
Abstract
This study investigates the pattern of hand injuries presenting to a UK regional tertiary centre. All referrals to our Hand Surgery Unit in 2019 were reviewed. Subgroup analyses of sex, deprivation, occupational injuries and assault cases were carried out. Over the study period, 4216 cases were referred. Most were male (70%), with a median age of 36 years and from a deprived area (75.2%). Soft tissue injury was documented in 53.6% and bone injury (fracture/dislocation) in 52.4%. Surgical management was required in 2214 (52.5%) cases. Work-related injuries accounted for 16.7% of cases and were more likely to require surgery. Assault-related injuries accounted for 8% of cases, with a male preponderance. Our findings can help facilitate service provision and guide regional and national prevention policies.
Introduction
Hand injuries are caused by a variety of mechanisms, in a variety of environments. Details about the epidemiology of acute hand injuries in the UK secondary care setting are relatively scarce. According to NHS Digital (2020), there were 25 million emergency department attendances in the year 2019/2020, representing a 17% increase from 2010/2011. However, there were no data about the types of injuries.
The complexity of the hand and its functional importance means there are significant costs associated with hand trauma, both direct and indirect, with many patients requiring specialist referral for appropriate management; these cases represent a considerable physical, psychosocial and socioeconomic burden. They are associated with loss of productivity, anxiety, depression and post-traumatic stress disorder (Gustafsson and Ahlström, 2004; Maddison et al., 2023; Trybus et al., 2006). In the USA, hand injuries rank first in the order of the most expensive types of injury, above knee injuries, lower limb fractures, pelvic fractures and brain injuries (de Putter et al., 2012).
Knowledge of the epidemiology of acute hand injuries is important to facilitate local, regional and national service provision, guide prevention strategies and legislation, provide a baseline to study current and future trends, and to power future clinical trials. The aim of this study was to investigate the pattern, incidence and management of hand injuries presenting to a large regional tertiary centre in the UK.
Methods
This project was prospectively registered with the clinical audit department at our hospital trust. A medical chart review was undertaken of all trauma referrals to the Hand Surgery department between 1 January 2019 and 31 December 2019 (inclusive). Non-traumatic presentations of hand pathology and bone injuries proximal to the wrist (such as distal radial fractures) were excluded from the study; however, all upper limb soft tissue injuries were included. Patients with closed ligamentous injuries of the elbow and wrists were excluded. There is a separate referral pathway in our hospital for these injuries and hence they were not captured in our database. Brachial plexus injuries were also excluded as these cases are treated by the peripheral nerve surgery team. Data were collected about demographics, type of injury and management. Although the patients were identified retrospectively, data were collected for patients at the time of attendance using a dedicated hand surgery database.
Statistical analysis
A descriptive statistical analysis of all the patients was carried out using SPSS software version 28 (IBM Corp., Armonk, NY, USA). Subgroup analyses of sex, occupational injuries and assault cases were then performed. Using patient postcodes, deprivation data were retrieved from the 2019 English indices of deprivation postcode finder published by the Ministry of Housing, Communities and Local Government (now known as the Department for Levelling Up, Housing and Communities) (Ministry of Housing, Communities and Local Government, 2019). The cohort was then divided into deprived and non-deprived groups and further subgroup analyses were undertaken. Categorical variables were compared using the chi-square test. The Kolmogorov–Smirnov test showed that age was not normally distributed within the cohort so Mood’s median test was used to compare the median age for each subgroup analysis. A p-value <0.05 was considered to be statistically significant.
Results
Over the 12-month study period, 5262 cases were assessed, of which 4216 met the inclusion criteria. The characteristics and outcomes of the whole population and sex subgroup analyses are reported in Table 1. The cohort was predominantly male (70%), with a median age of 36 years. Surgical management was required in 2214 (52.5%) cases. The rate of surgical management for open injuries was significantly greater than that for closed injuries (75.5% vs. 24.5%, respectively; p = 0.001).
Characteristics and outcomes of all hand injuries.
