
Abstract
Background:
Post-extubation dysphagia (PED) is a common complication of critical illness and is associated with aspiration pneumonia, prolonged hospitalisation, and prolonged recovery. Expiratory muscle strength training (EMST) has been shown to improve swallowing function in selected populations, but its role in survivors of critical illness remains unclear.
Objective:
To systematically review the evidence evaluating the effects of EMST on swallowing outcomes in survivors of critical illness with PED.
Methods:
This systematic review was registered with PROSPERO (CRD42023444479) and conducted in accordance with PRISMA guidelines. Searches of MEDLINE, PubMed, EMBASE, CINAHL, and Cochrane databases were performed from 2000 to March 2026. Eligible studies included adult patients requiring >48 h of mechanical ventilation who underwent volitional EMST following extubation. Due to anticipated limited evidence, all quantitative study designs were included. Risk of bias was assessed using the Newcastle–Ottawa scale and the Joanna Briggs Institute checklist. Meta-analysis was not performed due to heterogeneity.
Results:
Three studies met inclusion criteria, including two from the same research group: one case series (n = 2) and two single-group cohort studies (n = 50 and n = 13). All studies reported improvements in swallowing measures, alongside increases in respiratory muscle strength and cough flow. However, EMST was either combined with inspiratory muscle training or other therapies, and no randomised controlled trials were identified. Methodological quality was low, with high risk of bias and absence of comparator groups.
Conclusions:
Evidence supporting EMST for PED in survivors of critical illness is extremely limited and of low methodological quality. Whilst mechanistic plausibility and data from other populations suggest potential benefit, robust randomised controlled trials with standardised training protocols and outcome measures are required before clinical implementation can be recommended.
Keywords
Introduction
Survivors of critical illness frequently experience persistent physical and psychological morbidity following discharge from intensive care.1,2 These sequelae contribute to prolonged recovery, 3 impaired quality of life,4,5 and increased healthcare utilisation and costs, long after the resolution of acute illness.6,7
Among patients who have undergone prolonged mechanical ventilation, post-extubation dysphagia (PED) represents an important complication; the most recent meta-analysis estimates that PED occurs in 36% of patients who underwent endotracheal intubation. 8 PED commonly occurs alongside generalised muscle weakness after critical illness. 9
PED is associated with clinically significant adverse outcomes. Impaired swallowing function increases the risk of silent aspiration 10 and aspiration pneumonia, 11 which in turn may prolong hospital stay 12 and has been related to increased mortality. 13 Beyond respiratory complications, PED has important nutritional consequences; patients deemed unsafe to swallow may be nil by mouth for prolonged periods, and require nasogastric feeding, 14 which carries its own risks and burdens.15–17 In addition, the inability to eat or drink can create new psychological issues, potentially exacerbating distress. 18
A number of interventions have been explored for the treatment of PED, including modification of dietary textures, along with exercises and compensatory manoeuvres. 19 Methods employing neuromuscular stimulation have also been described, 20 and have been shown to improve dysphagia and shorten both ICU and hospital length of stay in extubated patients after an acute stroke. 21
Expiratory muscle strength training (EMST) is a potential treatment for dysphagia, and its use has been described in other patient populations; early data suggested that, compared to sham training, EMST improves swallowing safety in patients with Parkinson’s disease 22 and amyotrophic lateral sclerosis. 23 However, a previous systematic review in non-PED dysphagia demonstrated variation in effectiveness based on the underlying aetiologies, and the methods used to assess swallowing, 24 whereas a network meta-analysis has shown that EMST, alone and in conjunction with other therapies, can prevent aspiration. 25 Furthermore, in patients with swallowing difficulty, EMST improves expiratory muscle strength, without improving pulmonary function. 26
The aim of this systematic review was to synthesise the available evidence examining the effects of expiratory muscle strength training on swallowing outcomes in survivors of critical illness.
Methods
Protocols and registration
This systematic review was registered with PROSPERO, the International Prospective Register of Systematic Reviews (University of York, registration number CRD42023444479), and the protocol has been previously published. 27 The results of this review were reported in line with PRISMA guidelines.28,29
Search strategy
The search strategy was written and performed by two librarians (EB, CT) after consultation with the remaining authors. Papers were restricted to those published in English from 2000 onwards. The search terms are listed in Supplemental file S1. The initial search strategy was performed on 24th November 2024 using Medline, PubMed, EMBASE, CINAHL and Cochrane (Reviews and CENTRAL). A repeat search was performed on the 23rd March 2026. As anticipated in the protocol, a limited number of papers were found with this search strategy (see Figure 1). Therefore, as per protocol, the search strategy was broadened by removing reference to swallowing disorders. However, this did not increase the yield of eligible papers. Hand searching of citation lists and searches in the grey literature were also performed.
