
Abstract
Background:
Individuals receiving invasive mechanical ventilation experience mobility limitations and are at risk for intensive care unit-acquired weakness and functional decline. Hydrotherapy has been proposed as a potential adjunct within complex care and rehabilitation pathways, as the physical properties of water may facilitate supported movement and upright activity. However, its use in ventilator-dependent populations is often avoided due to safety and feasibility concerns. This systematic review aimed to synthesize the available evidence on the safety, feasibility, and clinical implementation of hydrotherapy in this population.
Methods:
A systematic review was conducted in accordance with PRISMA 2020 guidelines and prospectively registered in PROSPERO. Six electronic databases were searched. Eligible studies included individuals receiving invasive mechanical ventilation who participated in clinically supervised hydrotherapy. Given heterogeneity in study designs and outcomes, a structured narrative synthesis was undertaken with emphasis on safety, feasibility, and ventilator management.
Results:
Six studies were included. Across all studies, hydrotherapy was consistently reported as safe, with no airway- or ventilation-related adverse events, including accidental extubation, tracheostomy displacement, ventilator disconnection, or water ingress. Feasibility was demonstrated in intensive care, rehabilitation, long-term ventilation, and pediatric prolonged mechanical ventilation settings when structured protocols, multidisciplinary staffing, and continuous physiological monitoring were employed. Reported outcomes included stable respiratory parameters, facilitated movement, and positive experiential responses.
Conclusions:
Although the evidence base is limited and predominantly descriptive, available findings suggest that hydrotherapy can be safely and feasibly delivered to selected individuals receiving invasive mechanical ventilation in well-resourced clinical environments.
Keywords
Introduction
Individuals receiving invasive mechanical ventilation in the context of critical illness frequently experience marked limitations in mobility and upright activity, with immobility or bed-based activity predominating during ICU stay. 1 In this population, ICU-acquired weakness is common and strongly associated with prolonged ventilation, increased mortality, and long-term functional impairment. 2 Therapeutic aquatic environments have been described as offering distinct mechanical properties such as buoyancy, hydrostatic pressure, viscosity, and warm-water immersion that reduce gravitational load, support assisted movement, and may expand opportunities for health-related functioning compared with land-based settings.3–5 These properties may be relevant for individuals with mobility limitations, as water-based interventions have been shown to improve postural control and physical functioning. 6 Within the context of critical care, however, the relevance of aquatic therapy extends beyond rehabilitation considerations and raises fundamental questions related to safety, feasibility, and systems-level decision-making when applied to invasively ventilated patients.
Individuals who require invasive mechanical ventilation represent one of the most medically complex populations in critical care, with prolonged ventilation often accompanied by intensive care unit-acquired weakness, disuse atrophy, and reduced functional capacity, and downstream effects on daily functioning and participation.7,8 In pediatric populations, prolonged mechanical ventilation is similarly linked to post-intensive care sequelae affecting physical, cognitive, and emotional well-being, with potential long-term implications for development and quality of life. 9 Comparable long-term physical impairments have been demonstrated in adult survivors of acute lung injury requiring mechanical ventilation. 10 Early rehabilitation and mobilization strategies within critical care have been shown to improve selected clinical and functional outcomes in mechanically ventilated adults, including reduced duration of mechanical ventilation and ICU length of stay, and improved muscle strength and functional status.7,11
Aquatic therapy has been proposed as a potential adjunct to these approaches, as buoyancy and warm-water immersion may enable supported movement, upright tolerance, and graded activity in individuals who are unable to tolerate conventional land-based mobilization.3–5 In addition, studies have reported perceived psychosocial experiences such as increased motivation, enjoyment, and a sense of normalcy among both pediatric and adult populations; however, these findings remain exploratory and secondary to considerations of safety and feasibility in critically ill populations.12–16
Despite these potential benefits, hydrotherapy in invasively ventilated patients raises substantial safety and logistical concerns, particularly regarding airway protection, ventilator circuit integrity, and the organizational complexity of delivering aquatic interventions in critical care settings.12,13,15 In addition to clinical concerns, published feasibility reports and qualitative studies highlight the considerable logistical and organizational demands associated with implementing hydrotherapy for invasively ventilated patients, including access to specialized facilities, trained multidisciplinary teams, structured transfer procedures, and rigorous safety protocols.12–15 Such infrastructure is not routinely embedded within acute critical care pathways, and limited exposure to aquatic interventions in these contexts may further contribute to perceptions of elevated risk.
Consequently, aquatic therapy may be underutilized in clinical practice, even where aquatic services exist, limiting access to an intervention that may otherwise support movement and activity for individuals with severe mobility constraints.
The existing evidence base remains limited and heterogeneous, consisting predominantly of case reports, feasibility studies, and qualitative investigations conducted across intensive care units, pediatric programs, and long-term ventilation services.12–16 To date, no systematic synthesis has integrated the available evidence regarding safety, feasibility, health-related outcomes, and implementation considerations of hydrotherapy in this population. The aim of this systematic review was therefore to synthesize the available evidence on hydrotherapy for individuals receiving invasive mechanical ventilation, with a primary focus on safety, feasibility, and clinical implementation within critical care and related systems.
Methods
Design and registration
This systematic review was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; ID: CRD420251231930) and conducted in accordance with the PRISMA 2020 guidelines. 17 The registered protocol prespecified the research question, eligibility criteria according to the PICOS framework, information sources, screening and selection procedures, data extraction processes, quality appraisal methods, and a structured narrative synthesis approach with a specific focus on safety, feasibility, and clinical implementation.
Given the anticipated heterogeneity of study designs and outcome measures, meta-analysis was not planned a priori. No deviations from the registered protocol occurred.
Eligibility criteria
Population
Studies were eligible for inclusion if they involved children or adults receiving invasive mechanical ventilation via tracheostomy or endotracheal tube, across any clinical context in which mechanical ventilation was actively managed. Eligible settings included intensive care units, step-down units, post-acute care environments, and long-term ventilation services. Studies involving non-invasive ventilation only (e.g. CPAP or BiPAP without tracheostomy) were excluded. Although included studies spanned intensive care, post-acute, and long-term ventilation settings, invasive mechanical ventilation constituted the defining clinical condition anchoring this review, reflecting a continuum of critical care-related management rather than discrete patient populations.
