
Abstract
Selective denervation of sensory nerve branches to the wrist is a palliative surgical treatment option for patients with chronic wrist pain when preserving the range of motion and function is preferred. Treatment varies from partial isolated denervation of the posterior interosseous nerve to extensive ‘complete’ denervations. This study aimed to provide an overview of the literature regarding treatment outcomes in the domains of pain, grip strength, patient satisfaction and return to work. MEDLINE (PubMed), EMBASE and Cochrane databases were systematically searched and identified 993 studies, of which 12 were eligible for analysis. Denervation resulted in high ‘return to work’ rates (up to 94%), patient satisfaction (up to 92%), increased grip strength (7%–64%) and improved average pain scores (36%–92%). Treatment outcomes of both partial and complete denervations were favourable; however, variations in outcomes suggest the need for improving evidence regarding surgical technique and nerve identification.
Keywords
Introduction
Chronic pain in the hand and wrist is a common problem. In the UK, the prevalence of chronic (>3 months) pain was present in 13% of the surveyed population who had pain in multiple locations in the hand or wrist (Carnes et al., 2007). Patients eligible for denervation should have chronic wrist pain (>3 months) and be skeletally mature (Hofmeister et al., 2006). This procedure is a palliative option when preservation of the range of motion and function are preferred and conservative treatment has been inadequate (Hofmeister et al., 2006; Le Nen et al., 2011).
Denervation techniques of the wrist have been modified over the years from Wilhelm’s ‘complete’ denervation in 1959 (Wilhelm, 2001) to less invasive ‘partial’ denervation using only a single incision (Berger, 1998; Grechenig et al., 2017). Partial denervation focuses on specific articular nerves, especially the anterior interosseous nerve (AIN) and posterior interosseous nerve (PIN). To determine the potential effect of denervation, the patient’s response to a preoperative anaesthetic nerve block has been evaluated (Hofmeister et al., 2006; Ishida et al., 1993; Riches et al., 2016; Storey et al., 2011). However, other authors refrain from using diagnostic blocks because the analgesic response after the local block poorly correlated with the postoperative change in pain scores (Patil and Arenas-Prat, 2016; Weinstein and Berger, 2002). Surgical scarring, incomplete surgical denervation and/or re-innervation of the joint may lead to reduced pain reduction. Furthermore, the local analgesic might spread to smaller terminal nerve branches to the wrist joint that are not divided during surgery. The procedure is contraindicated in chronic conditions that are still treatable with conservative methods and in a dysfunctional joint due to a structural deformity (Hofmeister et al., 2006; Patil and Arenas-Prat, 2016).
We systematically reviewed the literature describing therapeutic effects of nerve denervation in the domains of wrist pain, grip strength, patient satisfaction and return to work (RTW).
Methods
Literature search
A systematic search of the available literature in MEDLINE using PubMed, EMBASE and Cochrane CENTRAL databases was performed in March of 2019. In PubMed, the title and abstract (tiab) and medical subject headings (MeSH Terms) were added to the keywords of the search to expand the scope of the search. For EMBASE, the title (ti) and abstracts (ab) and further keywords (kw) were also added to the primary search terms that were used for the queries. The primary search terms included ‘wrist’, ‘denervation’, ‘neurectomy’, ‘neurotomy’, ‘nerve tissue’, ‘anterior interosseous nerve’ and ‘posterior interosseous nerve’. A search for additional trials was done in Cochrane CENTRAL. The complete search strategy is provided in the supplementary data (Table S1; Appendix S1). References in selected studies were screened for eligibility.
Inclusion and exclusion criteria
All clinical studies with their own patient cohort reporting outcomes on both complete and/or partial wrist denervation techniques on chronic wrist pain, regardless of the origin of the pain, were included. There was no limit for publication date. Non-English studies and studies on patients who underwent concomitant surgical procedures were excluded. Studies containing both patients with and without concomitant procedures were only included if the treatment and outcomes of the ‘denervation only’ group was reported separately.
Selection procedure
All studies from the search were screened on title and abstract for eligibility for analysis by two independent assessors (KC and AE) using an online referencing tool (Ouzzani et al., 2016). After selection based on title and abstract, full texts were screened for relevance of outcomes. In case of disagreement, both assessors discussed the eligibility of the study with the senior author (SS) acting as a referee until consensus was reached on final inclusion or exclusion.