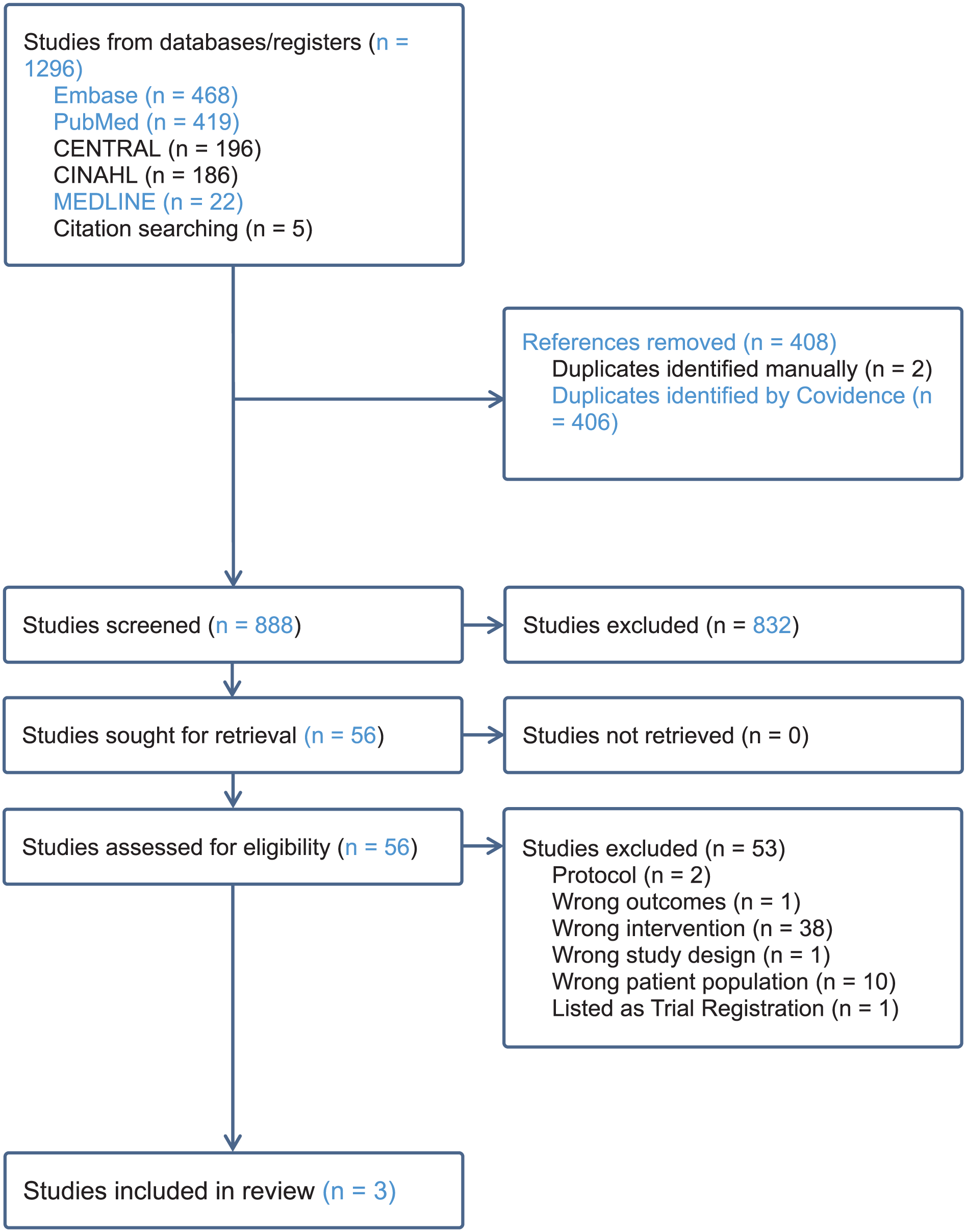
PRISMA diagram.
Study selection
All initial search results were uploaded to Covidence and duplicates removed. Two authors (PT, PS), independently screened titles and abstracts, with disagreements being resolved by a third author (BWJ). There was agreement on 95.6% of abstracts screened (Cohen’s Kappa 0.61). Assessment of the remaining eligible full-text studies was performed, and after further exclusions, data were extracted from the remaining included studies. Figure 1 summarises this process.