Intervention
Eligible interventions comprised clinically supervised therapeutic aquatic interventions, including hydrotherapy, aquatic physiotherapy, hydrokinesiotherapy, and warm-water therapeutic exercise, delivered by trained clinicians with therapeutic intent. Interventions limited to hygiene-related purposes or conducted without qualified clinical supervision were excluded.
Outcomes
Studies were required to report at least one outcome relating to: (1) safety and adverse events; (2) physiological, functional, or health-related responses; (3) psychosocial or experiential outcomes; or (4) feasibility and implementation considerations.
Study design
In light of the limited and emerging evidence base, all empirical study designs were eligible for inclusion, including case reports, case series, qualitative and mixed-methods studies, and observational designs. Randomized or quasi-experimental studies were eligible but none were identified.
Information sources and search strategy
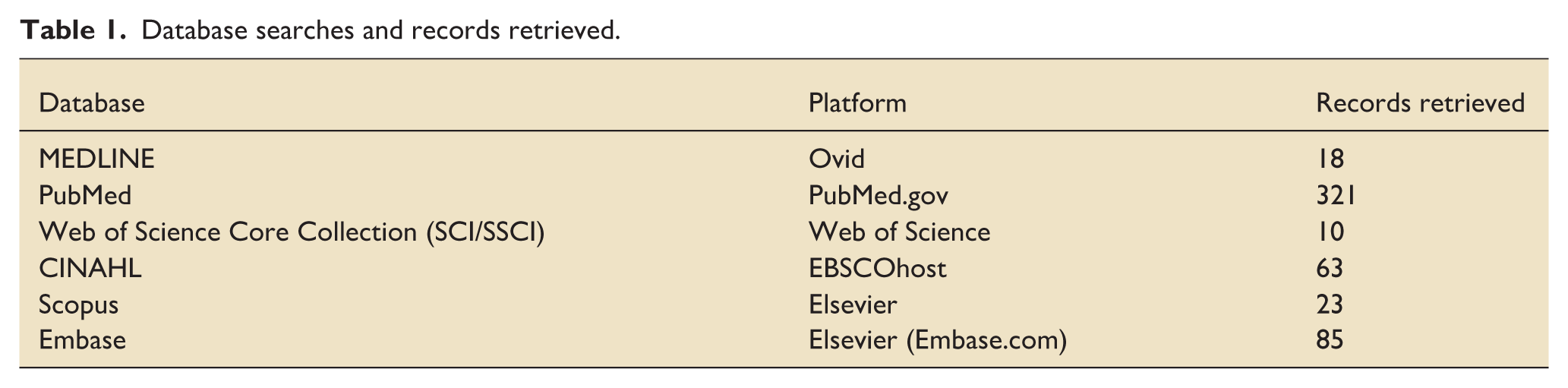
A comprehensive literature search was conducted between 22 November and 25 December 2025 across six electronic databases: MEDLINE (Ovid), PubMed, Embase, CINAHL (EBSCOhost), Scopus, and the Web of Science Core Collection (SCI/SSCI). One additional record was identified through citation tracking and manual searching. No restrictions were applied with respect to publication date, language, or country.
Details of database searches and records retrieved are presented in Table 1, and full electronic search strategies for all databases are provided in Supplemental Appendix A.
Database searches and records retrieved.
Study selection
Records were imported into Rayyan (QCRI), an online systematic review management tool, and duplicates were removed prior to screening. Two reviewers (MN and YM) independently screened titles and abstracts, followed by independent full-text review. Disagreements were resolved through discussion and consensus.
Thirteen full-text articles were assessed for eligibility, of which seven were excluded due to non-eligible populations, resulting in six studies included in the final synthesis. Where studies included mixed samples, only data relating to individuals receiving invasive mechanical ventilation during aquatic therapy were extracted.
Data extraction
Data extraction focused on study design, clinical context, participant characteristics, ventilation modality, aquatic intervention procedures, safety monitoring practices, and reported outcomes relating to safety, physiological or functional responses, psychosocial experiences, feasibility, and implementation.
No study authors were contacted for additional information.
Quality appraisal
Methodological quality was assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Tools, with the checklist appropriate to each study design applied. 18 One reviewer conducted the appraisal, and a second reviewer independently verified all assessments. Appraisal criteria and summary ratings are presented in Supplemental Appendix B.
Synthesis approach
Given the prespecified focus on safety, feasibility, and clinical implementation, and the substantial heterogeneity across study designs, populations, interventions, and outcome measures, quantitative synthesis was not appropriate.
A structured narrative synthesis was therefore undertaken, integrating findings across studies to identify recurring patterns related to safety signals, feasibility parameters, health-related clinical responses, and implementation considerations relevant to critical and post-critical care contexts.
Results
Study selection
Details of the search and screening process are presented in the PRISMA 2020 flow diagram (Figure 1). Following duplicate removal, 415 records were screened by title and abstract. Thirteen full-text articles were assessed for eligibility, of which seven were excluded due to non-eligible populations. Six studies met the inclusion criteria and were included in the final synthesis.