Quality of selected studies
Guidelines from the Oxford Centre for Evidence-Based Medicine (CEBM) were followed to assess the quality of the included studies. Furthermore, the online GRADEpro Guideline Development Tool (McMaster University/Evidence Prime Inc., Hamilton, Ontario, Canada) was used to give an overall indication of the risk of bias and quality of the included studies according to guidelines set by the Cochrane Handbook for each outcome measure discussed.
Outcomes
Full text manuscripts were screened to obtain the detailed patient characteristics including age, follow-up time and denervation technique. The primary outcome was postoperative pain using the visual analogue scale (VAS) on a 0–10 (or 0–100) scale or pre- and postoperative grip strength (in kilograms). Secondary outcomes included, ‘return to work’ (RTW) rate, patient satisfaction and patient recommendation rates.
Results
Study selection
The literature search yielded a total of 993 studies (Figure 1). After removing duplicates, screening titles and abstracts, 969 studies were excluded from further analysis. After screening full texts of 24 studies, another 12 studies were excluded based on incomplete presentation of outcomes, such as the absence of both pre- and postoperative VAS scores or grip strength outcomes. Results from 12 studies were included for analysis (Table 1).
PRISMA flowchart of the screening process in PubMed (MEDLINE) and EMBASE. Overview of selected studies and their levels of evidence according to the CEBM guideline. CEBM: Centre for Evidence-Based Medicine; AIN: anterior interosseous nerve; PIN: posterior interosseous nerve; SLAC: scapholunate advanced collapse; SNAC: scaphoid nonunion advanced collapse; RC: radiocarpal; OA: osteoarthritis; Kienböck’s: Kienböck’s disease; DRUJ: distal radio-ulnar joint; STTJ: scaphotrapezotrapezoidal joint; SR: scaphoradial; TTFC: triangular fibrocartilage complex; CRPS: chronic regional pain syndrome; SL: scapholunate; Level II of evidence: prospective cohort, comparative study; Level IV of evidence: retrospective case series, no control group.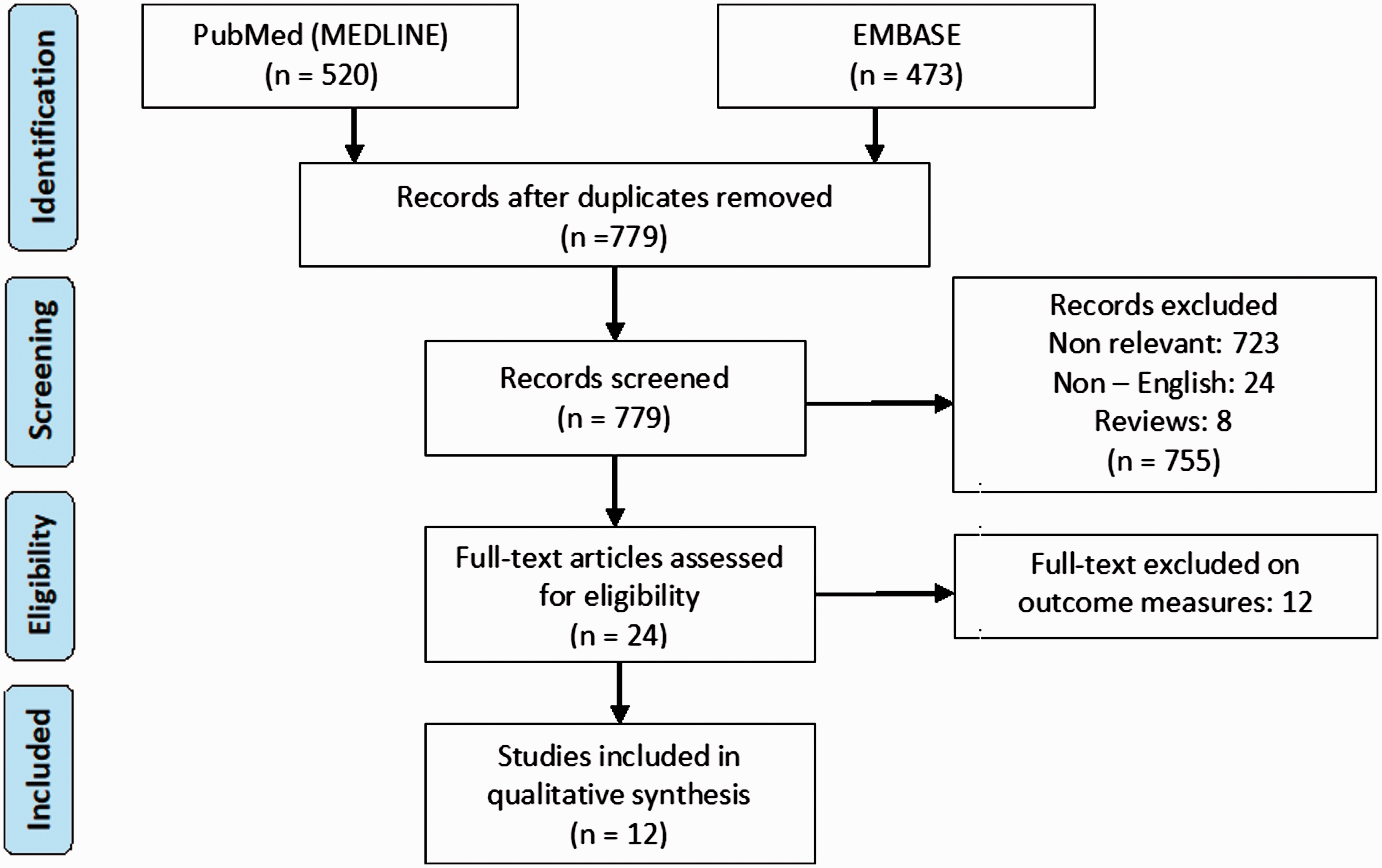