Inclusion criteria
Due to the anticipated limited number of studies, we accepted any quantitative study design. The target population was any adult patient over the age of 18, who was admitted to a critical care unit requiring more than 48 hours of mechanical ventilation. All patients were required to be liberated from ventilation and to use volitional EMST devices as the intervention. This included EMST performed alone, or in conjunction with an inspiratory component (inspiratory muscle training, IMT). The training devices could be mechanical (e.g. spring-loaded), or electronic. Training load, expressed as a percentage of the patient’s Maximal Expiratory Pressure (MEP), was extracted, as were the prescribed number of repetitions and sets per day. Comparators included sham training where the person exhales against a negligible resistance, or standard care. Exclusion criteria included patients with spinal injuries, long-term ventilatory support, neuromuscular disorder, pregnancy and known head and neck cancers.
The primary outcomes were any measures used to evaluate swallowing function as defined by the authors of the selected studies, anticipating heterogeneity of measures. Extracted secondary outcome measures included measures of cough function, changes in respiratory strength (Maximum Inspiratory Pressure, MIP, and MEP).
Risk of bias
For non-randomised studies, the Newcastle-Ottawa Scale was used. 30 As we have also included a case report, risk of bias was assessed by the Joanna Briggs Institute’s Checklist of Case Reports. 31 Given the small number and heterogeneity of included studies, formal certainty-of-evidence assessment was not undertaken. Study quality was instead described narratively.
Data extraction
Data were extracted onto a pre-trialled data extraction sheet (Microsoft Excel, USA), by two independent reviewers (PT/PS). The following were extracted: author, year of publication, study design, country of origin, swallowing related outcomes (including method of evaluation and its corresponding results), and respiratory related outcomes. Patient summary data was also collected, in addition to training data, including the type of device used, the number of repetitions and sets, training load, and whether additional interventions were included alongside EMST.
Due to the small number of non-randomised studies, meta-analysis was not performed.
Results
Literature search
Following adoption of the broader search strategy, 1296 citations were identified. After excluding duplicates, 888 abstracts were screened by title and abstract and 832 were excluded. Fifty-six studies were progressed to full-text screening, of which 53 studies were excluded, leaving 3 that were deemed eligible and underwent data extraction. The PRISMA flow chart summarises study selection (Figure 1).
Study summary
Study characteristics are listed in Table 1, and patient characteristics in each study are listed in Table 2. There were no randomised controlled studies. In the first, case reports are described in which two patients with different admission pathologies are trained using both inspiratory and expiratory muscle training devices, in addition to daily swallowing exercises. 32 In the second, a cohort of patients who were mechanically ventilated due to COVID-19 performed combined inspiratory and expiratory training using one device. 33 However, it should be noted that the cohort was split into several treatment modalities, with only 23 of 50 patients performing respiratory muscle training, but outcome measures were not separated by the differing combinations of interventions. The most recent cohort study is written by the authors of the case reports, in which a cohort of 13 patients with dysphagia and Intensive Care Unit Acquired Weakness (ICUAW) perform EMST alone with the swallowing exercises described in the case report. 34 Training regimes are listed in Table 3.
Study characteristics.

CSE: clinical swallow evaluation; FEES: fibreoptic endoscopic evaluation of swallowing; VFSS: video fluoroscopic swallow study.
Patient characteristics.

CSE: clinical swallow evaluation; FESS: flexible endoscopic evaluation of swallowing; ICU: intensive care unit; ICUAW: intensive care unit acquired weakness; NMES: neuromuscular electrical stimulation; RMT: respiratory muscle training; VFSS: video fluoroscopic swallow study.
Values calculated from individual level data provided in the text.
Training regimes.