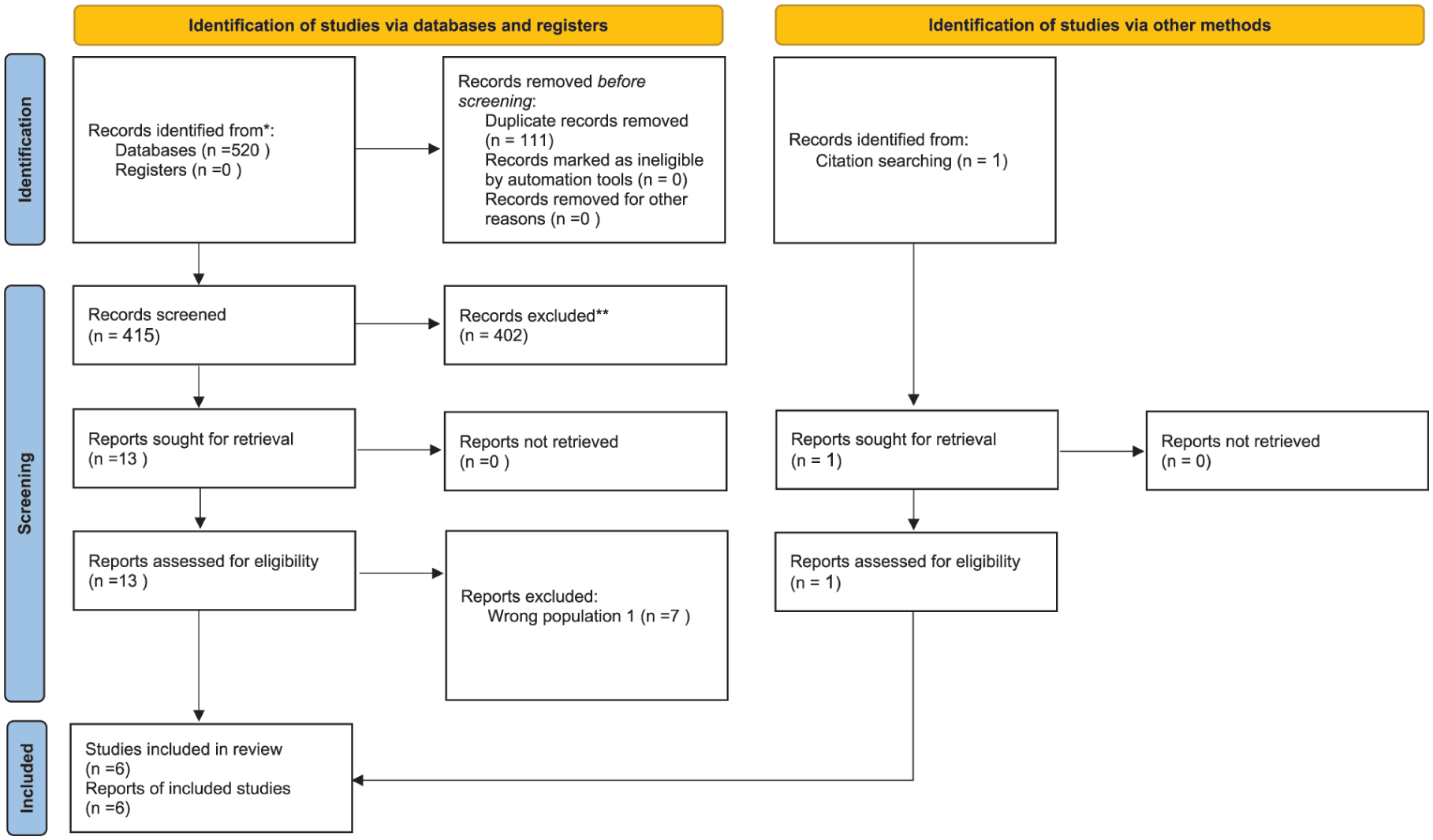
PRISMA 2020 flow diagram for new systematic reviews which included searches of databases, registers, and other sources.
Study characteristics
The six included studies were published between 2003 and 2020 and originated from the Netherlands, Australia, the United States, and Spain. Study designs comprised two case studies, one retrospective clinical report, one feasibility study, and two qualitative investigations. Sample sizes ranged from single cases to a feasibility cohort of 25 mechanically ventilated patients; one retrospective report included a larger mixed cohort, with only a small ventilated subset.
Across studies, individuals received invasive mechanical ventilation via endotracheal tube or tracheostomy during aquatic sessions conducted in intensive care unit hydrotherapy pools, tertiary hospital rehabilitation facilities, long-term ventilation programs, or specialized pediatric prolonged mechanical ventilation (PMV) services. Primary clinical conditions included Guillain-Barré syndrome, chronic spinal cord injury, critical illness polyneuropathy, prolonged mechanical ventilation in children, and complex respiratory insufficiency.
Aquatic interventions included hydrotherapy, aquatic physiotherapy, and structured pediatric aquatic therapy programs, with water temperatures ranging from 32°C to 36°C. Sessions typically involved buoyancy-assisted movement, guided mobilization, supported upright tolerance, respiratory facilitation, and sensorimotor stimulation. All interventions were clinician-led, with multidisciplinary teams including physiotherapists, respiratory therapists, and intensive care nurses providing continuous monitoring of oxygen saturation, hemodynamic status, respiratory patterns, and ventilator parameters. A detailed study-by-study summary is presented in Table 2.
Characteristics of included studies.
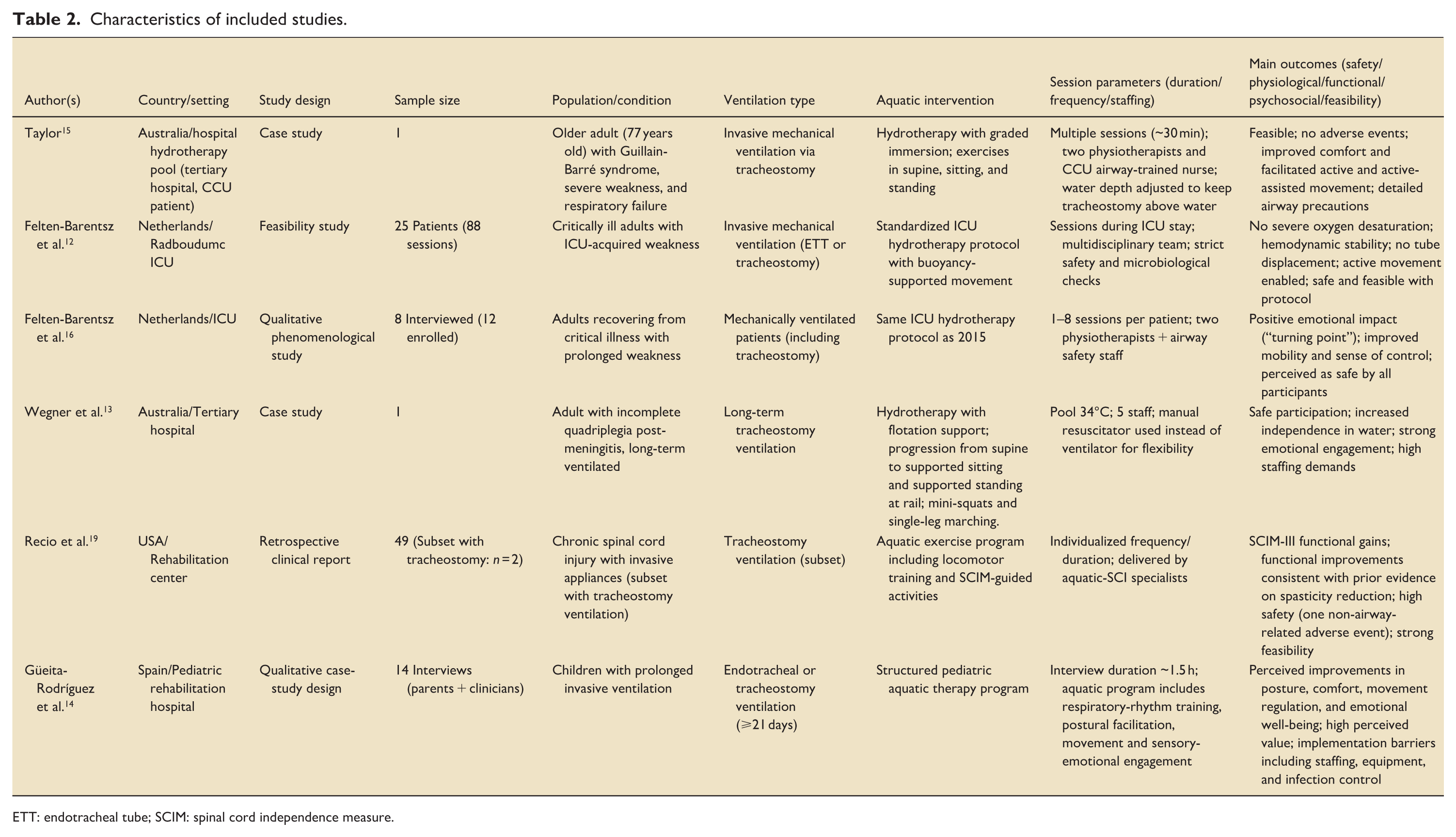
ETT: endotracheal tube; SCIM: spinal cord independence measure.