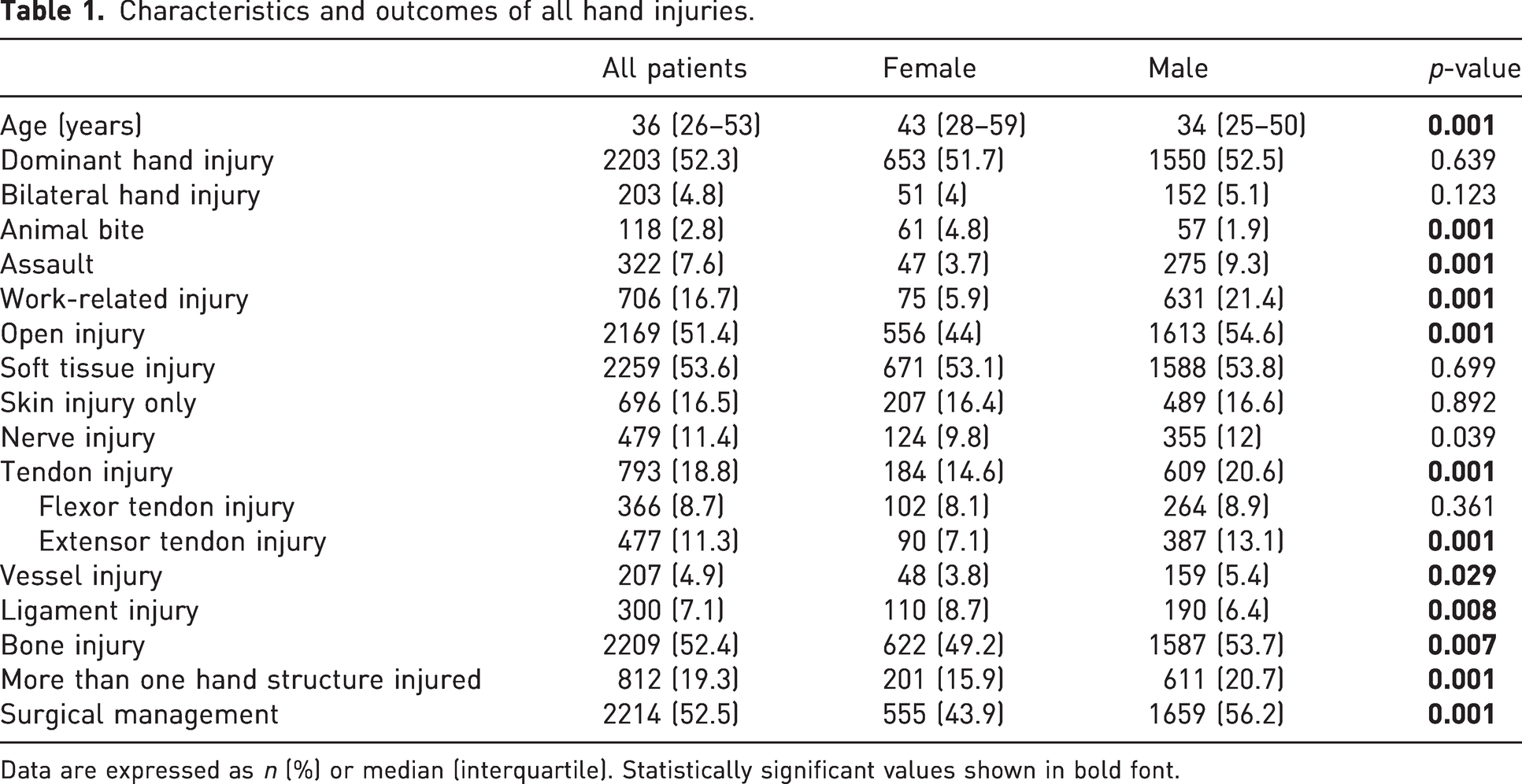
Data are expressed as n (%) or median (interquartile). Statistically significant values shown in bold font.
Table 2 presents a summary of the mechanisms of patient injuries. The most common mechanism of injury was a fall. Most work-related injuries occurred in men (89.4%). Bilateral and dominant hand injuries were less common among occupational injuries (p = 0.001). Soft tissue injury (including nerves, tendons and bloods vessels) was more prevalent in patients who sustained the trauma at work, relative to the rest of the cohort (71.1% vs. 50.1%, respectively; p = 0.001). This was also the case for surgical management (66.1% vs. 49.8%, respectively; p = 0.001) and penetrating injuries (p = 0.001). No significant difference was found with regard to hand fractures, dislocations or both. The other parameters of interest are highlighted in Table 3.
