or into supination. The median radial rotation angle of controls was 1° pronation (range −15° to 4°) compared to 3° pronation (range −24° to 31°) in the fracture group. The absolute rotation angle was significantly greater in the fracture group (median 10°, range 0–31° vs. 3°, range 0–15°; p < 0.001) and outside the “normal range” of controls in 26 cases indicating that 75% had rotated appreciably following injury. Intra- and inter-observer reliability of measurements were good with ICCs of 0.99 and 0.98, respectively.
Conclusions:
Malrotation of the distal radius appears common following distal radius fracture. Malrotation of the distal fracture fragment has been shown to affect distal radio-ulnar joint function. Despite this, rotational deformity is rarely addressed in clinical practice as it is difficult to appreciate on simple radiographs. The simplified method described here is easy to use in routine clinical practice and also appears reliable. Measuring radial rotation may be an important consideration when planning both primary treatment and corrective osteotomy for patients with distal radial malunion.
Introduction
Fractures of the distal radius are very common, 1 –7 with some studies suggesting that there are around 70,000 fractures of the distal forearm per year in the United Kingdom. 2 They occur at all ages, but typically present with a bimodal distribution, with high incidences in children and the elderly people. 1,8,9
Apart from truly undisplaced fractures, all fractures heal with some malalignment. There is debate regarding the degree of malalignment that is “acceptable,” that is, compatible with a sufficiently good outcome not to require surgical stabilization. Nonetheless, within the published literature there is broad agreement about shortening (up to 2 mm), dorsal tilt (up to 10°), and loss of radial inclination (of >10–15°). 10 –15 There are no agreed criteria about how much malrotation is acceptable of the distal fracture fragment relative to the shaft of the distal radius. Malrotation is difficult to assess radiologically and, therefore, is rarely reported. 16 In biomechanical testing malrotation of the distal fracture fragment leads to alterations in distal radio-ulnar joint (DRUJ) biomechanics. 17
Our hypothesis is that malrotation of distal radius fractures is common, but it is not clear whether it is into supination or pronation.
The primary aim of the study was to test the hypothesis that rotational malunion occurs commonly with distal radius fractures and secondarily to establish a simple method for assessing rotation of the distal radius relative to the diaphysis. If the null hypothesis were unproven, we aimed to establish the direction and magnitude of the malrotation and any association with conventional parameters of shortening and angular malalignment.
Methods
Subjects
We conducted a retrospective study of 35 computed tomography (CT) scans of confirmed distal radius fractures (34 patients) and 50 CT scans of wrists with no evidence of a previous distal radius fracture or developmental abnormality (48 patients who either had no fracture identified or had fractures of carpal bones only, e.g. scaphoid fractures) as controls. The patients had presented to our hospital following wrist injuries and had CT scans performed at the request of clinicians in the emergency department or fracture clinic or by their general practitioner, between 1 January 2011 and 30 January 2018.
The inclusion criteria were the following:
Fracture group: CT scans for any patient who had undergone CT scanning of their wrist(s), in which there was a confirmed distal radius fracture or malunion following a fracture (the fracture could be intra- or extra-articular, comminuted, or simple providing there was sufficient structural integrity to assess the alignment of the distal fracture fragment).
Control group: CT scans of wrists of patients with no evidence of a previous bony injury or developmental abnormality of the distal radius.
The exclusion criteria were the following:
Repeat CT scans of the same wrist (although CT scans of bilateral wrists were included).
CT scans, which did not include enough of the radius to assess the area of flattening of the volar cortex to allow proximal angle measurement (this mostly applied to the control group).
Fractures with metal fixation present, for example, plates and screws or Kirschner wires.
Highly comminuted fractures, where the comminution extended into the diaphysis, thus preventing meaningful measurement of the proximal angle (including some Muller AO C2 and C3 fractures, in which the flat volar metaphyseal cortex was too damaged for accurate assessment).
Isolated radial styloid fractures.
CT scanning
CT scans were performed with the forearms in neutral rotation using a Siemens Definition Edge CT scanner (Siemens Healthcare GmbH, 92052 Erlangen, Germany). Images were obtained in the axial plane with 1 mm slice thickness extending to approximately 3 cm proximal to the fracture. Acquisition parameters were as follows: 120 kV, 120 mA with 0.28-s rotation time. Both bone windows (W 2000 HU; L 250HU) and soft tissues windows (W350 HU; L 50 HU) were displayed. Coronal and sagittal reconstructions were then performed.