Methodological quality of included studies
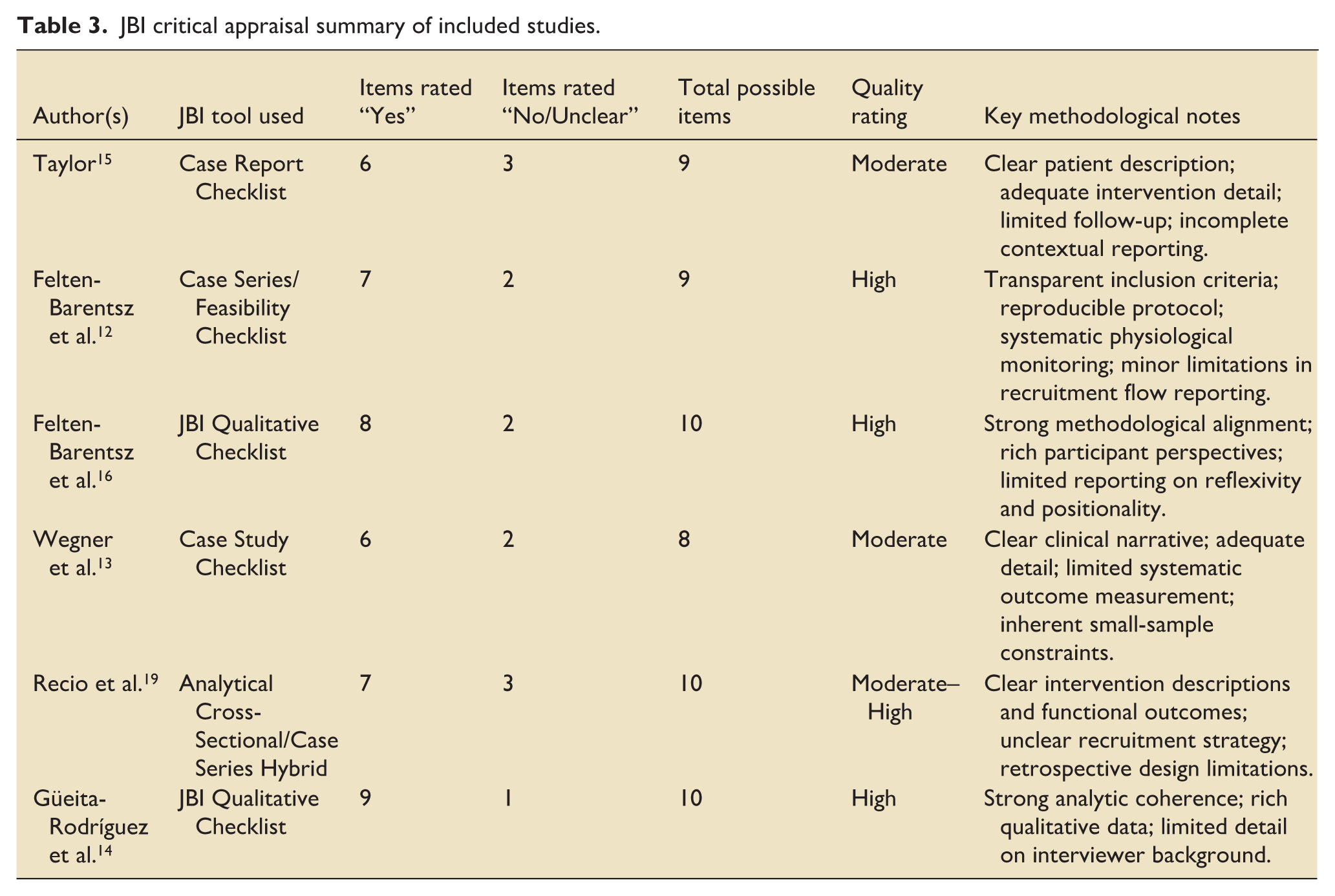
Methodological quality was assessed using the relevant JBI Critical Appraisal Tools. Overall, the evidence base demonstrated moderate to high methodological quality, reflecting the small sample sizes and predominantly descriptive clinical designs.
The case report 15 and case study 13 met core appraisal criteria related to clearly described clinical histories, intervention protocols, and outcome documentation, with limitations including minimal follow-up duration and limited contextual detail.
The feasibility study 12 demonstrated high methodological rigor, including transparent inclusion criteria, a reproducible intervention protocol, and systematic physiological monitoring; minor limitations related to incomplete reporting of participant recruitment flow.
The qualitative studies14,16 met most JBI criteria, demonstrating methodological congruence between research questions, data collection, and analysis, alongside rich representation of participant perspectives, though both provided limited detail regarding researcher reflexivity.
The retrospective clinical report 19 demonstrated moderate to high methodological quality, with clear intervention descriptions and reported functional outcomes, while recruitment procedures were less detailed due to the retrospective design. A summary of appraisal findings is presented in Table 3.
JBI critical appraisal summary of included studies.
