
Abstract
The purpose of this study was to investigate prognostic factors for the time off work, the time to resumption of activities of daily living and hobbies, and duration of complaints in patients with a traumatic hand or wrist injury. In a 10-month longitudinal prospective cohort study, 383 patients were included and interviewed in person every 2 to 3 months. Several sociodemographic, psychological and work-related prognostic factors were investigated. For the time off work, job type, diagnosis, complication, blaming someone else for the trauma and gender were all found to be individual prognostic factors in Cox regression. For the time to resumption of activities of daily living and hobbies, and duration of complaints, gender, diagnosis, treatment and complications were found to be prognostic factors in univariate analysis. Age was solely correlated with resumption of activities of daily living and the duration of complaints. Considering these prognostic factors can help predict a patient’s recovery more accurately.
Introduction
Traumatic hand and wrist injuries are known to be associated with high costs and a high impact on many areas of patients’ lives. Previous literature has predominantly focused on the time patients need to return to work. Multiple prognostic factors have been identified, including gender, age, income, educational level, dominant hand, employment type, type of work, location of the injury, responsibility for the injury, symptoms of PTSS (post-traumatic stress syndrome), diagnosis and hand injury severity score. For many of these factors, different studies have found opposing outcomes, as outlined in the systematic review by Shi et al. (2014). Furthermore, the vast majority of previous studies have either a low level of evidence (retrospective cohort studies) or a small sample size. The high quality prospective study by Opsteegh et al. (2009) focuses solely on return to work in operatively treated patients, including elective procedures for non-traumatic hand disorders. Outcomes other than return to work, such as the time patients’ need to resume their activities of daily living (ADL) or hobbies, have been studied to a minimal extent.
The purpose of the current study was to measure the impact of traumatic hand and wrist injury more broadly, by investigating prognostic factors for the time off work, time to return to ADL, resumption of hobbies and duration of complaints. Furthermore, the purpose was to integrate the majority of previously studied prognostic factors in one study.
Methods
A prospective cohort study was carried out, including all adult patients (18 years or above) with a new traumatic hand or wrist injury who presented at the Emergency Department in a 4-month period between 1 December 2016 and 31 March 2017 at Isala Zwolle, the Netherlands.
These injuries were defined as an injury caused by any form of trauma, with the location of injury including the fingers, hand or wrist (whereby the proximal border of the wrist was set at the distal one-third of the forearm).
Patients
Patients in whom the traumatic hand or wrist injury was not the only injury, patients with other severe illnesses and those who did not speak English or Dutch were excluded. Data was collected through structured personal interviews. Patients were first interviewed within 2 weeks after the trauma to obtain (and verify) their baseline measurements. Subsequently, they were interviewed every 1 to 2 months until patients had resumed all their activities and were free of complaints or until follow-up ended (5 to 9 months). The interviewer was blinded for all baseline measurements during all but the first interview.
Demographic variables included age at the date of the trauma and gender. Clinical factors included the side of the injured hand, whether this was the patient’s dominant hand and a detailed description of injury (later classified into diagnostic groups). Trauma-related factors included the circumstances of occurrence of the trauma (whether the patient holds someone else responsible for the trauma), and whether the trauma occurred during work or private time. Work-related factors included whether the patient had a job, the number of working hours per week, the type of employment (employed or self-employed) and the type of work. A description of the job, including physical demands, was obtained and later classified into blue collar or white collar. White-collar jobs were defined as jobs that have low physical demands, such as administrative work, service jobs or light retail work. Blue-collar jobs were defined as jobs that have high physical demands, such as construction and production work or heavy retail work.