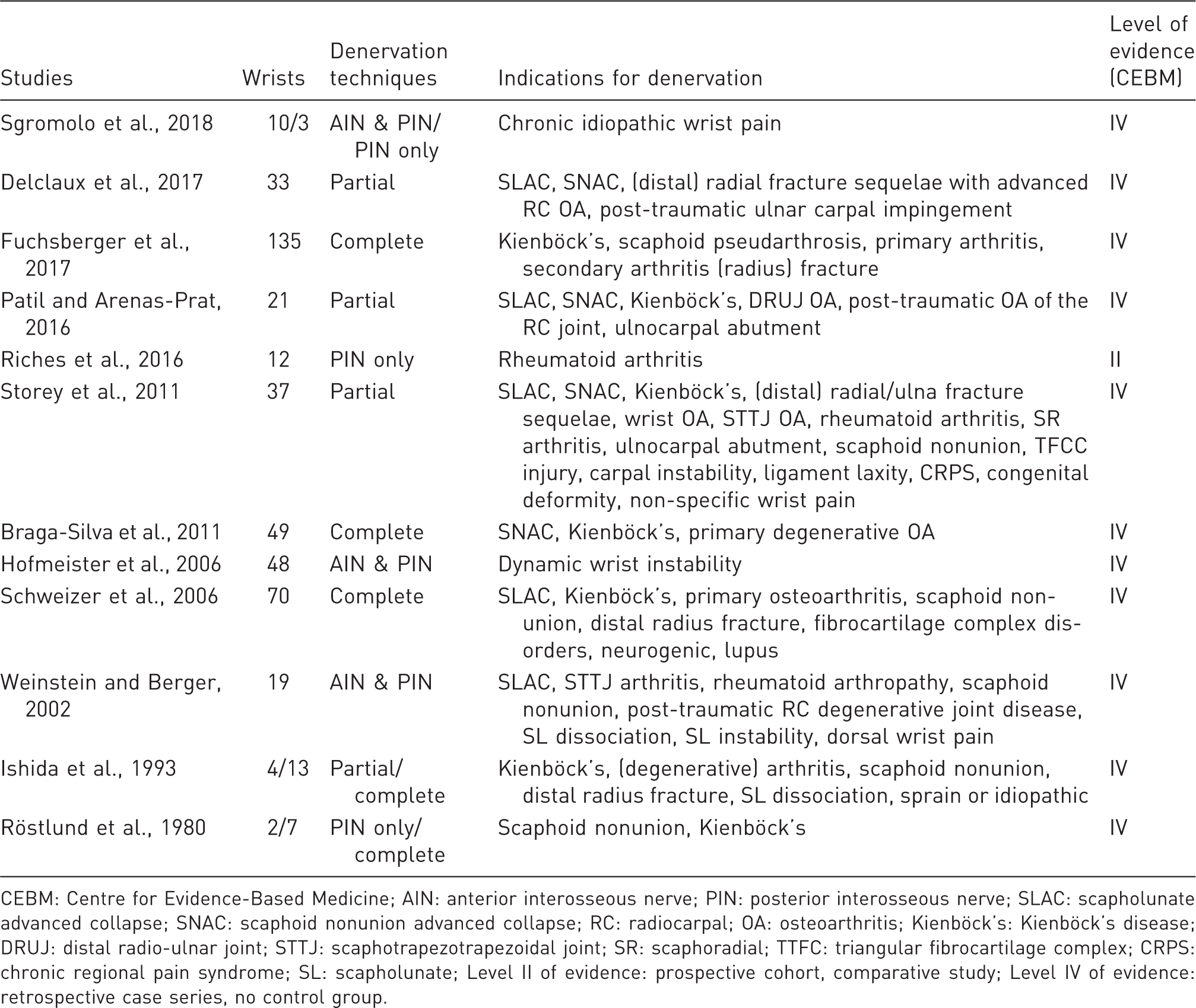
Indications for selective denervation
The 12 included studies reported a range of conditions for which patients were treated with selective denervations. These are summarized in Table 1.
Surgical techniques for selective denervation
The studies included can be subdivided according to surgical technique; (modified) complete denervation techniques and less invasive partial denervations (Table 1) (Berger, 1998; Wilhelm, 1965, 2001). The complete denervation, according to Wilhelm, targets the PIN, articular branch of the first interosseous space, articular branches of the lateral antebrachial cutaneous nerve, articular branch of the superficial radial nerve, articular fibres of the palmar branch of the median nerve, articular fibres of the AIN, perforating fibres of the deep branch of the ulnar nerve, articular fibres of the dorsal branch of the ulnar nerve and the articular branch of the posterior antebrachial cutaneous nerve. Variations