Mechanism of injury.
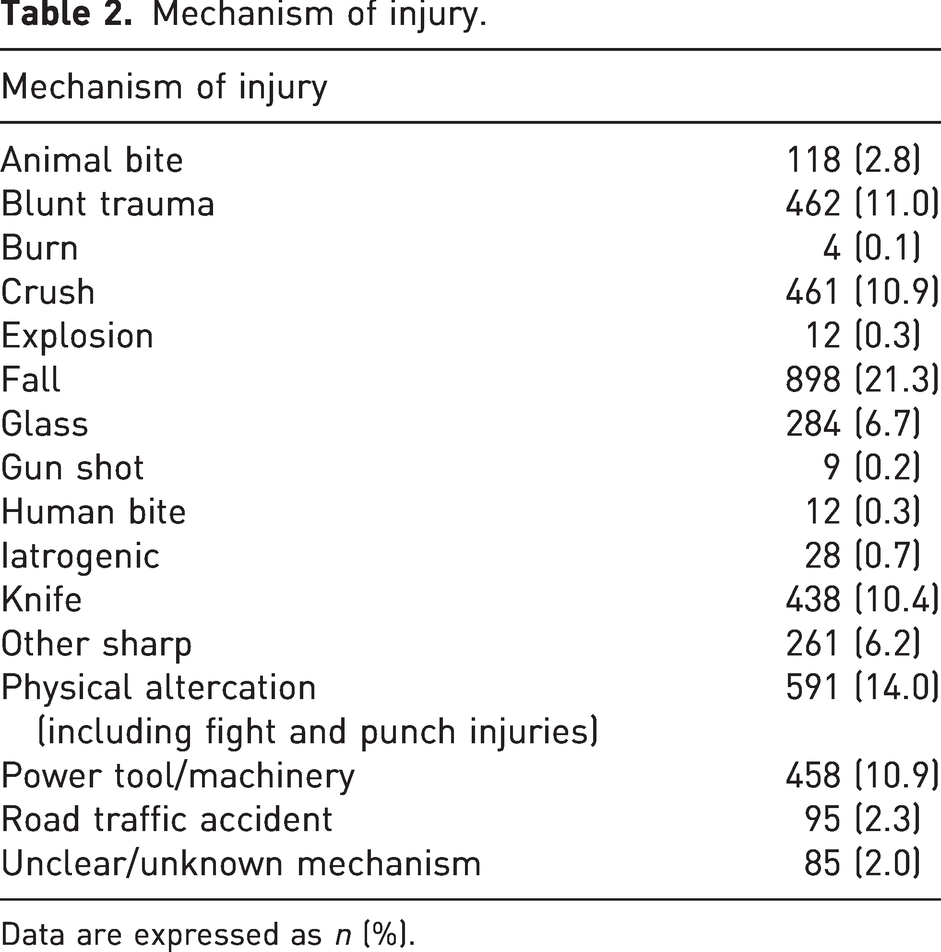
Data are expressed as n (%).
Characteristics and outcomes of occupational and non-occupational injuries.