Assessments
Primary outcome measurements were the time to resume work fully (the same number of working hours as before the trauma) and the duration of complaints in weeks. Having complaints was defined as ‘having pain or physical limitations to such an extent that they affected several daily activities’. Secondary outcome measurements were the time to resume work partially (fewer working hours than before the trauma), the time to resume ADL and the time to resume hobbies. All times were measured in weeks. For patients who did not resume certain activities or still had complaints at the end of follow-up, the period between their trauma and the last measuring point (their last direct interview) was noted. The outcomes ‘complication’ and ‘operatively treated’ were recorded. A complication was defined using the definition of the Dutch federation of medical specialists (Federatie Medisch Specialisten, 2017): ‘An unintended or unwanted outcome of treatment, resulting from the (lack of) actions from the caregiver, which is detrimental to the patients’ health to such extend that a change in treatment is necessary and/or that there is (irreparable) physical damage’. Changes in job due to the trauma were documented.
Statistical analysis
Normality of the variables was assessed both by Shapiro–Wilk and Kolmogorov–Smirnov test. Mann–Whitney U tests (two unpaired groups) or Kruskal Wallis tests (multiple unpaired groups) were used to test for differences between groups.
Correlations between continuous variables were assessed using Spearman’s Rho and Kendall’s tau. Before Cox regression, variables were tested for multicollinearity using Pearson Chi-Square and Fisher’s exact test for dichotomous variables and Spearman’s Rho and Kendall’s tau for continuous variables. Proportional hazards were assumed after assessing the log-minus-log plots of all variables in the model. In Cox regression, all variables were fixed covariates.
Results
Four hundred and eight patients were eligible for inclusion in the study. In 25 patients, consent was not obtained and another 29 patients were lost to follow-up. In 354 patients, follow-up (87% of all eligible patients) was complete.
Baseline characteristics
Baseline characteristics of the patients.
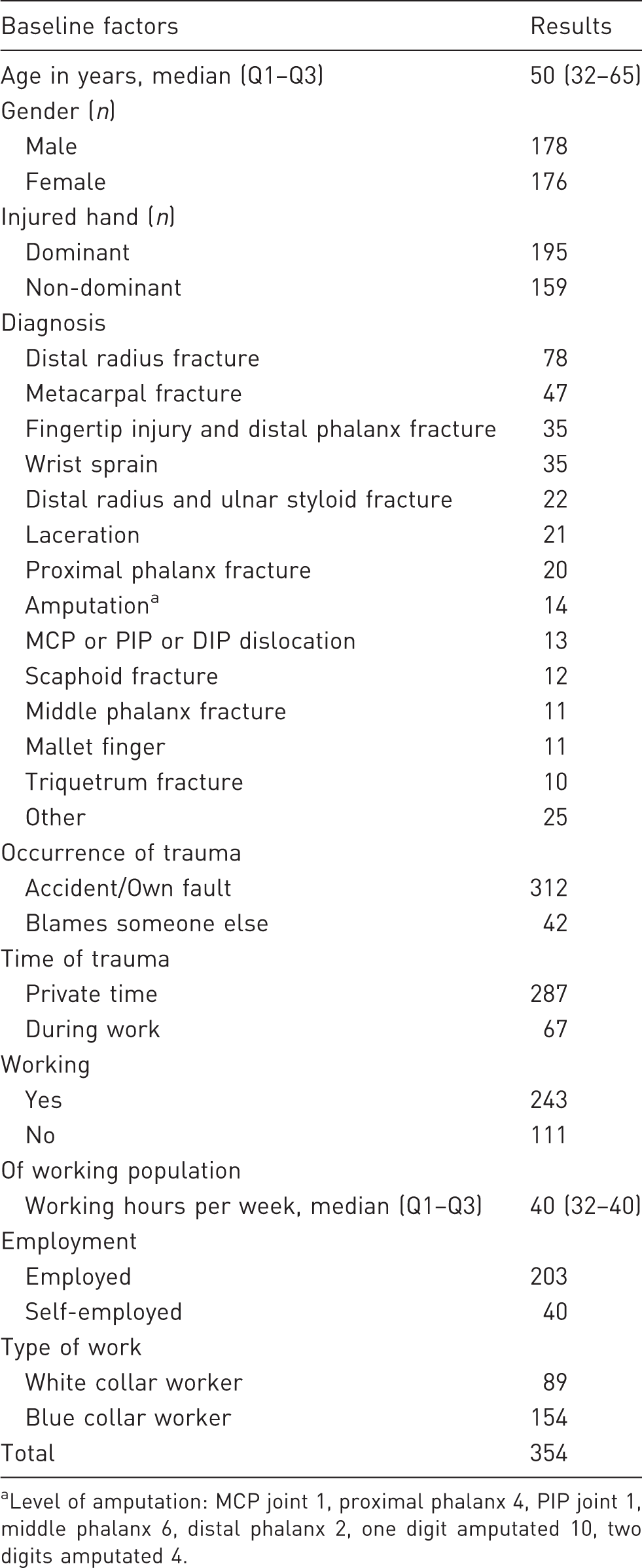
Level of amputation: MCP joint 1, proximal phalanx 4, PIP joint 1, middle phalanx 6, distal phalanx 2, one digit amputated 10, two digits amputated 4.