Calculation of rotational deformity
The method for calculation of rotational deformity was adapted from Frahm et al. 18 and Prommersberger et al. 16 Our method involved identifying the first axial image proximal to the radio-carpal joint. The midpoint of the sigmoid notch was identified, and a line was drawn between this and the most radial cortex of the distal radius, that is, at the radial styloid (Figure 1(a)). A second line was drawn horizontally across the image and the angle between the two lines was determined using the angle measurement function on the picture archiving and communications system (PACS) system. This was defined as the distal angle (Figure 1(a)). The first axial image demonstrating the flattening of the volar surface of the radius as the scans moved proximally up the forearm from the distal radius was taken for the proximal angle measurement. This was typically 2–3 cm proximal to the proximal end of the DRUJ. A line was drawn tangential to the flattened volar cortical surface of the radius (Figure 1(b)). Again, a horizontal reference line was drawn and the angle between the two lines was determined. The difference between the proximal and distal angles was calculated as the radial rotation angle (RRA); it was recorded as either supination (positive values) or pronation (negative values).
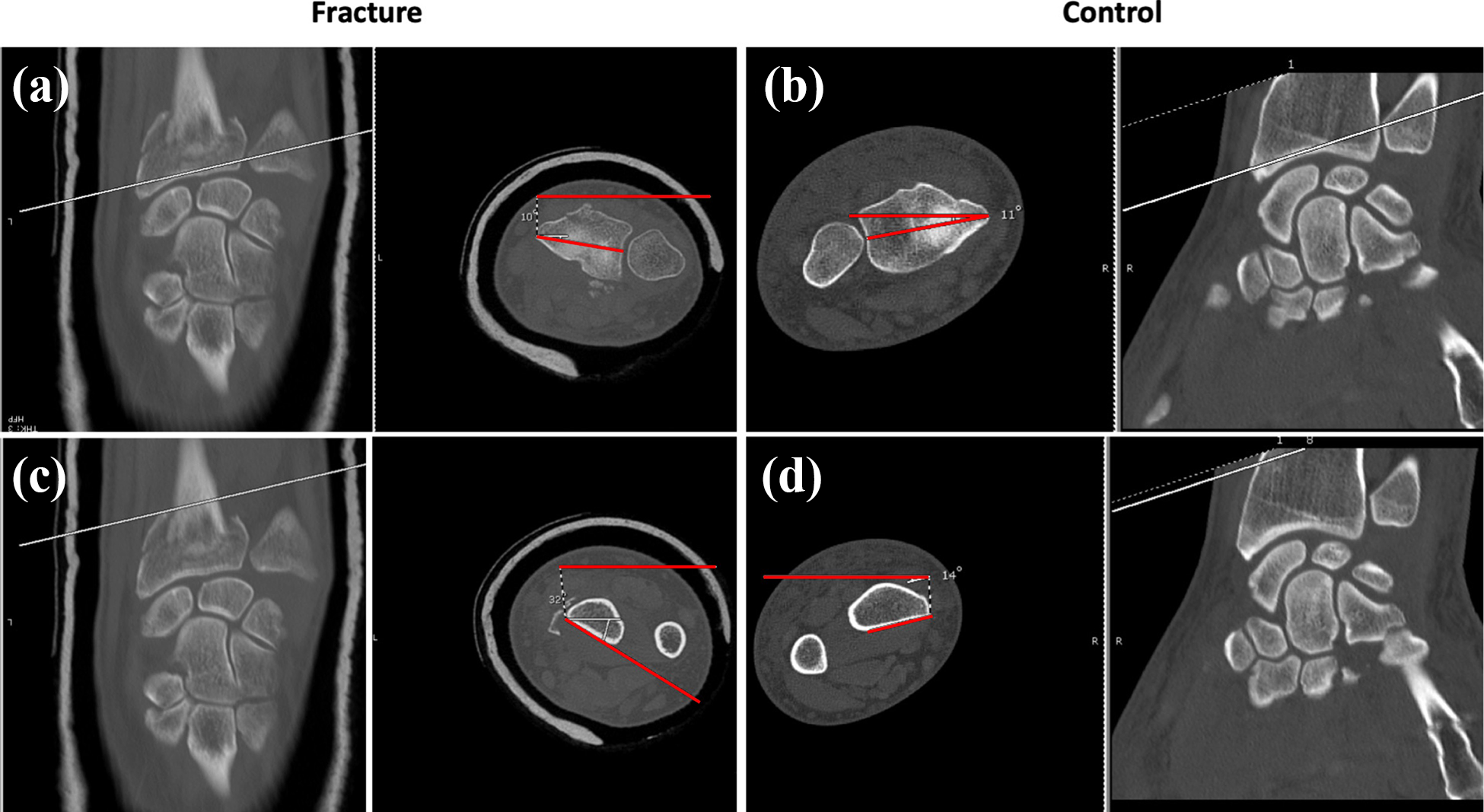
Measurement of (a, b) distal and (c, d) proximal angles of the distal radius for calculating radial rotation angle on both fractured (a, c) and normal (b, d) distal radii.