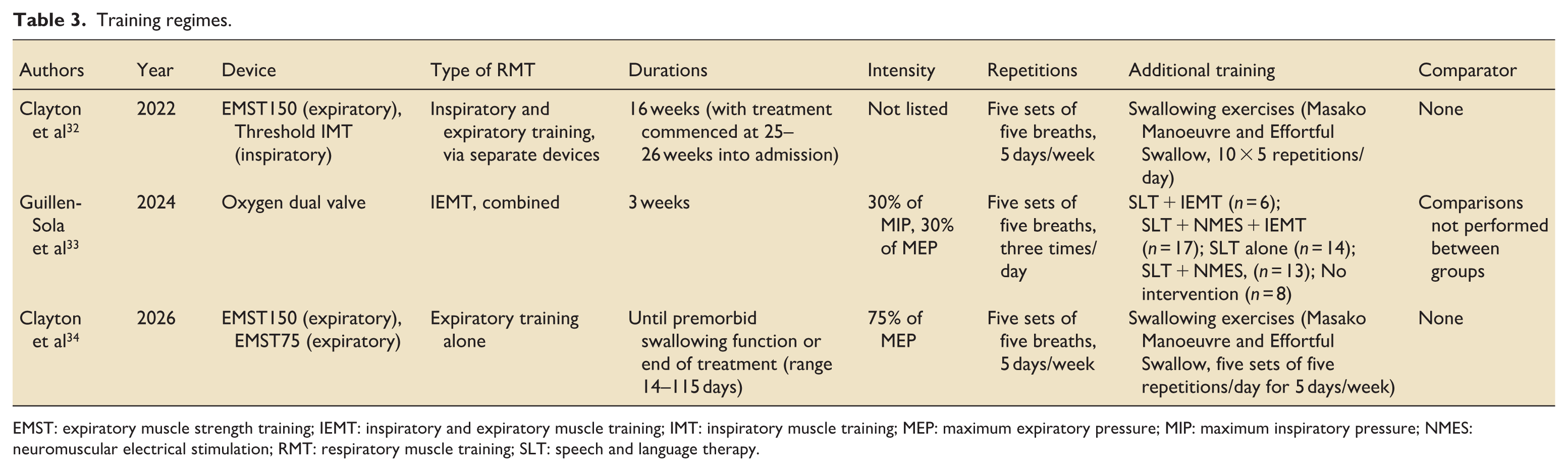
EMST: expiratory muscle strength training; IEMT: inspiratory and expiratory muscle training; IMT: inspiratory muscle training; MEP: maximum expiratory pressure; MIP: maximum inspiratory pressure; NMES: neuromuscular electrical stimulation; RMT: respiratory muscle training; SLT: speech and language therapy.
Outcome measures
All studies reported outcomes in terms of changes in the Penetration Aspiration Scale (PAS) and the Functional Oral Intake Scale (FOIS), with assessment being performed either by Fibreoptic Endoscopic Evaluation of Swallowing (FEES), or by Video fluoroscopic Swallowing Study (VFSS). Additional measures were unique to each study and are listed in Table 2.
Summary results
In both case reports, patients demonstrated an improvement in all swallowing evaluations, and in peak expiratory flow rate (PEF). These are not amenable to statistical analysis, but raw numbers are presented in Table 4.
Results of case reports.

PEF: peak expiratory flow; n/r: not reported.
Guillen-Sola et al demonstrated statistically significant improvements in most swallowing assessments, and in measures of tongue strength and endurance. The sample as a whole had significant improvements in MIP, MEP and peak cough flow (PCF, Table 5).
Summary results of cohort studies.

BRS: bolus residue scale; DOSS: dysphagia outcome and severity scale; FEES: fibreoptic endoscopic evaluation of swallowing; FOIS: functional oral intake scale; MEP: maximal expiratory pressure; MIP: maximal inspiratory pressure; n/a: not applicable; NZSS: New Zealand secretion scale; PAS: penetration–aspiration scale; PCF: peak cough flow; PEF: peak expiratory flow; YPRS: Yale pharyngeal residue scale.
Values derived from individual level data presented within the text.
p-value < 0.001.
Clayton et al reported improvements in swallowing outcomes in a cohort of 13 patients, with all participants demonstrating improvement in PAS, FOIS, New Zealand Secretion Scale (NZSS), and Yale Pharyngeal Residue Scale (YPRS). Formal summary statistics were not reported; however, inspection of individual participant data suggests improvements in median swallowing scores, as well as increases in mean MEP and PEF.
Risk of bias
Risk of bias assessment is presented in Table 6. Methodological quality of studies was low across all studies.
Risk of bias assessments.

Tools used – Joanna Briggs Institute checklist for case reports, Newcastle Ottawa scale for cohort studies.
The case report study demonstrated clear descriptions of the patient demographics and clinical course, as well as their assessment methods and outcome trajectories. However, the intervention was not fully described, limiting reproducibility, and the single-patient design and heterogeneity of the presenting pathology limit generalisation.
Guillen-Sola et al lacked a non-exposed comparator group, and the results are limited as patients were exposed to different interventions, but the results were analysed as a single cohort. Less than half the cohort performed expiratory muscle training, and comparisons between the different exposures were not performed.