of Wilhelm’s technique are targeting a number of the aforementioned nerves. The partial denervation techniques can be subdivided in resection of only the PIN (PIN only), the AIN and PIN (AIN & PIN), or the aforementioned combined with resection of, for example, cutaneous branches of the radial and/or median nerve (partial) (Delclaux et al., 2017; Patil and Arenas-Prat, 2016; Storey et al., 2011).
Pre- and postoperative pain scores
Overview of studies publishing pre- and postoperative pain scores according to the VAS.
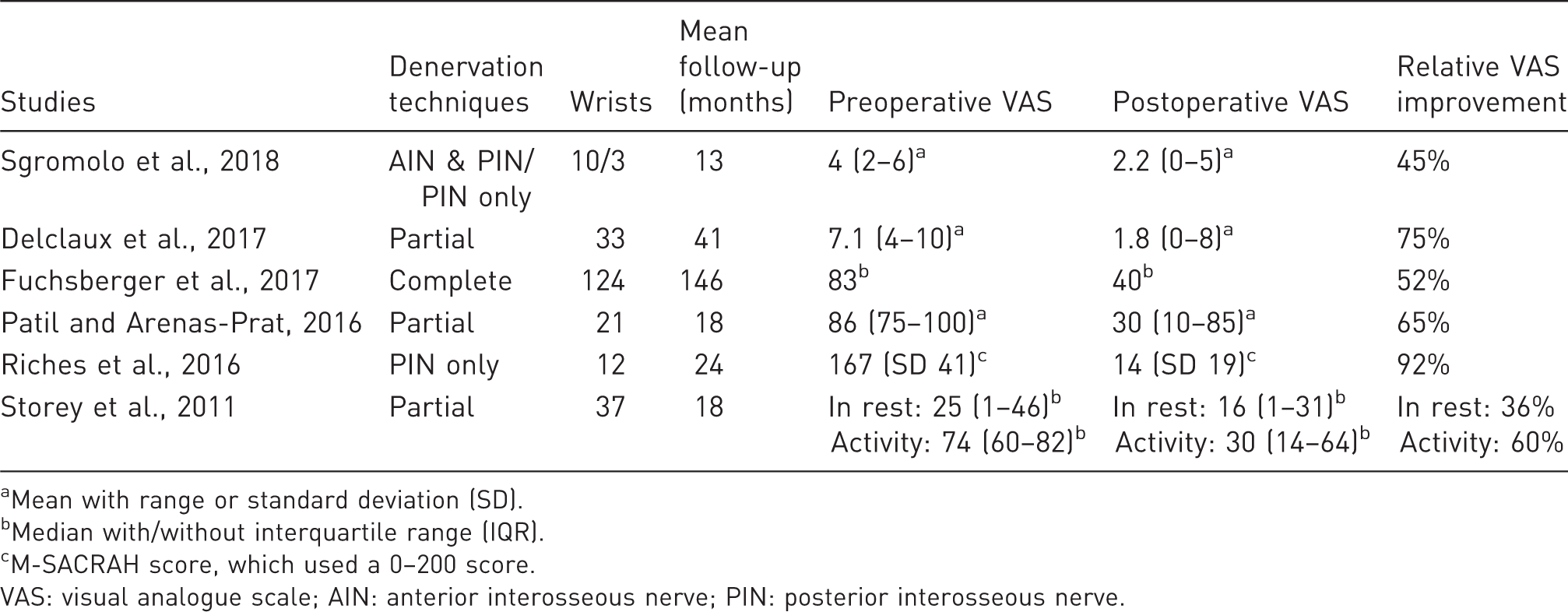
Mean with range or standard deviation (SD).
Median with/without interquartile range (IQR).
M-SACRAH score, which used a 0–200 score.
VAS: visual analogue scale; AIN: anterior interosseous nerve; PIN: posterior interosseous nerve.
Grip strength
Overview of studies reporting grip strength.
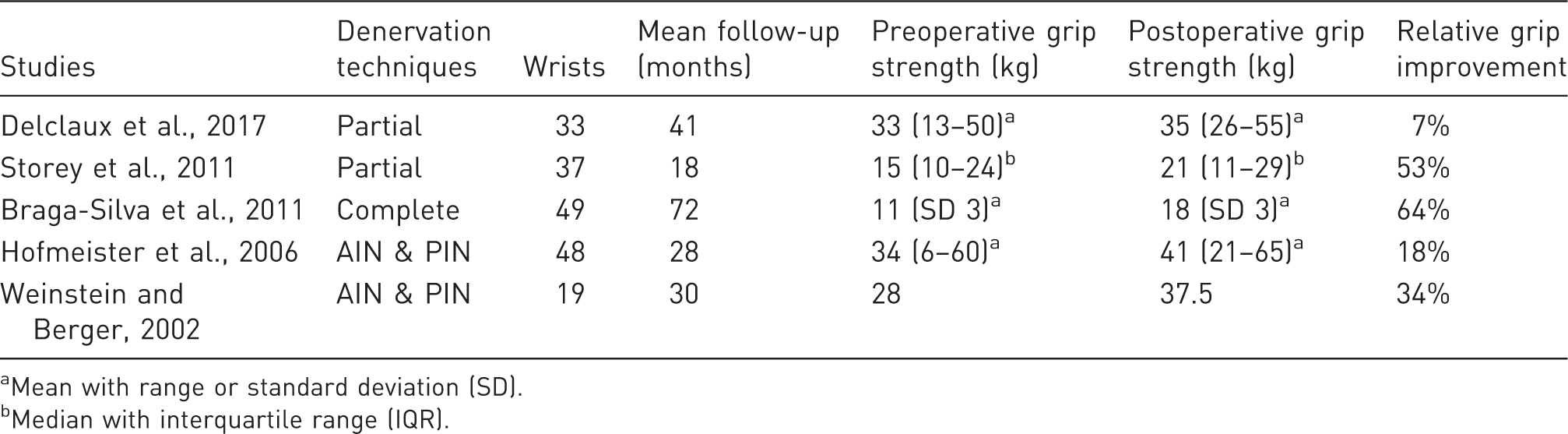
Mean with range or standard deviation (SD).
Median with interquartile range (IQR).
Return to work
Overview of studies reporting return to work rate.
