
Abstract
Background:
Radial arterial catheters are frequently used for monitoring and blood sampling in critical care patients. Ischaemic complications are rare but can cause significant morbidity. The use of vascular ultrasound in critical care is becoming increasingly commonplace. This service evaluation aims to assess the feasibility of training novices in advanced vascular ultrasound assessment, prior to radial arterial cannulation.
Methods:
Over a 4-month period, data was collected from patients admitted to the intensive care unit at the William Harvey Hospital, Ashford, Kent. Ultrasound was used to assess for the presence, size and flow of the radial and ulnar arteries. The assessments were performed by two novice residents in intensive care, who were trained in advanced ultrasound assessment of the radial and ulnar arteries, by an intensive care consultant with expertise in vascular ultrasound.
Results:
One hundred and five limbs were assessed in 53 patients. Novices were deemed to be sufficiently competent, after performing scans on 15 patients over a 2-week period. Satisfactory images were acquired in 100% of patients. The most common finding was a small diameter ulnar artery, present in 30 limbs (29%), while only 1 patient (1%) was found to have an absent ulnar artery. Thirty-two limbs had a radial arterial catheter in-situ. There were no ischaemic complications.
Conclusion:
This service evaluation demonstrates that the training of novices in advanced ultrasound assessment of the radial and ulnar arteries by an intensive care consultant, is feasible. Moreover, this modality may identify patients at risk of critical limb ischaemia. This particular investigation may be considered for incorporation into existing vascular ultrasound assessments.
Background
Radial artery cannulation is a common procedure in the intensive care setting, permitting continual blood pressure monitoring and blood sampling for point of care and laboratory testing. The radial artery is a common choice for arterial cannulation due to its distal location, ease of access and the superficial position of the artery. Another perceived benefit of using the radial artery is the theoretical lower risk of ischaemic complications due to collateral supply via the superficial and deep palmar arches receiving inflow from the ulnar artery. Other common sites for placement of arterial catheters include the femoral, brachial, axillary and dorsalis pedis arteries.
Disruption to or absence of ulnar arterial supply could impair collateral blood supply to the hand and increase the risk of ischaemic complications following radial arterial cannulation. Though rare, there are several case reports of congenitally absent ulnar arteries and the absence of an ulnar artery has been found in 0.015% of cadaveric dissections.1–5 Ulnar collateral supply could also be impeded by other pathologies including atherosclerosis and trauma. Allen’s test, a clinical bedside test first described in 1929 and modified in the 1950s can be performed prior to arterial cannulation to assess the collateral supply from the ulnar artery and a reverse Allen’s test can assess radial supply. 6 Allen’s test however has a low sensitivity, is prone to inter observer variability, is challenging to perform on critically ill patients and is subsequently infrequently performed in this setting. 7 Ulnar collateral flow can also be assessed via angiography or ultrasound (US) however these rarely precede cannulation in an anaesthetic or ICU environment.
Though permanent ischaemic damage has been reported in as few as 0.09% of radial arterial catheter insertions, the impact of ischaemic injury to the hand could be significant in the affected patients. 8 It is likely that there is under-reporting of digital ischaemia on ICU, given the numbers of patients in multiple organ failure (with clinical focus centred on other organ damage) and the high proportion of patients on vasopressor support (a risk factor for distal limb ischaemia). Other potential complications from radial artery cannulation include bleeding, pain, infection, formation of arterio-venous fistulae and thromboembolism. Small radial artery diameter, and an increased ratio of arterial catheter external diameter to vessel diameter have previously been associated with thrombotic complications. 9 Significant numbers of ICU patients may have underlying atherosclerosis, peripheral vascular disease or require vasopressors. These ICU patient groups are at greater risk of limb ischaemia, which may not be appreciated when arterial catheters are initially placed due to the timely need for insertion in critically ill patients.
US is increasingly used in ICU settings for focused bedside investigations, as well as intravenous and arterial cannulations. There have been multiple studies assessing ischaemic complications of radial artery cannulation, and the use of ultrasound to facilitate radial arterial cannulation.10,11 However, there is a paucity of evidence of using US to assess arterial supply prior to cannulation in an ICU setting. It has been shown that US reduces complications with arterial catheter placements compared with the traditional palpation technique however there is currently no accepted ‘gold standard’ method for using point of care US to assess arterial supply prior to radial artery cannulation. 12 It is common practice to use ultrasound to aid in radial artery cannulation on ICU. This service evaluation assesses the feasibility of training doctors in using this ultrasound technique to assess for the presence of ulnar artery, size and colour flow of radial and ulnar arteries in the ICU.