The images were analyzed by two independent observers using Fujifilm’s synapse PACS software. Intra- and inter-observer variabilities were determined by comparing blinded, repeat measurements of a subset of ten scans. The scans were selected at random and remeasured at least 1 week apart. The data were recorded using Microsoft Excel spreadsheets.
Statistical analyses
Statistical analyses were performed with Prism 7.0 for Mac OS X (GraphPad® Software, 2012) and SPSS® Statistics Version 25 (IBM® Software, 2018).
The difference in absolute rotation angle of the distal radius (i.e. irrespective of direction of rotation) between those with fractures of the distal radius and controls was analyzed using the Mann–Whitney test. Results were considered to be statistically significant if p < 0.05.
For intra- and inter-observer reliability the intra-class correlation coefficients (ICC, one- and two-way random-effect models) were calculated. An ICC of greater than 0.80 was considered to be acceptable. 19 This was supplemented by visual inspection of Bland–Altman plots, showing the difference between two measurements against their mean. Reliability is indicated visually with at least 95% of all dots being within the upper and lower limits of agreement. 20,21
This study was undertaken with the approval of the hospital research and audit committee.
Results
Demographics
The two groups of patients were similar for age and gender, with roughly equal numbers of right and left wrists in both groups. The mean ages of the patients with distal radius fractures was 50 (range 21–79) years compared to 42 (range 15–82) years for controls. Both groups had similar proportions of men (54 and 56%) and women (46 and 44%). The proportion of right and left wrists studied within the groups was also comparable (Table 1).
Study group characteristics.
SD: standard deviation.
A number of fracture patterns were evident within the fracture group. The majority (77%) were intra-articular with some comminution (AO B3, C1-3), while the remainder were extra-articular (AO A2–3).
Radial rotation angle
Inspection of the data revealed that the RRA could be a negative value (representing pronation of the distal epiphysis relative to the metaphysis) or a positive value (representing supination of the epiphysis). In the fracture group, 13 (37%) of the subjects had a supination rotational angle (with a mean angle of 8.9°) and 21 (60%) had a pronation rotational angle (with a mean angle of 12°). The remaining subject was neutral (0°). The control group supinated in 18 (36%; with a mean angle of 2.3°), pronated in 26 (52%; with a mean angle of 4.2°) and were neutral in 6 (12%) (Figure 2). The χ 2 analysis did not find any statistically significant relationship between the presence or absence of a fracture and the direction of RRA (χ 2 = 2.34; df = 2; p = 0.311).

Proportion of radial rotation angles that were neutral, pronated, or supinated in each study group.
In the control group, 90% of angles (irrespective of direction) were less than or equal to 5°. Using 5° as a cutoff, 26 of the fractures (75%) had supination or pronation angles outside this.
The median RRA was −3° (range −24° to 31°, mean 3.9°), that is, the distal radius pronated relative to the diaphysis, in the fracture group compared to −1° (range −15° to 4°, mean 1.4°) in the control group. The absolute (i.e. irrespective of direction) RRA was 10° (range 0–31°, mean 10.5) in the fracture group compared to 3° (range 0–15°, mean 3.02) in the control group. A Mann–Whitney U test indicated that the RRA was significantly greater in the fracture group (mean rank 59.67) than in the control group (mean rank 31.33), U = 291.50, z = −5.21, p < 0.001 (Figure 3).