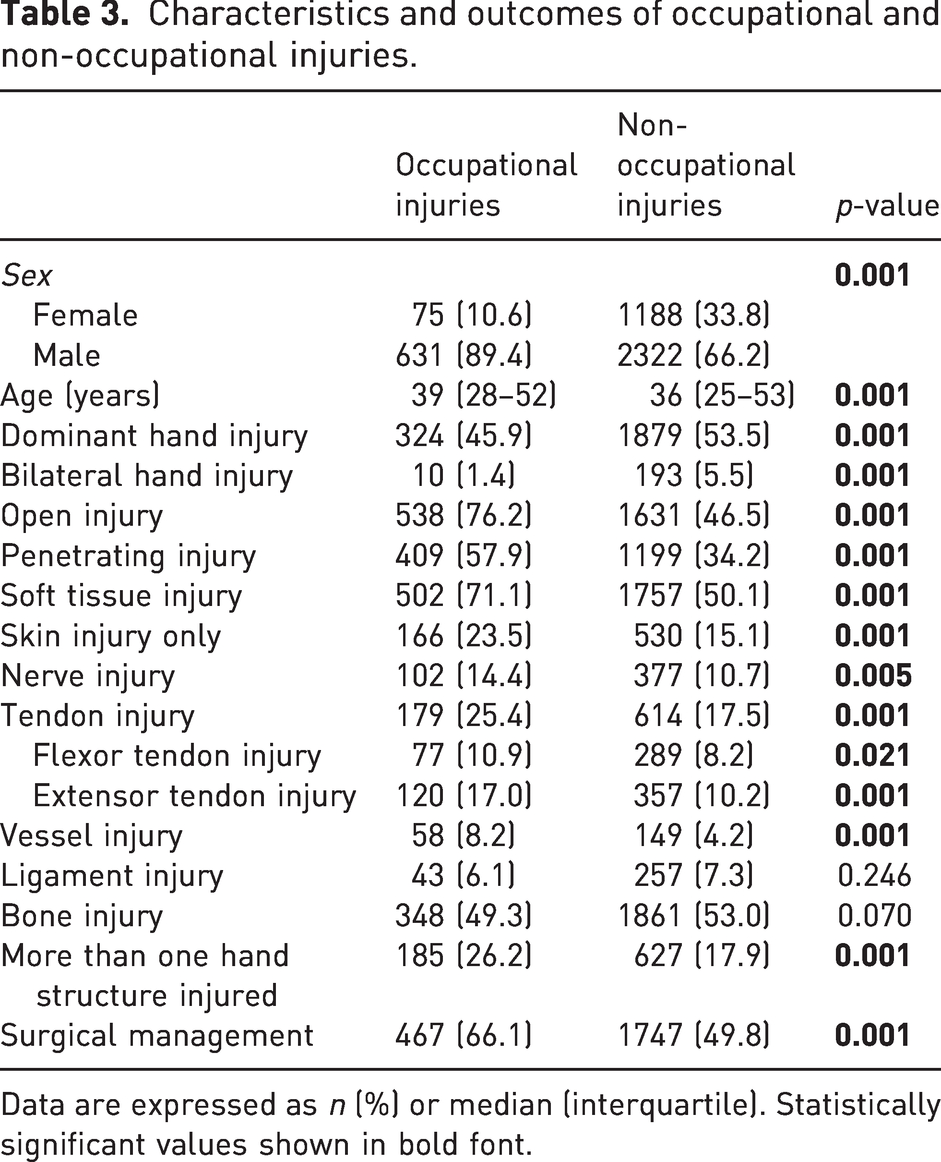
Data are expressed as n (%) or median (interquartile). Statistically significant values shown in bold font.
Within the whole group, 322 (8%) cases were assault-related injuries, with a male preponderance when compared to all non-assault injuries. The subgroup analyses for assault versus non-assault cases are presented in Table 4. Assault-related injuries were more likely to be bilateral, to damage more than one anatomical structure and to require surgery. Bone was the most frequently damaged structure, followed by tendons, nerves and finally blood vessels. The incidence of bone injury was similar to that in non-assault-related injuries, although the frequency of damage to all other structures described was significantly higher among assaulted patients.
Characteristics and outcomes of assault and non-assault-related injuries.
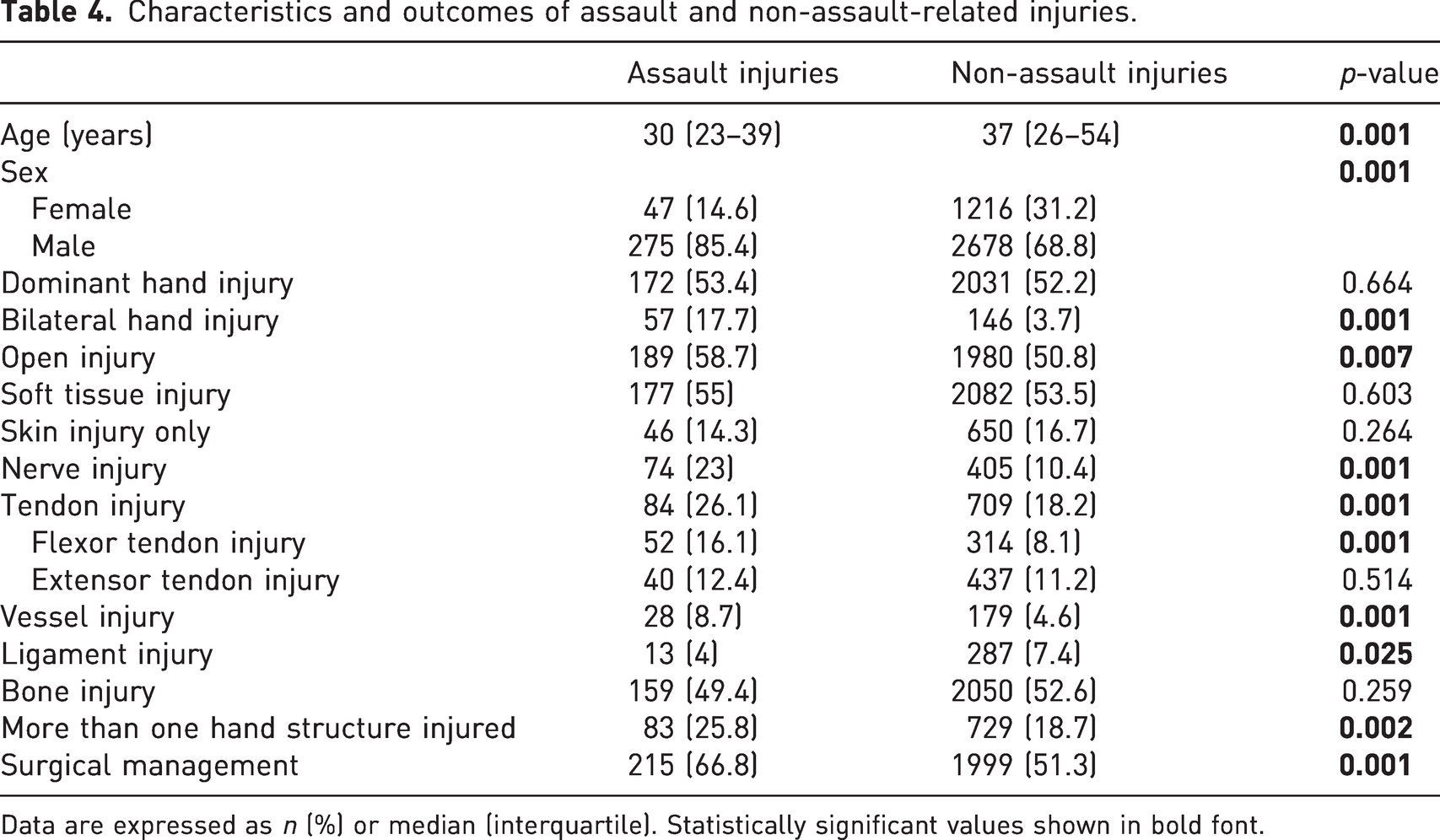
Data are expressed as n (%) or median (interquartile). Statistically significant values shown in bold font.
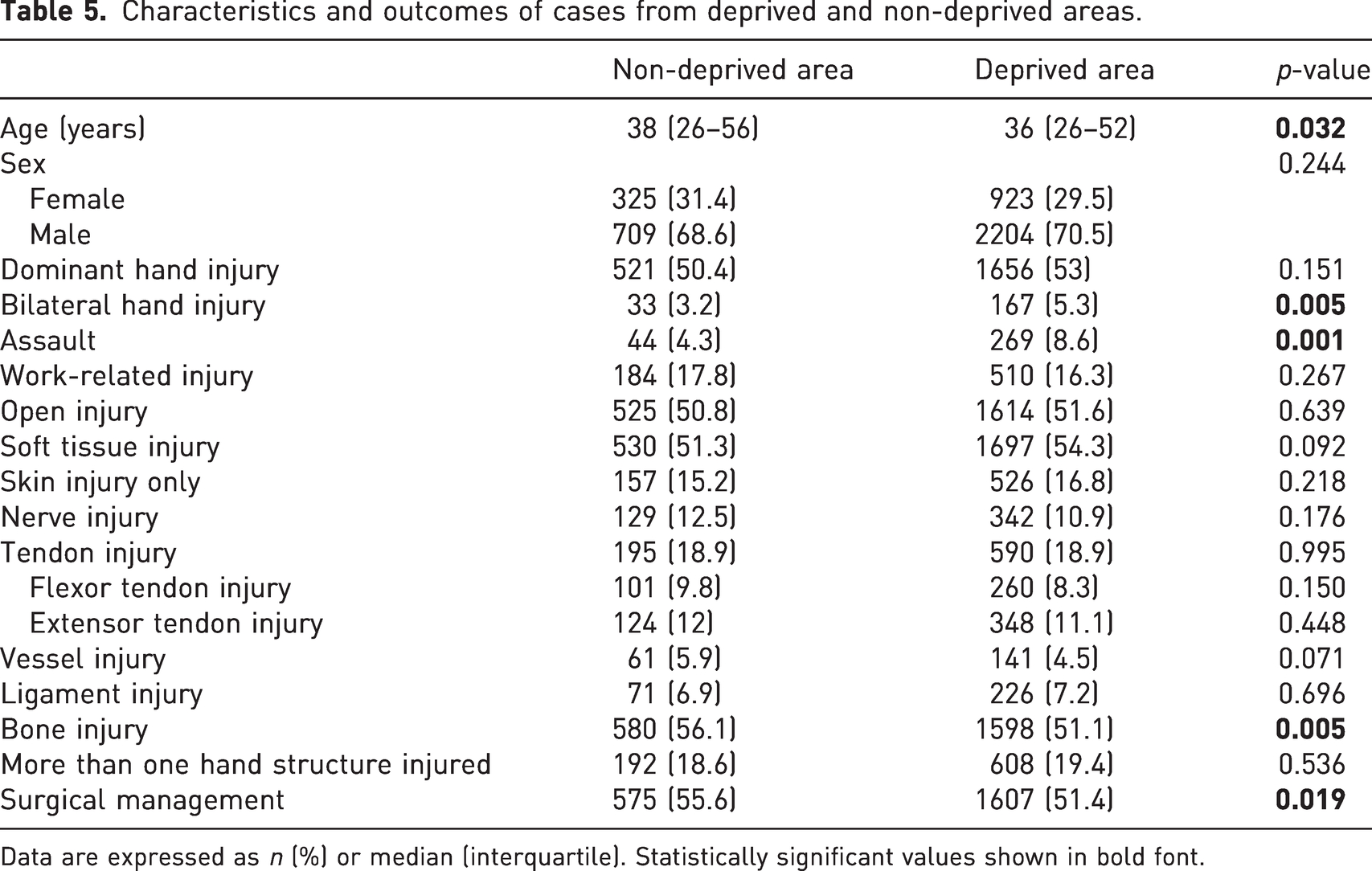