Objectives
To use ultrasound to assess for the presence, size and collateral ulnar arterial flow in ICU patients who have arterial catheters already in-situ or due to be inserted.
To show the feasibility of training ICU doctors in the ultrasound assessment of radial and ulnar artery size and flow.
Methods
Ethical approval was obtained from the East Kent Hospitals University Foundation Trust’s Research and Innovation Department, with a registration number: 2024/GAP/07.
This was a prospective observational service evaluation conducted at the William Harvey Hospital’s intensive care unit – a busy 18 bedded district general hospital ICU serving a mixed adult surgical and medical patient population in Kent, England. Data was collected from patients admitted to the ICU from December 2019 to March 2020. Patients under the age of 18 were excluded. Data was collected for 53 patients in total.
Two ICU junior doctors were trained in vascular ultrasounds over a 2-week period by one FUSIC (Focussed Ultrasound in Intensive Care) supervisor and FUSIC Committee member. During this 2-week period, both doctors were observed and assessed to be competent in the identification of radial and ulnar arteries, measurement of vessel diameter and assessment of flow through the vessels using colour Doppler in 15 patients each prior to data collection. Observation for 15 patients was chosen pragmatically, as this allowed sufficient time to learn the skill and detect any performance errors. The mean time for ultrasound assessment of each limb was also noted for each doctor.
Ultrasound was then used to determine the presence, longitudinal and transverse vessel diameter, colour flow and flow velocities of both radial and ulnar arteries bilaterally in all patients studied. The ultrasound studies were performed using a Sonosite PX ultrasound system (FUJIFILM Sonosite, Inc. 21919 30th Dr. SE Bothell, WA 9802, USA). Basic sonographer training scans were also performed using a Butterfly Handheld Ultrasound device (1600 District Ave, Burlington, MA 01803, USA). These scans were not used for the data represented in the results section (Figures 1–4). Patient notes were also reviewed to determine past medical history, current medications including any vasoactive infusions and any complications associated with the arterial catheter if applicable. Radial and ulnar artery diameters were explored to investigate anatomical variability relevant to risk assessment and were classed as small if the diameter was ⩽0.18 cm. Parametric data are presented as mean (standard deviation). Statistical analysis was performed using paired t-test.
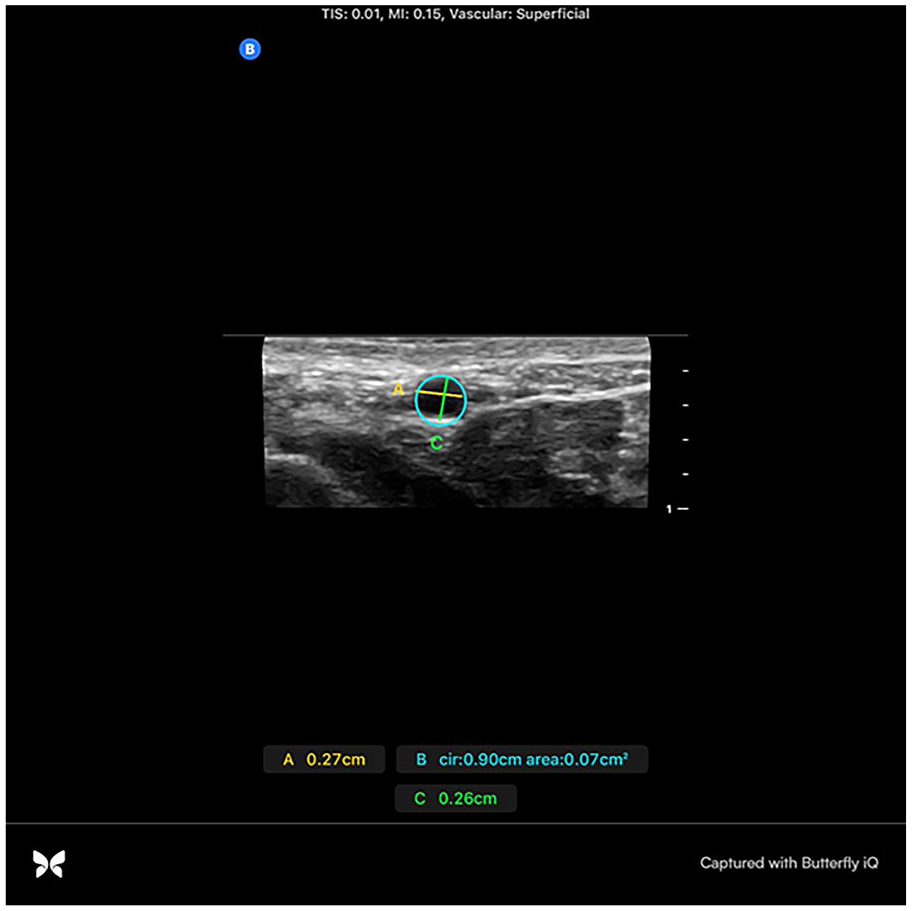
Radial artery elliptical diameter measurement in short-axis.