Return to work
Of the 243 working patients, two did not return to work for reasons other than their hand or wrist injury. The remaining 241 patients resumed their work partially in a median time of 1 week and fully in 2 weeks. Due to the trauma, four patients did not return to work fully, 13 did not return to work at all and 17 had to change their job.
Variables and median (first and third quartiles, Q1–Q3) time to event in weeks.
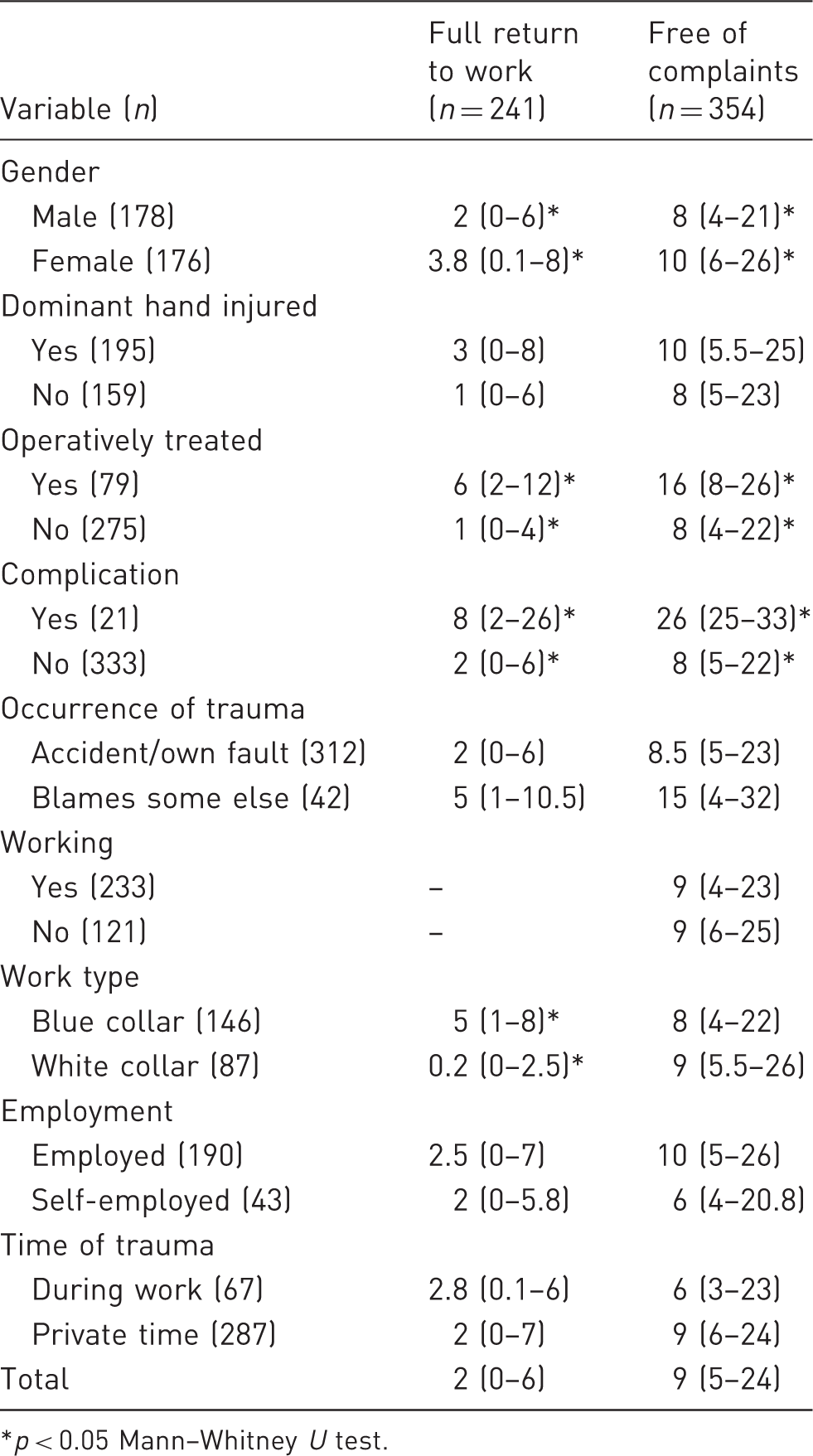
p < 0.05 Mann–Whitney U test.