Safety outcomes and ventilator management
Across all six studies, aquatic therapy delivered to individuals receiving invasive mechanical ventilation was consistently reported as safe. No study documented airway- or ventilation-related adverse events, including accidental extubation, tracheostomy displacement, ventilator circuit disconnection, or water ingress.
The strongest safety evidence was reported in a feasibility study describing 17 hydrotherapy sessions delivered to five critically ill adults, during which no episodes of oxygen desaturation below 90%, hemodynamic instability, or equipment-related complications occurred. 12 Adult case studies similarly reported stable ventilation and respiratory parameters throughout aquatic sessions, emphasizing careful preparation, secure airway management, and continuous observation.13,15
Ventilator management procedures demonstrated a high degree of consistency across studies. Portable ventilators or ventilator circuits were positioned poolside, with tubing routed and secured to minimize traction, kinking, or accidental disconnection.13,15,19 Predefined criteria for initiating and discontinuing sessions were based on respiratory and hemodynamic stability, with suction and emergency airway equipment prepared in advance. Humidification systems were adjusted when required, and ventilator alarms remained active throughout sessions. 12
In pediatric PMV programs, clearly assigned staff roles supported airway security, continuous monitoring, and manual support in water, with tracheostomy care supplies immediately available at poolside. 14
Feasibility and implementation considerations
Hydrotherapy was consistently reported as feasible for ventilator-dependent individuals when delivered within structured clinical frameworks. The ICU feasibility study documented successful coordination of sessions through predefined inclusion criteria, structured protocols, interdisciplinary staffing, and systematic monitoring procedures. 12
In adult rehabilitation contexts, aquatic sessions were implemented using coordinated clinical teams, secure equipment placement, flotation supports, and individualized manual assistance to facilitate upright activity.13,15 Feasibility within a spinal cord injury rehabilitation program was demonstrated through adaptations such as extended ventilator tubing, careful positioning, and tailored support strategies. 19
In pediatric rehabilitation settings, clinicians emphasized the importance of clear role allocation, immediate availability of suction and emergency equipment, and staff trained in complex airway management. 14 Collectively, these findings indicate that hydrotherapy can be integrated into ICU, inpatient rehabilitation, and pediatric PMV services when appropriate staffing, equipment adaptations, and airway precautions are in place.
Physiological and functional outcomes
Across studies, aquatic therapy was associated with positive physiological and functional responses. In the ICU feasibility study, participants demonstrated stable respiratory parameters and good tolerance of immersion, with buoyancy facilitating mobilization and transitions to upright or semi-upright positions that were difficult to achieve on land. 12
Functional responses were reported across adult case studies, including facilitated active and active-assisted movement, supported standing, improved trunk control, and increased range of motion.13,15 Reduced gravitational load enabled supported standing, assisted stepping, and antigravity movement not feasible in land-based therapy.
In the spinal cord injury cohort, functional changes were reflected in improvements on Spinal Cord Independence Measure (SCIM-III) subscales and enhanced mobility. 19 In children receiving prolonged invasive ventilation, aquatic therapy was associated with improvements in postural alignment, motor coordination, relaxation, and tolerance for supported activity, with immersion facilitating smoother movement organization compared with land-based rehabilitation contexts. 14
Psychosocial and experiential outcomes
Psychosocial and experiential outcomes were primarily described within qualitative and descriptive studies. In an ICU-based qualitative investigation, participants reported increased comfort, reduced fear of movement, and a greater sense of control during aquatic sessions, often describing hydrotherapy as a meaningful turning point following prolonged immobility. 16
Parents and clinicians in pediatric PMV programs described greater enjoyment, relaxation, emotional well-being, and willingness to participate during aquatic sessions compared with land-based therapy. 14 Adult case studies similarly reported increased confidence, relaxation, and enhanced readiness to engage in movement during aquatic interventions.13,15 Across studies, aquatic therapy was associated with positive emotional experiences, increased motivation, and enhanced perceptions of participation and agency.
Discussion
This systematic review synthesized the available evidence on safety, feasibility, and reported physiological/functional and psychosocial outcomes of aquatic therapy for individuals receiving invasive mechanical ventilation. Overall, the evidence base remains sparse, heterogeneous, and predominantly descriptive, spanning ICU, post-acute, long-term ventilation, and pediatric prolonged mechanical ventilation contexts.
Across adult ICU, long-term ventilation, spinal cord injury, and pediatric PMV contexts, several consistent patterns emerged. First, safety outcomes were uniformly favorable: none of the included studies reported airway compromise, ventilator disconnection, accidental extubation, tracheostomy displacement, or water ingress during aquatic sessions. Second, physiological and functional responses were frequently observed, including improved respiratory comfort, smoother ventilatory patterns during immersion, increased active movement, reduced spasticity, and enhanced postural control. These findings are consistent with established hydrodynamic and neuromuscular mechanisms of warm-water immersion described in rehabilitation literature, 3 and may help contextualize observed responses in ventilator-dependent populations. Third, psychosocial and experiential outcomes were consistently positive across the included studies. Adults and children described increased enjoyment, motivation, emotional relief, and enhanced experiences of participation during aquatic sessions. These observations align with broader aquatic rehabilitation literature demonstrating improvements in emotional well-being and reductions in anxiety and depressive symptoms across diverse clinical populations.20–22 Importantly, such evidence provides contextual support rather than direct proof of effectiveness in ventilator-dependent populations.
Finally, all included studies demonstrated feasibility when aquatic therapy was delivered through structured protocols, adequate staffing, appropriate ventilator setup, and continuous physiological monitoring.12–15,19 Taken together, these findings suggest that aquatic therapy can be delivered safely in selected settings when implemented within established services supported by defined protocols and experienced multidisciplinary teams. These observations should be interpreted as hypothesis-generating and not as evidence of safety beyond carefully selected and well-supported contexts.
Taken together, these findings suggest that aquatic therapy may represent a potentially underutilized option in selected settings, with preliminary reported benefits for functioning, participation, and well-being among individuals dependent on invasive mechanical ventilation. These observations should be interpreted as hypothesis-generating rather than as evidence of established effectiveness. However, the predominantly descriptive nature of the evidence underscores the need for more rigorous, systematically designed research.
Interpretation of findings
The findings of this review suggest that aquatic therapy offers a distinctive therapeutic environment for individuals receiving invasive mechanical ventilation. Consistent patterns observed across diverse populations suggest that water-based mechanisms may theoretically support therapeutic responses despite substantial variation in diagnosis and functional status.