The subgroup analyses on deprivation are summarized in Table 5. Deprivation data, based on postcodes, were obtained for 4161 cases. Of these, 3127 (75.2%) were from a deprived area, with these cases more likely to be due to assault compared to their counterparts from non-deprived regions. Relative to the non-deprived group, cases from a deprived region were younger, and had a significantly greater rate of bilateral hand injuries, but lower incidence of bone injury and surgical management.
Characteristics and outcomes of cases from deprived and non-deprived areas.
Data are expressed as n (%) or median (interquartile). Statistically significant values shown in bold font.
Discussion
This study highlights the significant burden that hand trauma places on tertiary referral units, with 4216 cases presenting over a 12-month period, and more than half requiring surgery. There was a clear male preponderance and three-quarters of cases lived in deprived areas. This pattern was particularly pronounced in two common categories of injury mechanism: occupational and assault cases. Among those with work-related injuries, non-dominant hand injuries were more common.
Previous work has identified the hand and wrist as the most commonly injured anatomical regions in patients presenting for acute assessment (Ootes et al., 2012; de Putter et al., 2012), with up to one-quarter of total emergency department cases accounted for by hand trauma (Angermann and Lohmann, 1993; Arroyo-Berezowsky and Quinzaños-Fresnedo, 2021; Clark et al., 1985; Hill et al., 1998; de Putter et al., 2012; Rosberg and Dahlin, 2004). Furthermore, these cases have a substantial economic impact, with hand and wrist injuries recorded as the most expensive type of injury (de Putter et al., 2016), and US-based figures suggesting an annual cost of up to US$740 million (£580 million, €674 million) (de Putter et al., 2012, 2016). Fractures of the hand and fingers have previously represented the most common hand injury, as well as incurring the greatest cost to manage successfully (de Putter et al., 2012). This financial effect is thought to be a result of lost productivity in those affected (de Putter et al., 2012). Occupational hand injuries are said to incur both high healthcare and wider societal costs than other types of injury (Rosberg et al., 2013), which may be linked to a delayed return to work after the event (Opsteegh et al., 2009).