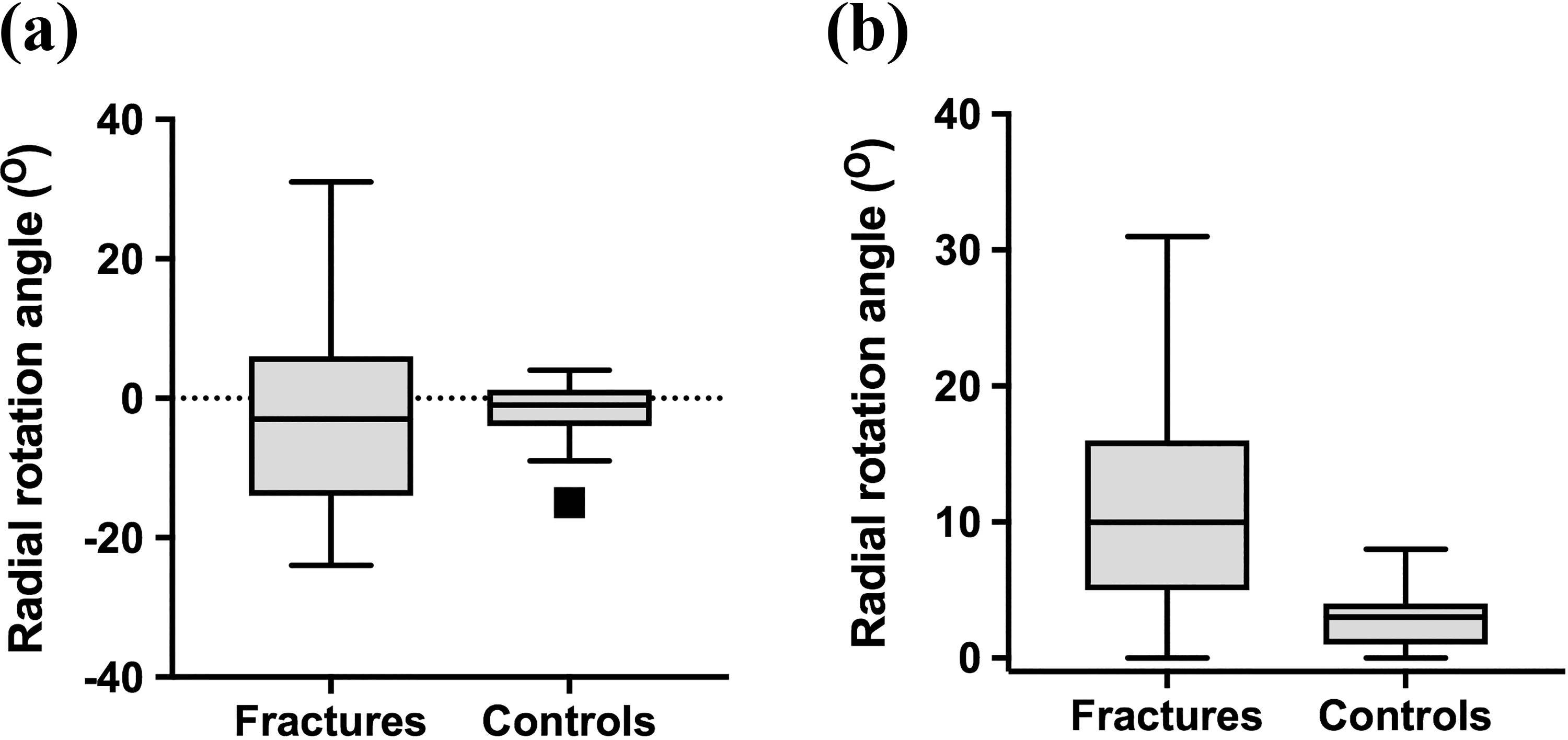
Box and whisker plots depicting the radial rotation angle for patients with distal radius fractures and control subjects without distal radius fractures. The central box represents the interquartile range (25th to 75th), with the median represented by the middle line. The whiskers represent the minimum and maximum values. (a) Raw rotation angle. (b) Absolute rotation angle (irrespective of direction, i.e. magnitude of rotation).