Safety as a foundational enabler of participation
The consistently stable respiratory and airway parameters reported across all included studies indicate that, when delivered using structured protocols and skilled interdisciplinary teams, aquatic therapy does not appear to increase clinical risk for individuals receiving invasive mechanical ventilation.12–15,19 These findings challenge prevailing clinical assumptions that aquatic environments inherently pose elevated risk for this population, concerns frequently cited in case-based rehabilitation reports and qualitative accounts.13–15 Instead, the present findings align with broader evidence supporting early, enriched-sensory mobilization for patients with complex medical needs, 23 suggesting that safety may function as a prerequisite for participation rather than a barrier to engagement.
Physiological mechanisms supporting functional engagement
The functional and respiratory responses reported across studies are theoretically consistent with established physiological effects of aquatic immersion, although these mechanisms have not been directly tested in invasively ventilated populations. Hydrostatic pressure may support chest wall mechanics and reduce inspiratory effort, contributing to smoother thoraco-abdominal patterns during immersion. 3 Buoyancy reduces axial loading and facilitates postural activation even among individuals with profound weakness, enabling active and active-assisted movement and supported standing in both adult and pediatric cases. In addition, warm water provides multisensory input that may modulate tone, reduce discomfort, and support more organized motor patterns, as described in aquatic neurorehabilitation literature.3,24
In pediatric populations receiving prolonged mechanical ventilation, these mechanisms align with rehabilitation frameworks emphasizing the importance of sensory- and movement-rich experiences for neurobehavioral regulation and engagement. Evidence from pediatric critical care literature indicates that developmentally appropriate enriched motor experiences may mitigate some adverse effects of prolonged mechanical ventilation and ICU-acquired weakness.9,25
Psychosocial restoration and motivation
Across studies, participants reported emotional and experiential benefits, including feelings of normalcy, autonomy, reduced anxiety, and renewed engagement. These experiences align with rehabilitation literature identifying aquatic environments as psychologically supportive and motivating contexts.22,26 From a motivational perspective, aquatic therapy affords autonomy and perceived competence, key drivers of engagement within self-determination theory. 27 In pediatric settings, caregiver reports of joy, bonding, and relaxation highlight a psychosocial dimension that is often difficult to achieve in conventional respiratory rehabilitation.
Feasibility within real-world clinical constraints
Across the included studies, hydrotherapy was shown to be feasible in diverse clinical environments, including ICU hydrotherapy pools, inpatient rehabilitation programs, long-term ventilation services, and pediatric PMV programs.12–16,19 Although interventions were resource-intensive and required substantial staff coordination, all studies demonstrated that aquatic therapy could be delivered safely when guided by structured workflows, predefined physiological stability criteria, and clearly delineated roles among physiotherapists, respiratory staff, and nursing personnel.
Feasibility in high-acuity ICU settings is particularly noteworthy. Critically ill adults who were unable to tolerate upright positioning or weight-bearing on land were nevertheless able to engage in supported movement and postural activation in water.12,15 Similar feasibility was reported in long-term ventilated adults 13 and in pediatric prolonged mechanical ventilation programs. 14
Collectively, these findings suggest that, under carefully selected clinical conditions, hydrotherapy may be considered as a highly selective adjunct within early mobilization pathways; however, this position remains inferential and requires empirical validation. Notably, all included studies were conducted within established hydrotherapy services or specialized rehabilitation settings.12–16,19 Feasibility demonstrated within such contexts does not necessarily imply broad accessibility. Aquatic therapy in acute and critical care settings requires purpose-built facilities, specialized staffing, coordinated multidisciplinary oversight, and adherence to infection control standards. Such infrastructure is not universally available and varies across healthcare systems, which may limit routine integration into critical care pathways.
Implications for critical care practice and systems
The findings of this review have implications primarily at the level of critical care decision-making rather than routine rehabilitation delivery. Aquatic therapy for individuals receiving invasive mechanical ventilation should be considered a highly selective, resource-dependent intervention situated at the interface between critical care, rehabilitation, and systems capacity.
Across the included studies, aquatic therapy was implemented in carefully selected individuals who demonstrated respiratory and hemodynamic stability, manageable ventilator settings, secure airway access, and the capacity to tolerate transport and immersion without physiological compromise. Patients with unstable cardiorespiratory status, uncontrolled infections, open or unsealed wounds, impaired thermoregulation, high secretion burden, or insufficient airway security were consistently excluded. These exclusion criteria indicate that aquatic therapy is inappropriate for the majority of mechanically ventilated patients and should not be considered in the absence of clear physiological stability and defined safety thresholds12,28 and appropriate tracheostomy management protocols. 29
Safe implementation further depended on substantial system-level resources, including access to a specialized aquatic environment, availability of portable ventilators suitable for poolside use, continuous physiological monitoring, and a multidisciplinary team with clearly delineated roles, consistent with existing professional guidance for aquatic therapy in individuals with tracheostomies 29 and established safety criteria for mobilization in mechanically ventilated patients. 28
Decisions to initiate aquatic therapy required interdisciplinary agreement involving critical care physicians, respiratory therapists, nursing staff, and rehabilitation professionals, with clearly defined lines of responsibility and accountability.
Structured early mobilization in mechanically ventilated ICU populations is guided by internationally published expert consensus safety frameworks that define physiological stability thresholds for active rehabilitation. 28 These frameworks emphasize graded progression, multidisciplinary decision-making, and predefined respiratory and hemodynamic criteria. Within this context, aquatic therapy would not constitute an alternative paradigm, but rather a highly selective adjunct modality that must operate under the same safety principles. In parallel, emerging critical care rehabilitation models increasingly incorporate multimodal and multisensory stimulation approaches aimed at enhancing arousal, engagement, and functional recovery. Although high-quality trials isolating sensory-enriched interventions in invasively ventilated adults remain limited, structured multisensory input is conceptually aligned with broader ICU rehabilitation strategies. Aquatic immersion inherently provides combined tactile, proprioceptive, and vestibular stimuli, suggesting a theoretical compatibility with sensory-enriched rehabilitation models. Preliminary feasibility reports of hydrotherapy in selected ventilated ICU patients indicate that such interventions can be delivered safely within structured early mobilization programs,12,13 although robust outcome data remain sparse.
Despite uniformly favorable safety reports, the evidence does not support aquatic therapy as a standard component of ICU mobilization. The intervention remains resource-intensive, context-specific, and supported primarily by descriptive evidence. Figure 2 synthesizes these considerations into a practice-oriented framework intended to support interdisciplinary clinical judgment rather than prescribe protocolized care.