Occupational hand injuries were common in our series, similar to previous reports (Burke et al., 1991; Dębski and Noszczyk, 2021). Removal of locks and safety guards from power tools is thought to increase productivity, with obvious implications for worker safety (Dębski and Noszczyk, 2021; Smith et al., 2018). We cannot detail any lack of specific safety measures for the work-related injuries in our series. However, the high incidence of unilateral, non-dominant hand injuries may be a result of loss of control of a power tool held in the dominant hand. Penetrating injuries from power tools may also explain the pattern of soft tissue damage recorded. Prevention of work-related hand trauma may be helped by appropriate education, quality control of mechanical tools and enforcement of effective safety protocols (Buffet et al., 2022; Smith et al., 2018). The indirect societal costs may also be minimized by urgent referral to specialist hand surgery centres to optimize treatment and expedite recovery (Misra et al., 2017; Patterson et al., 2010; Trybus et al., 2006). Well-equipped hand trauma services are essential to improve overall outcomes and our findings may be used by departments serving a similar population to guide the planning and execution of service delivery.
Despite the wealth of data on work-related injuries, relatively little has been published about assault-related hand trauma. A descriptive analysis from India reported that assault-related hand trauma accounts for 13.5% of cases (Desai et al., 2018), while a recently published Australian study attributed 4% of cases to ‘violent injury’ (Saleh et al., 2023). Although direct comparisons may be limited by the different populations served, we found that 7.6% of hand trauma presentations were due to assault. There were also significantly more bilateral limb injuries and damage to soft tissue structures, with multiple structures affected. Knives are the weapon of choice in assaults in the UK (Hobson et al., 2022; Palasinski et al., 2021), and there has been an increase in the incidence of knife-based crime (Ajayi et al., 2021). Knife injuries accounted for 41% of the assault cases in our cohort. Furthermore, victims of knife crime are more likely to have a lower socioeconomic status (Reilly et al., 2022). The area served by our hand trauma unit is ranked as the seventh most deprived local authority in England (Ministry of Housing, Communities & Local Government, 2019), with most of our patients coming from deprived areas. Assault-related hand trauma in the West Midlands area of the UK may benefit from well-implemented preventative measures to tackle knife crime, using multimodal strategies that have been shown to produce significant reductions in weapon offences and injuries in urban areas (Murray et al., 2015).
The proportion of men in this study (70%) was consistent with other previous epidemiological studies from trauma centres in the UK (Hill et al., 1998), Europe (Moellhoff et al., 2023) and in the USA (Butala et al., 2014; Wenzinger et al., 2019). However, the proportion of men with work- and assault-related hand injuries was increased, being 89.4% and 85.4%, respectively, in these subgroups. A male preponderance of work-related injuries has previously been identified (Dębski and Noszczyk, 2021).
To our knowledge, this study is one of the largest published analyses of hand trauma presentations. It updates other UK-based studies (Angermann and Lohmann, 1993; Clark et al., 1985; Hill et al., 1998), and the number of patients is twice that of other more recent epidemiological studies (Arroyo-Berezowsky and Quinzaños-Fresnedo, 2021). Although we present data from 2019, a previously published study found that presentations to our unit fell by half during the COVID-19 pandemic (Pidgeon et al., 2021). Our findings provide a perspective on hand trauma that is not influenced by peri-pandemic changes (Saleh et al., 2023), allowing the data to guide service provision when there is an expected return to previous trends. Our series was from adults seen at a large hospital serving a predominantly urban area. The results may not be generalizable to departments treating children, in whom the injury patterns may differ (Dizin et al., 2022). This study is also limited by incomplete data in certain cases. Although data were prospectively recorded on an electronic system, some records lacked details as a result of inadequate documentation by the assessing clinician.
Hand trauma presents a considerable healthcare burden, one that has economic consequences for the patient and the wider society. This study can help facilitate service provision, guide regional or national intervention prevention policies, and provides baseline data on current hand trauma trends to inform future prospective studies.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received the following financial support for the research, authorship, and/or publication of this article: HKNK and ST are National Institute for Health Research (NIHR) Academic Clinical Fellows. No direct funding was received for this article. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.