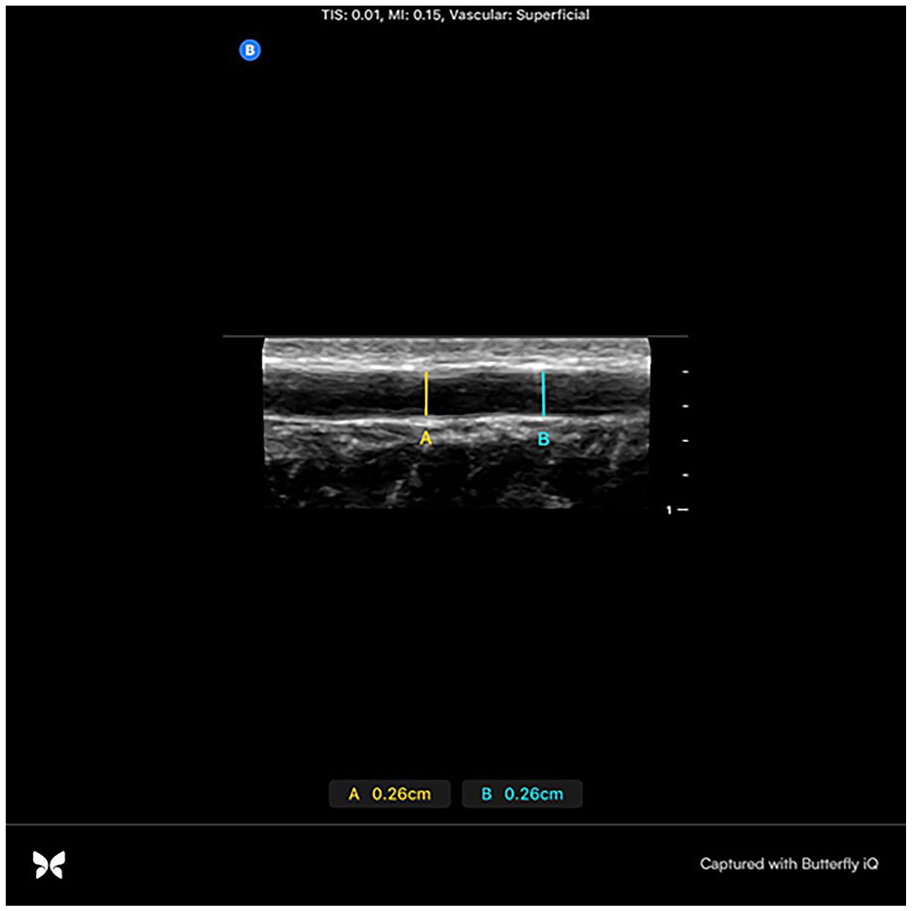
Radial artery diameter measurement in long-axis.