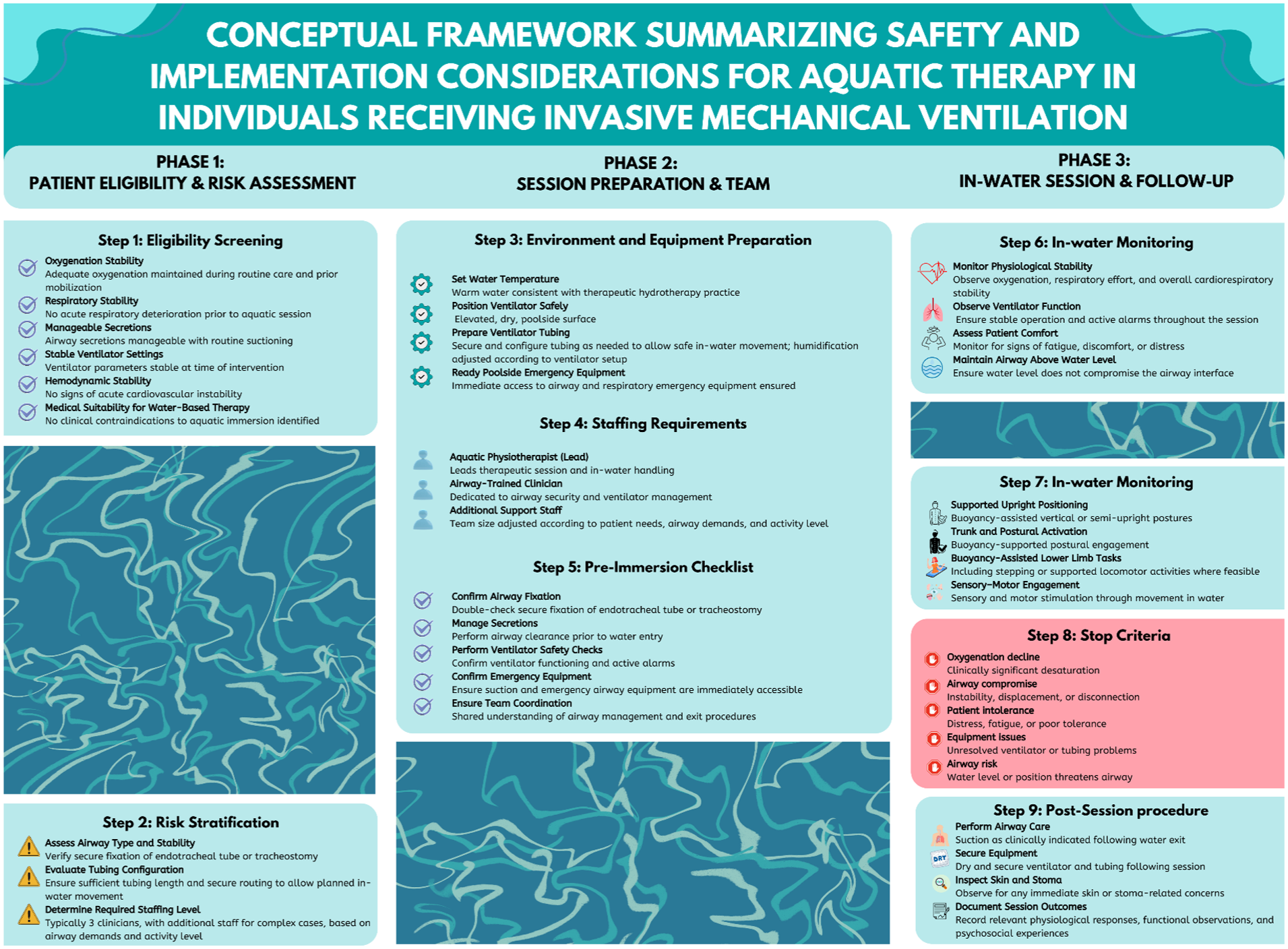
Conceptual framework summarizing safety and implementation considerations for aquatic therapy in individuals receiving invasive mechanical ventilation.
Strengths and limitations of the evidence base
The evidence base for aquatic therapy in individuals receiving invasive mechanical ventilation is still emerging, yet it offers coherent and clinically relevant preliminary insights. A key strength is the convergence of findings across highly diverse clinical contexts, including adult ICUs, long-term ventilation services, spinal cord injury rehabilitation, and pediatric prolonged mechanical ventilation programs. Despite substantial variation in diagnoses, ages, and therapeutic goals, all included studies consistently reported safe implementation alongside positive physiological and psychosocial responses. This convergence suggests that core therapeutic mechanisms of aquatic intervention may plausibly extend across ventilator-dependent populations; however, such applicability remains provisional given the limited evidence base.
An additional strength lies in the qualitative depth provided by two of the included studies.14,16 These investigations illuminate affective, motivational, and relational dimensions of aquatic rehabilitation that are not readily captured through physiological or functional measures alone. Such insights help explain why immersion-based therapy may hold particular value for individuals experiencing prolonged medicalization, dependency, and restricted access to meaningful activity and participation.
However, several important limitations constrain the strength of the current evidence. Most notably, all included studies involved very small samples, with several relying on single-case reports. While such designs are appropriate and necessary at early stages of clinical innovation, they limit inferences regarding treatment efficacy, generalizability, and optimal therapeutic dosage. The absence of comparative or controlled designs further restricts the ability to determine whether observed benefits exceed those achievable through conventional land-based rehabilitation.
Additional limitations relate to marked heterogeneity in intervention protocols. Water temperature, therapist-to-participant ratios, session duration and frequency, therapeutic techniques, and ventilator management practices varied widely across studies. This variability complicates identification of essential intervention components for safety or therapeutic effect and limits reproducibility across clinical settings.
Outcome measurement also lacked consistency. Few studies employed validated functional or patient-reported outcome measures appropriate for ventilator-dependent populations, and only one study 19 used a standardized functional instrument. This inconsistency reduces comparability across studies and hinders cumulative evidence development. Reporting of safety monitoring procedures was similarly variable; although no adverse events were reported, several studies did not clearly specify monitoring thresholds or predefined criteria for session termination, information that is critical for establishing robust safety frameworks in clinical practice.