ADL and hobby resumption
Four patients did not do any ADL tasks themselves before the trauma and the remaining 350 patients resumed their ADL in a median time of 4.5 weeks. Twenty-nine of 350 patients did not resume full ADL activities. Of the 343 patients who had a hobby at the time of the trauma, 40 did not resume their hobby. The median time to resume hobbies was 5 weeks. Higher age had a significant positive correlation with the time to ADL resumption, but not with hobby resumption. Female patients, patients with a complication and operatively treated patients took significantly longer to resume both their ADL and hobby.
Employed patients and patients whose trauma occurred during work both resumed their ADL significantly faster. When excluding patients without a job from the analysis, this significant difference remains intact. Furthermore, self-employed patients resumed their hobby significantly faster compared with employed patients. The number of working hours per week was not correlated with either ADL or hobby resumption.
Duration of complaints
The median time until patients were free of complaints was 9 weeks. At the end of follow up, 108 of 354 patients still experienced complaints. Female patients, patients of higher age, operatively treated patients and patients with a complication had complaints significantly longer (Table 2).
Diagnosis
Patients with an amputation or distal radius and ulnar styloid fracture had the longest time off work, both with a median time of 7 weeks until full return to work. Those with a scaphoid or distal radius fracture both took 5 weeks to fully return to work. The fastest work resumption was seen in patients with a mallet finger or metacarpo-phalangeal, proximal interphalangeal or distal interphalangeal dislocation. They returned to work fully in a median time of zero weeks, although they were not free of complaints for median times of 10 and 6 weeks, respectively.
The time needed to resume all ADL activities was the longest for patients with a scaphoid fracture (8 weeks) or proximal phalanx fracture (6.5 weeks). The time to resume hobbies was the longest for patients with an amputation (13 weeks), scaphoid fracture (11.5 weeks) or proximal phalanx fracture (8.5 weeks).
The diagnoses with the longest duration of complaints were amputation (28 weeks), scaphoid fracture (25.5 weeks) and proximal phalanx fracture (24 weeks). Patients with wrist sprain or laceration had the shortest durations of complaints (3 and 4 weeks, respectively). For all outcome measures there were significant differences between diagnoses.