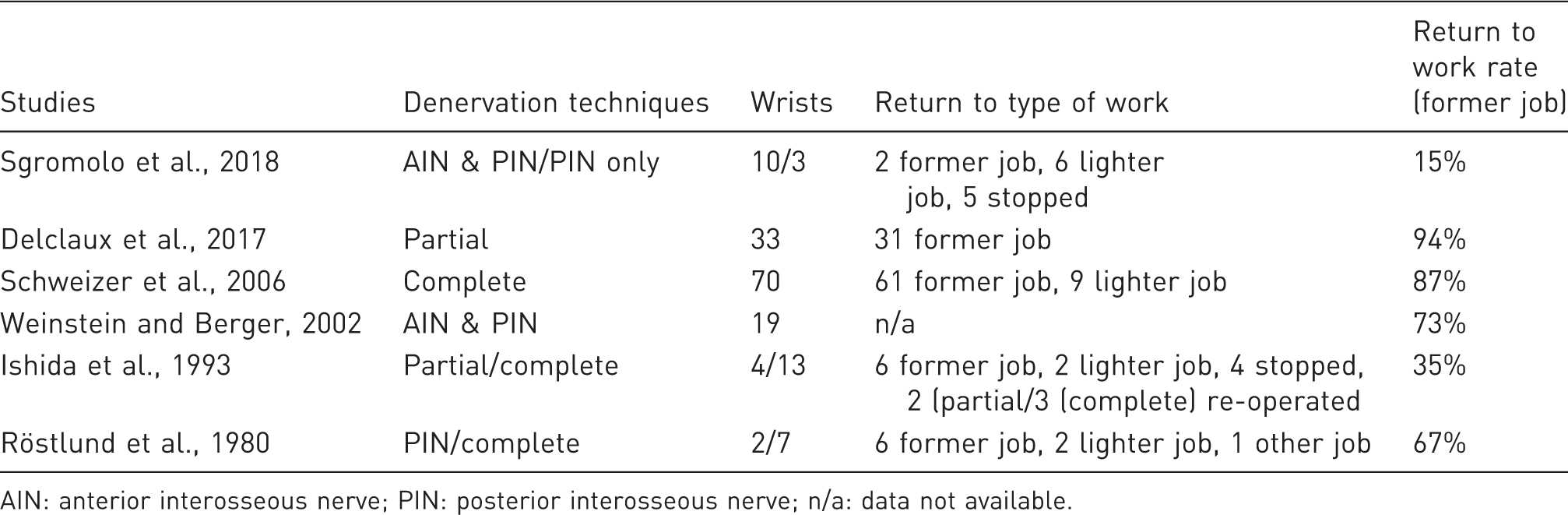
AIN: anterior interosseous nerve; PIN: posterior interosseous nerve; n/a: data not available.
Patient satisfaction
Overview of studies reporting patient satisfaction and recommendation rates.
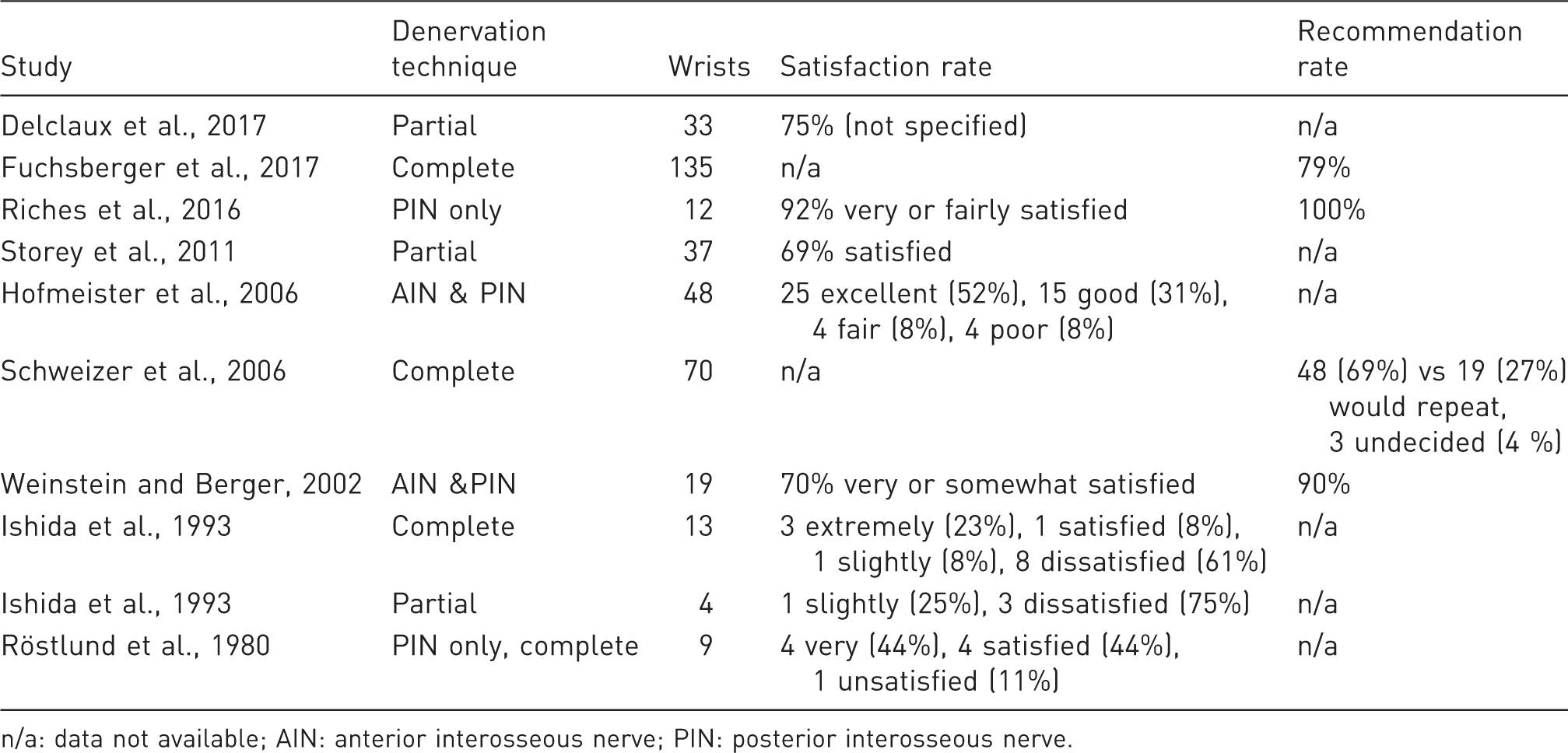
n/a: data not available; AIN: anterior interosseous nerve; PIN: posterior interosseous nerve.
Complications and re-operations
Postoperative complication rates, including re-operations (including permanent interventions, e.g. proximal row carpectomy) and persistent or worse pain, varied from 6% to 29% (Delclaux et al., 2017; Hofmeister et al., 2006; Storey et al., 2011; Weinstein and Berger, 2002). In the cohort of Ishida et al. (1993), two out of four partial denervation patients needed additional surgery due to persistent pain, in contrast to the three out of 13 complete denervation patients. Using a partial denervation technique, Delclaux et al. (2017) reported persisting dysesthesia in 21% of patients, of which one patient developed a complex regional pain syndrome. Neuromas in 8% of patients and transient hypoesthesia were described anecdotally (Braga-Silva et al., 2011).
Denervation versus other surgical techniques
In 2016 Riches et al. published a prospective series of 94 patients with rheumatoid arthritis (RA) with a mean follow-up time of 3 years (Riches et al., 2016). These patients underwent one of eight surgical procedures (Swanson’s arthroplasty, wrist arthrodesis, carpal tunnel decompression, RA nodule excision, synovectomy/tenosynovectomy, tendon repair/release and PIN denervation). The 12 patients who underwent PIN denervation did not differ significantly in terms of pain and functional recovery as compared with the other procedures.