Clayton et al included a smaller cohort but with more clinically representative pathologies and adequate follow up. However, as with the other studies, the lack of a comparator group limits interpretation of treatment effects. Overall, all included studies were considered to be at high risk of bias.
Discussion
This systematic review identified only limited evidence in support of expiratory muscle strength training (EMST) for the treatment of post-extubation dysphagia (PED) in survivors of critical illness. Only three eligible studies were identified. The first was a case report describing two patients who demonstrated improvements in swallowing outcomes over a prolonged training period, and when combined with inspiratory muscle training (IMT). The second study reported that combined expiratory and inspiratory training (IEMT), delivered in combination with other modalities such as pharyngeal stimulation and speech and language therapy, was associated with improvements in respiratory muscle strength, cough flow, swallowing function, and physiological measures including tongue strength and endurance. The most recent cohort study found that EMST without IMT, in conjunction with swallowing exercises, can improve swallowing and respiratory function. No randomised controlled trial evidence was identified in the critically ill population.
The physiological rationale for EMST as a potential treatment for PED is supported by mechanistic evidence. For example, studies in healthy volunteers have demonstrated that regular EMST training can lead to hypertrophy of the geniohyoid muscle. 35 Furthermore, electrical activation of the muscles of swallowing during expiratory loading has been demonstrated using surface electromyography. 36 However, PED is multifactorial and it is not simply that muscle atrophy during critical illness leads to PED. 37 Indeed, whilst rapid muscle atrophy is a known consequence of critical illness, and affects numerous muscle groups,38,39 specific atrophy of the muscles of swallowing has not been demonstrated in critically ill patients, although reductions in swallowing muscle size are associated with dysphagia in older people. 40 Furthermore, thickness of swallowing muscle is known to be related to strength of swallowing measures 41
In addition to these changes in muscular structure and function, there is evidence from other clinical populations in support of EMST. Meta-analyses have shown that patients with neurological diseases who were randomised to EMST have lower PAS scores than their controls. 42 In older people, EMST has been identified amongst other behavioural interventions as being effective in treating dysphagia, although the authors recognised the heterogeneity of their populations. 43
Any proposed clinical trial investigating whether EMST can improve swallowing function has certain methodological questions that are not answered by this review. These include the duration of training, the intensity of training and the proposed outcome measures. A systematic review of EMST and its effects on swallowing outcomes across differing patient groups found that there is variation in the duration of training, ranging from 4 to 8 weeks; this is more than what was described in the cohort study, but shorter than the training reported in the case studies. The review found that training sessions were consistent at five sessions per week, with most studies describing an intensity of performing five sets of five breaths per session. 24 In healthy volunteers, EMST performed three times per week for 4 weeks produced similar improvements in MEP to those training five times per week, 44 however the authors acknowledge that patient groups may require different training regimes.
The systematic review also found that there was variation in the expiratory load, ranging from 50% to 75% of a subject’s MEP. In the case report, expiratory load was not reported, and in the study by Guillen-Sola, the initial resistance was set at 30% of MEP. In patients with Parkinson’s disease, such a low resistance has been shown to improve some self-reported domains of swallowing function, compared to a sham training technique. 45 An additional systematic review investigating EMST in acquired motor-based swallowing impairments described that individual studies were consistent in terms of training schedule (five sets of five breaths, 5 days/week) and in terms of training load, with the majority of studies quoting 75% of MEP as the initial load, in keeping with the training regime described by Clayton et al. 26
In two of our reported studies, EMST was combined with inspiratory muscle training (IMT), either through separate devices, or a single device training both phases of the respiratory cycle. In patients with COPD, there were similar improvements in expiratory muscle strength when either separate or combined training approaches were used, compared to IMT alone. 46 IMT alone has been used in patients with dysphagia secondary to ischaemic stroke, demonstrating improved indices of swallowing function, compared to control, and that these improvements in function were correlated with improvements in respiratory function. 47 It is therefore unclear whether survivors of critical illness would benefit from combined approaches.
The most recent cohort study by Clayton et al utilised EMST without IMT but, consistent with their earlier case report, included additional swallowing exercises. Therefore, none of the studies used EMST in isolation, making it difficult to establish the independent contribution of EMST to the observed improvements. Notably, the Masako manoeuvre, used in both of Clayton et al’s studies, is associated with improvements in dysphagia severity in older people. 48
A key consideration is whether EMST can achieve clinically meaningful outcomes in a desired length of time – the median time to resolution of dysphagia after extubation was found to be 7 days, 49 and another study found that, in patients whose dysphagia resolved whilst in hospital, mild PED had a median duration of 3 days, and moderate-to-severe dysphagia had a median duration of 6 days. 12 However, the authors also found that 55% of all patients in the moderate-to-severe group still had dysphagia at discharge.