Finally, most interventions were conducted in well-resourced, specialized centers with substantial staffing and technical capacity. This context limits external validity and raises questions about feasibility in health systems where resources, staffing, or infrastructure may be more constrained.
Taken together, the current evidence base should be viewed as promising but preliminary. It provides a foundational platform for future research and protocol development, rather than definitive evidence of effectiveness.
Strengths and limitations of this review
This systematic review has several methodological strengths that enhance its rigor and transparency. First, the review was prospectively registered in PROSPERO and conducted in accordance with PRISMA 2020 guidelines, ensuring clear documentation of methods and reducing the risk of reporting bias. The search strategy was comprehensive, encompassing six major academic databases without restrictions on language or publication date, and was supplemented by targeted citation tracking. This breadth is particularly important in a field where relevant evidence is sparse and dispersed across multiple clinical disciplines.
Second, the review applied clearly defined PICOS eligibility criteria tailored to the specific clinical characteristics of individuals receiving invasive mechanical ventilation. This approach enabled inclusion of diverse study designs, including case reports, qualitative studies, and feasibility investigations, while maintaining conceptual coherence across populations, interventions, and outcomes. Independent data extraction and JBI-based quality appraisal by two reviewers further strengthened methodological reliability and minimized bias within the review process.
A further strength lies in the analytic approach. Given the heterogeneity and largely descriptive nature of the available evidence, narrative and thematic synthesis represented the most appropriate methodology. Organizing findings into consistent domains (safety, physiological response, psychosocial experience, and feasibility) allowed for a structured and clinically meaningful interpretation of early-stage research in this area.
In addition, although the search strategy was extensive, the review was limited to published literature; unpublished or gray literature could not be systematically identified, raising the possibility of publication bias, particularly in a field where negative or inconclusive findings may be underreported.
Heterogeneity in reporting across included studies further restricted the depth of synthesis. Variability in intervention parameters, staffing models, ventilator configurations, and outcome measures precluded meaningful comparison and prevented formulation of protocol-specific recommendations. Moreover, while qualitative findings enriched understanding of experiential dimensions, the review was unable to conduct participant-level or transcript-level analyses, and thematic interpretations were therefore limited to authors’ reported summaries.
These limitations reflect the developmental stage of the field rather than shortcomings of the review process itself. Accordingly, the findings presented here should be interpreted as a structured consolidation of existing knowledge and a foundation for advancing future research, rather than as definitive evidence of effectiveness.
Future research directions
The findings of this review highlight several priorities for strengthening the evidence base on aquatic therapy in individuals receiving invasive mechanical ventilation. First, controlled and comparative study designs are needed; to date, no randomized, quasi-experimental, or matched-cohort studies have examined this intervention in ventilator-dependent populations. Such designs are required to determine whether hydrotherapy offers effects distinct from, or complementary to, land-based rehabilitation, to identify subgroups most likely to benefit, and to clarify dose-response relationships.
Second, standardized and empirically tested intervention protocols should be developed and validated. Current studies vary widely in eligibility criteria, staffing and role allocation, ventilator management practices, water temperature, therapeutic techniques, and session dosage. Future protocols should specify team roles, poolside ventilator configuration, safety thresholds, termination criteria, and emergency procedures, ideally supported through multicenter collaboration to enhance external validity.
Third, future research should incorporate validated, clinically meaningful outcome measures appropriate for ventilator-dependent adults and children, including respiratory comfort/dyspnea, ventilator-related functional capacity, mobility and postural control, and patient-reported outcomes related to functioning, participation, and well-being. In pediatric settings, parent-reported outcomes warrant particular emphasis.
Fourth, mechanistic studies are needed to clarify how immersion influences respiratory load, ventilatory mechanics, secretion mobilization, and autonomic regulation in invasively ventilated individuals, using instrumented physiological assessment where feasible.
Fifth, pediatric evidence remains limited and should be expanded to include developmental, sensorimotor, emotional, and family-centered outcomes across a broader range of diagnostic groups.
Finally, implementation science approaches are required to evaluate feasibility across health systems, including barriers and facilitators to adoption, resource and staffing implications, training needs, sustainability, and equity of access. Ethical and caregiver perspectives should be integrated, including perceptions of risk and benefit and the impact of aquatic participation on caregiver well-being, using qualitative and participatory methodologies.
Conclusion
This systematic review provides the first comprehensive synthesis of evidence on hydrotherapy for individuals receiving invasive mechanical ventilation. Across six small and predominantly descriptive studies, hydrotherapy was consistently reported as safe and feasible within well-resourced settings, and associated with reported physiological, functional, and psychosocial responses. Although the evidence base remains limited by small samples and predominantly descriptive designs, the convergence of findings across highly heterogeneous contexts highlights the potential of aquatic therapy as a supportive modality for individuals with profound mobility restrictions and complex respiratory needs.
The review underscores the central importance of interdisciplinary collaboration, clearly defined safety criteria, and ventilator-specific adaptations that enable immersion without compromising airway security. At the same time, substantial gaps remain, including the absence of standardized protocols, limited mechanistic understanding, variability in outcome measurement, and a lack of controlled comparative studies. Addressing these gaps through rigorous, systematically designed research will be essential for strengthening the evidence base and informing clinical decision-making.
Taken together, the available evidence is hypothesis-generating and suggests that hydrotherapy represents a promising but still exploratory intervention whose role requires rigorous empirical evaluation before broader clinical adoption can be considered. Continued research, protocol development, and implementation-focused investigation are needed to better define its role within complex respiratory care and rehabilitation pathways, rather than to support routine clinical adoption at this stage.
Supplemental Material
sj-docx-1-inc-10.1177_17511437261452040 – Supplemental material for Aquatic therapy in invasively mechanically ventilated patients: A systematic review of safety, feasibility, and clinical considerations
Supplemental material, sj-docx-1-inc-10.1177_17511437261452040 for Aquatic therapy in invasively mechanically ventilated patients: A systematic review of safety, feasibility, and clinical considerations by Michal Nissim and Yael Megido in Journal of the Intensive Care Society
Supplemental Material
sj-docx-2-inc-10.1177_17511437261452040 – Supplemental material for Aquatic therapy in invasively mechanically ventilated patients: A systematic review of safety, feasibility, and clinical considerations
Supplemental material, sj-docx-2-inc-10.1177_17511437261452040 for Aquatic therapy in invasively mechanically ventilated patients: A systematic review of safety, feasibility, and clinical considerations by Michal Nissim and Yael Megido in Journal of the Intensive Care Society
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.