Radiological variables including radial height, radial inclination, and volar tilt were evaluated by multiple regression analysis to explore their relationship with radial rotation. In this sample, no correlations were found between the variables.
Reliability of measurement method
The intra-observer ICC was 0.996 (95% CI 0.985–0.999), which shows a statistically significant agreement between repeated measurements performed by the same individual on separate occasions (p < 0.0001). This was also confirmed visually using a Bland–Altman plot, showing that all data points fell within the 95% limits of agreement (Figure 4(a)).
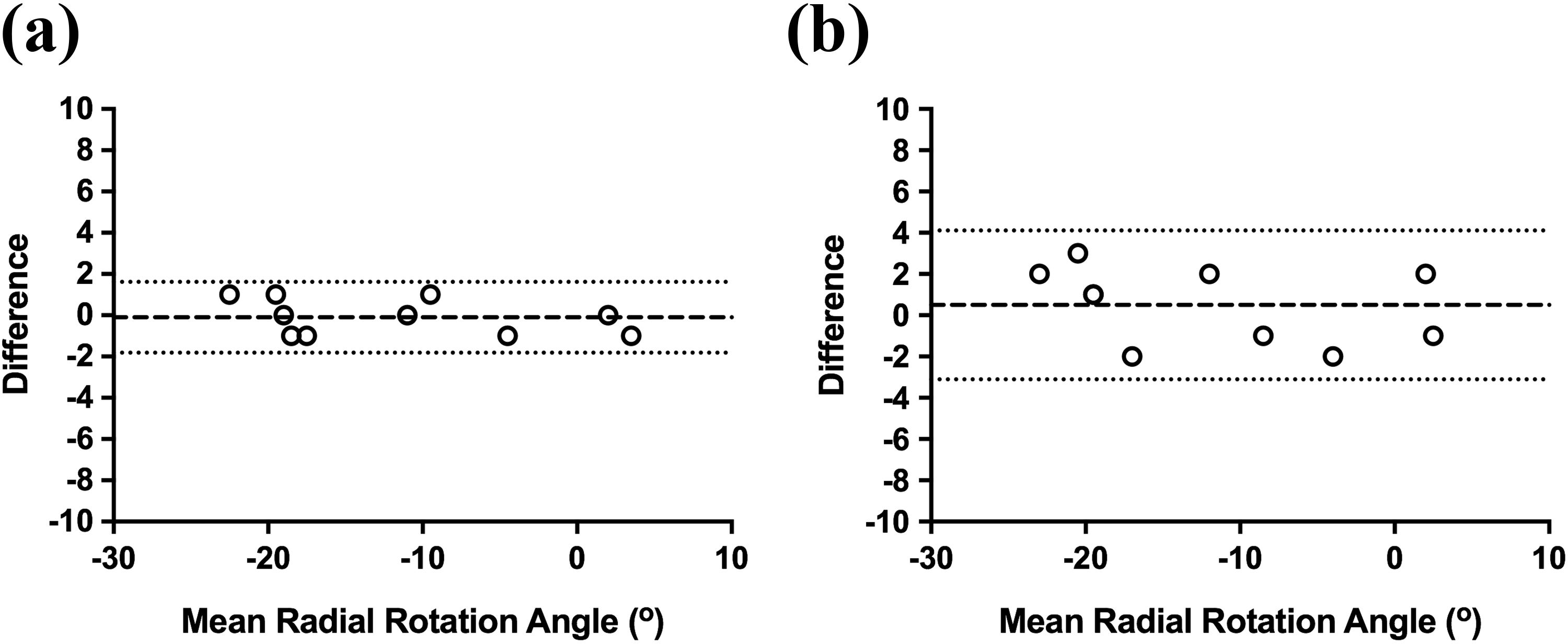
Bland–Altman plots for (a) intra-observer and (b) inter-observer reliability of measuring radial rotation angle.