In contrast, Clayton et al reported high adherence to the intervention (81%–100% of sessions), but treatment duration ranged from 17 to 115 days. This prolonged time may reflect including participants with both dysphagia and ICUAW. Although ICUAW is associated with PED, 9 this is a distinct sub-group of all patients with PED, which limits generalisability.
Importantly, muscle dysfunction in critical illness does not occur uniformly; respiratory and limb muscle weakness may present together or independently.50,51 By extension, PED may occur without ICUAW, and would still require appropriate investigation and treatment.
As these participants with both PED and ICUAW continued to receive treatment until they achieved either the pre-morbid swallowing function, or a plateau in function, the observed improvements may reflect prolonged exposure to treatment.
Furthermore, it has been shown in patients with early FEES assessment (2–4 h post-extubation) swallowing function did improve within the first 24 h of extubation, without intervention. 52 Prolonged intervention, as described in the Clayton (2026) study may not always be feasible. Therefore, any intervention must be sufficiently intense to produce improvements in a short timeframe. Alternatively, patients at risk of prolonged dysphagia need to be identified early, to avoid unnecessary intervention in patients who would recover naturally.
An additional consideration is the sensory component of dysphagia; neuromuscular weakness represents only one of six mechanisms identified in PED, alongside other factors such as altered cognition. 37 In addition to weakness, sensory disturbance of the tongue has been reported after extubation, 53 and loss of laryngeal sensation is associated with aspiration risk and increased secretion burden. 54 Clayton et al. recognise that sensory issues did not always resolve in their cohort of patients, and they suggest additional modalities such as pharyngeal stimulation may be required for sensory disturbance, which would not be targeted by EMST. 34
Future studies must also consider suitable outcome measures. The papers in this review used both VFSS and FEES, and although Penetration-Aspiration Scale (PAS) was common to both, Guillen-Sola described a range of bolus consistencies, whereas this was not specified in the case reports. It has been previously noted in non-critically ill patients that various video fluoroscopic protocols have been described in studies looking at the effects of EMST on swallowing. 24
A systematic review comparing endoscopic to fluoroscopic methods found that whilst there was no significant difference in diagnostic performance, FEES was better at diagnosing both pharyngeal residue and aspiration. 55 However, this was in a mixed patient cohort, none of which were survivors of critical illness. It has been suggested that FEES is a more feasible investigation that can be done at the bedside, without transfer to a radiology suite. 56
Another potential option would be the use of patient reported outcome measures (PROMs). Neither study identified in this review used PROMs, although in a scoping review, only 12 out of 110 papers investigating dysphagia in stroke patients made use of PROMs. 57 Any study investigating interventions for post-extubation dysphagia may benefit from the creation of a Core Outcome Set (COS), combining bedside assessment with “gold-standard” investigations and PROMs. Such COSs have been defined for dysphagia in other patient cohorts, 58 and a Delphi study defining core outcomes for dysphagia after admission to intensive care secondary to cardiac surgery has been described. 59 A randomised controlled trial is currently registered to assess the role of EMST in dysphagia in critically ill patients, using both FEES and self-reported measures of function. 60
Conclusion
This review found only a small number of non-randomised studies that have investigated the use of EMST in survivors of critical illness with post-extubation dysphagia. Although these papers demonstrated improvements in indices of swallowing function, they should be interpreted with caution due to their poor methodologies. Much of the evidence base is related to patients with dysphagia due to long-term pathologies, making it difficult to apply to the critically unwell. Whilst studies are in progress, future studies need to limit the heterogeneity of training stimuli, standardise outcome measures, and evaluate EMST as a standalone therapy.
Supplemental Material
sj-docx-1-inc-10.1177_17511437261444651 – Supplemental material for Effects of expiratory muscle strength training on swallowing in survivors of critical illness: A systematic review and narrative synthesis
Supplemental material, sj-docx-1-inc-10.1177_17511437261444651 for Effects of expiratory muscle strength training on swallowing in survivors of critical illness: A systematic review and narrative synthesis by Philip Skurok, Brian W. Johnston, Emma Brown, Caroline Timothy, Christopher Morse and Peter Turton in Journal of the Intensive Care Society
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.