Predictive model for return to work
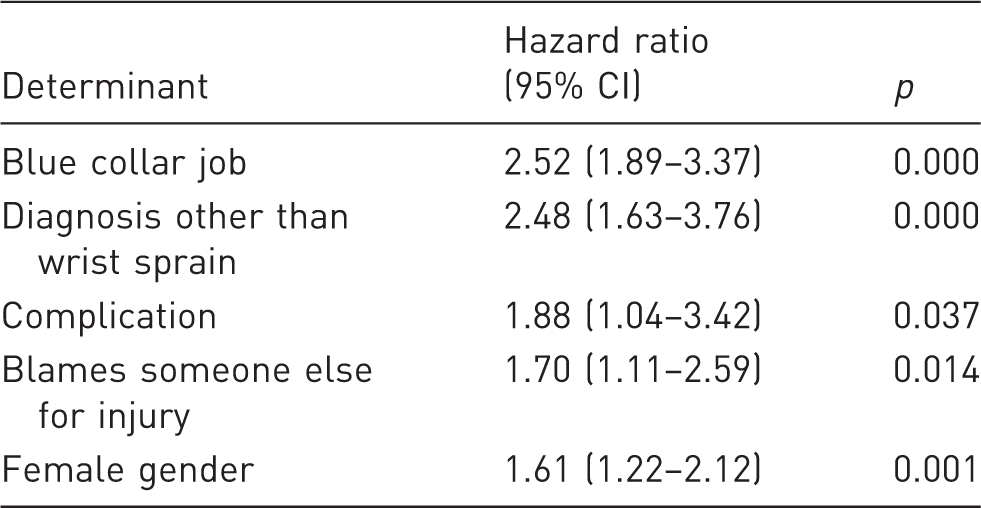
Return to work, Cox regression.
Discussion
For return to work, the type of work was found to be the strongest predictor. This finding is in accordance with all previous literature assessing type of work (Bruyns et al., 2003; Gustafsson and Ahlstrom, 2004; Opsteegh et al., 2009; Skov et al., 1999). The second and third strongest predictors were a diagnosis other than wrist sprain and a complication. The fourth strongest predictor is the circumstances of occurrence of the trauma; patients who hold someone else responsible for their injury take longer to return to work. This finding is consistent with previous research (Grunert and Dzwierzynski, 1997; Rusch et al., 2003).
The last independent predictor with the lowest hazard ratio is gender; females taking longer to return to work. This outcome is contradictory to what was reported by Chang et al. (2011), Lee et al. (2010) and Skov et al. (1999), who found gender not to be a prognostic factor. However, these were all retrospective cohort studies relying on medical records as their data source. Alongside return to work, gender was also a prognostic factor for ADL resumption, hobby resumption and the duration of complaints. Contrary to Skov et al. (1999), we did not find employment type to be a predictor for return to work. This could be due to a relatively low number of self-employed patients in the study (n = 40 or 16%).
Other prognostic factors for resumption of ADL and hobbies and the duration of complaints were operative treatment, complications and diagnosis (most notably, patients with wrist sprain take less time). Age is positively correlated with the time to ADL resumption and the duration of complaints. Furthermore, working patients resume their ADL significantly faster as compared with unemployed patients, although age is likely to be a confounding variable here. Next to that, patients whose trauma occurred during working time resume their ADL faster than patients whose trauma occurred during private time. This significant difference remains intact after excluding unemployed patients, making age less likely to be a confounder here. Outcome measures other than return to work have not been researched in previous literature.
At the end of follow up 93% of patients had fully returned to work, 92% resumed their ADL, 86% resumed their hobby and 70% were free of complaints. Patients, who at the end follow-up had not resumed certain activities, were accounted in the analysis with the time to the last interview. This makes all the presented median times to events underestimations of the reality.
Strengths of the current study are the high rate of complete follow-up (87% of all eligible patients) and the relatively large sample size. Potential prognostic factors were selected on the basis of previous literature provided they could be recorded through personal interviews. This method of data collection could induce some information bias. Although return to work is a clear event, the other outcome measures (ADL resumption, hobby resumption and duration of complaints) are more subjective.
Footnotes
Acknowledgements
The authors thank Lonneke Buijteweg (Emergency physician at Isala Zwolle, the Netherlands) and all other staff involved at the Emergency Department at Isala Zwolle for all their efforts concerning setting up the study and including patients. The authors also thank Sander Brink (Epidemiologist and statistician at Isala Zwolle, the Netherlands) for his help with the statistical analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval details
This study was approved by the medical ethics committee at Isala Zwolle, the Netherlands.
Informed consent
Verbal informed consent was obtained for all patients included in the study.