The inter-observer ICC was 0.981 (95% CI 0.927–0.995), which shows statistically significant agreement between measurements performed by different individuals on separate occasions (p < 0.0001). This was also confirmed visually using a Bland–Atman plot, again showing that all data points fell within the 95% limits of agreement (Figure 4(b)).
Discussion
This study has demonstrated that rotational deformity is very common in displaced fractures of the distal radius. Rotational deformity can be difficult to measure on simple radiographs but should be considered in addition to volar tilt, radial inclination, and shortening. This is likely to be important as studies have shown that distal radius malunion can be associated with a reduction in forearm rotation. 16,17 In our study, 26 of the 35 subjects (74%) in the fracture group had a rotational deformity. This finding fits with previous similar studies, such as that of Prommersberger et al. 16 who found that 23 of the 37 distal radius malunions had a rotational deformity.
Hayes et al. 22 also found similar results, demonstrating that patients with previous distal radius fractures had a significantly larger radial torsion angle than healthy controls (49.3° in the fracture group vs. 36.7° in the control group). In our study, we found that RRA was also significantly larger in the fracture group when compared to the control group (median angle 10° vs. 3° for controls). Prommersberger et al. 16 also found a range of mean radial rotational deformities between 10° and 14° in their study of distal radius malunions. The differences in radial torsion angles found between our study and that of Hayes et al. 22 could be explained by the use of different measurement methods that were used to calculate the radial rotational deformity.
The method used in this study is adapted from that developed by Frahm et al. 18 In their method they created a single “fusion image” from the two axial CT slices, which is complex. This method is much easier to apply to standard CT scans taken in routine clinical practice. By using a referencing line, there was also no need for standard positioning of the patient’s forearm and wrist in the scanner. Other methods of measuring rotational deformity such as those described by Bindra et al. 23 and Bade et al. 24 and used in the study of Hayes et al. 22 involve measurement of both the proximal and the distal radius. The method used in this study requires scans of much less of the injured wrist, with no requirement to scan the proximal forearm. This results in less radiation exposure to the patient and is more cost-efficient.
Any method for measurement of radial rotational deformity must be reliable and easy to reproduce. The high levels of intra- and inter-observer reliability found in this study show that the method used is reliable and easy to reproduce. This high level of intra- and inter-observer reliability is similar to that of the methods currently used for measuring radial rotation profiles. 23,25,26 The big advantage is that it is applicable to standard CT scan imaging without extended imaging or costly and complex digital reconstructions.
This study has its limitations, including the lack of bilateral wrist CT scans to provide a side-to-side comparison. Many previous studies have found variation in radial torsion angle among individuals but limited variation between sides of the same individual. 22,23,26,27 Despite this, a study by Dumont et al. 25 noted some intra-individual side-to-side variation in normal volunteers, indicating that side-to-side comparison may not be as robust as originally believed. The lack of side-to-side comparison in the present retrospective study prevents us from assessing this.
The number of subjects is small with only 35 subjects and 50 controls. Larger studies with greater numbers of subjects may help to reduce the influence of outliers or extreme observations and be more representative of the population. As this was a retrospective study, it was not possible to collect data concerning the forearm ranges of motion and thus the effect of the deformities upon supination and pronation. However, previous studies have identified the impact of rotational deformity of the radius on forearm rotation. 16,17 The measurement method may not be applicable to assess rotational deformity in highly comminuted distal radius fractures including some Muller AO C2 and C3 fractures, which disrupt the flat volar metaphyseal surface used for measurement of the proximal angle.
Finally, the scans of the injured wrists were not performed randomly for patients with any distal radius fracture, that is, there is potential bias that rotational abnormalities may be more common in this group of patients who required a CT scan.
Conclusions
Despite the limitations of this study, it is evident that malrotation of the distal radius following fracture is common, but frequently overlooked in clinical practice not least as it is very difficult to measure on standard radiographs. We have developed a new, simple, and reliable method for assessing rotation of the distal fracture fragment on standard CT scan images without the need for proscribed positioning or analysis with complex software. When managing patients with distal radius malunion, the radial rotational deformity identified using this method may be an important consideration when planning corrective osteotomy to improve outcomes for patients. Consideration of radial rotation deformity may also be beneficial in optimizing the reduction and stabilization of distal radius fractures to minimize symptoms from malunion.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.