Discussion
All studies showed reduction in reported VAS pain scores postoperatively as a result of denervation. Only two studies reported reduction in pain at rest and pain during activity separately (Delclaux et al., 2017; Storey et al., 2011), and both reported an improvement in both domains. Patients with longer follow-up times after denervation tended to benefit less from denervation (Ferreres et al., 1995; Fuchsberger et al., 2017; Röstlund et al., 1980). Progression of the underlying condition could have caused the pain to increase and/or limit the function of the wrist joint (Dellon, 1985). However, with the limited numbers of studies available, we were unable to conclude whether a complete denervation results in better long-term results compared with partial techniques or vice versa. To objectively assess the impact on the patients’ well-being, whether positive or negative, the preferred outcome measure for pain is the VAS. Our search only yielded six studies in English in which the VAS was described on a scale of 0–10 or 0–100 (Table 2). In the remaining six studies, only relative changes in pre- and postoperative VAS were reported. The relative VAS improvement of the isolated PIN (PIN only) denervation by Riches et al. (2016) is higher than the other more extensive partial denervation techniques, however, that score is the result of the MSACRAH, which uses a combined pain score of the VAS during activity and in rest is used in contrast to most of the other studies (Table 2). It is unclear whether this explains the relatively high VAS improvement of Riches et al. (2016). The partial denervation studies show an overall higher trend in improvement compared with the complete denervation study of Fuchsberger et al. (2017).
Grip strength was increased after denervation overall, however a relative decrease has also been reported (Röstlund et al., 1980), but this was not included in Table 2, as only a relative difference was described in that report. Grip strength improved the most after complete denervation (Braga-Silva et al., 2011). A factor is that the mean preoperative grip strength in the cohort of Braga-Silva et al. (2011) is lower compared with the other studies, therefore a similar increase in absolute grip strength resulted in a higher relative improvement in grip strength. Patient satisfaction was generally high after denervation in both the complete and partial denervation groups. The partial denervation group of Storey et al. (2011) and Ishida et al. (1993) showed a trend for more dissatisfied patients. Nevertheless, the majority of patients are still in favour of repeat selective denervation if they had the chance to initially choose again for a surgical treatment (Schweizer et al., 2006). The RTW rate was relatively high, despite the fact that a number (four and six, respectively) of patients in two studies had received financial compensation or were amidst a discharge procedure due to their incapacity to work (Sgromolo et al., 2018; Weinstein and Berger, 2002). Weinstein and Berger (2002) stated that a failure of the denervation was independently associated with workers’ compensation claims.
The reported complication rates after denervation suggest that further improvement of the current procedures and standardization of complication reports for selective denervation is needed, because it is still unclear which denervation technique is superior regarding complications. The effectiveness of the complete, PIN only, AIN and PIN and other partial denervation techniques varied in the studies published over the years and can in part be explained by the anatomical variation that complicates the identification of relevant nerve branches (Berger, 1998; Braga-Silva et al., 2011; Buck-Gramcko, 1977; Buck-Gramcko, 1993; Delclaux et al., 2017; Dellon, 1985; Ekerot et al., 1983; Ferreres et al., 1995; Fukumoto et al., 1993; Geldmacher et al., 1972; Grechenig et al., 1998; Hofmeister et al., 2006; Ishida et al., 1993; Patil and Arenas-Prat, 2016; Riches et al., 2016; Röstlund et al., 1980; Schweizer et al., 2006; Storey et al., 2011; Weinstein and Berger, 2002; Wilhelm, 2001).
Improving nerve identification may ensure more selective denervation techniques with similar results to complete denervation (Ekerot et al., 1983) to treat chronic pain while preserving the range of motion (Sgromolo et al., 2018) and leaves the option open for other salvage procedures in case of insufficient pain relief. Despite heterogeneity in the literature and therefore without conclusive evidence of which technique is superior, denervation of the wrist shows a trend towards positive patient outcomes in regard to pain relief, RTW rate and patient satisfaction. Standardization of measuring and reporting outcomes (e.g. using standardized scoring systems for pain and grip strength) should be introduced in order to conclude which surgical technique is best for treating chronic pain. Further exploration of methods to overcome disappointing results due to anatomical variation and misidentification of the relevant sensory nerves could lead to more effective denervation procedures.
Supplemental Material
JHS886777 Supplemetal Material1 - Supplemental material for Selective denervation of the wrist for chronic pain: a systematic literature review
Supplemental material, JHS886777 Supplemetal Material1 for Selective denervation of the wrist for chronic pain: a systematic literature review by Kenneth W. T. K. Chin, Anton F. Engelsman, Thomas M. van Gulik and Simon D. Strackee in Journal of Hand Surgery (European Volume)
Supplemental Material
JHS886777 Supplemetal Material2 - Supplemental material for Selective denervation of the wrist for chronic pain: a systematic literature review
Supplemental material, JHS886777 Supplemetal Material2 for Selective denervation of the wrist for chronic pain: a systematic literature review by Kenneth W. T. K. Chin, Anton F. Engelsman, Thomas M. van Gulik and Simon D. Strackee in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.