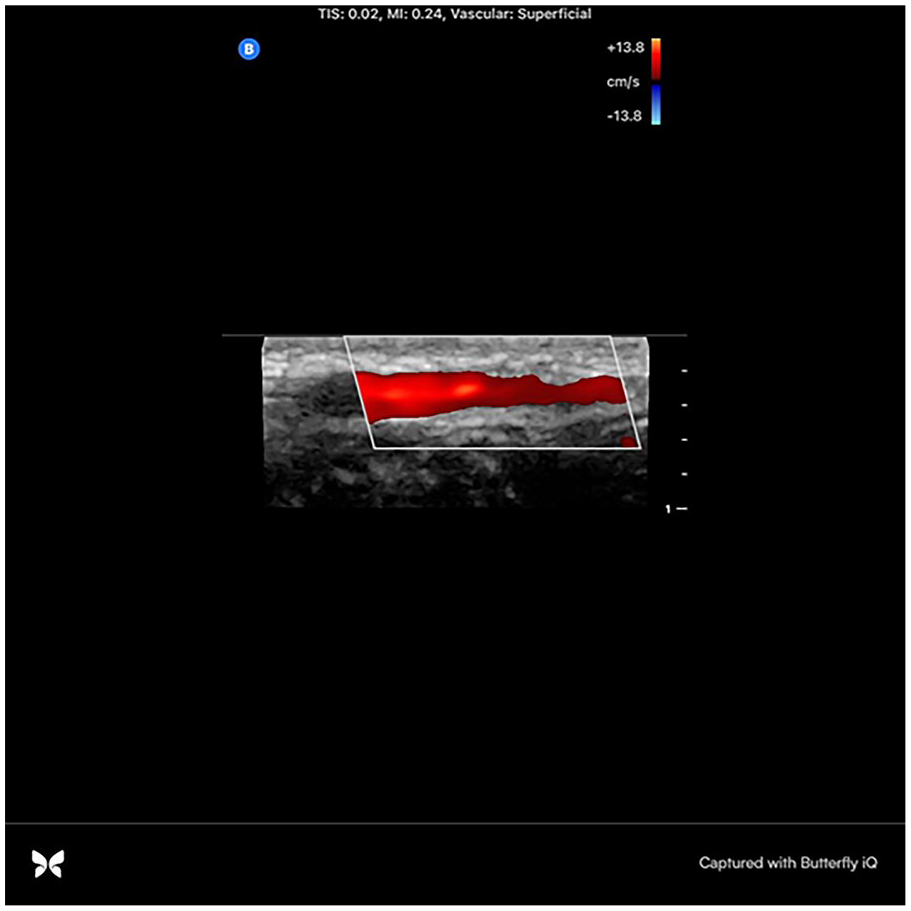
Colour Doppler flow within the radial artery in long-axis.
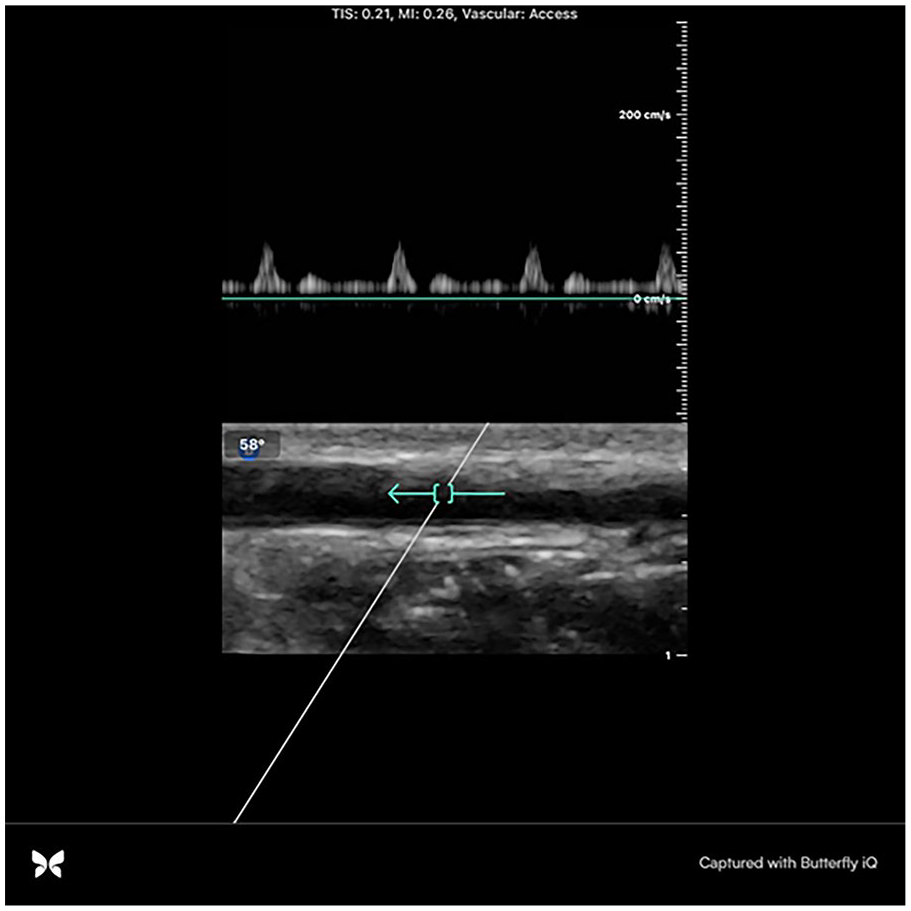
Pulsed wave Doppler flow within the radial artery in long-axis demonstrating good flow at 53 cm/s.
Results
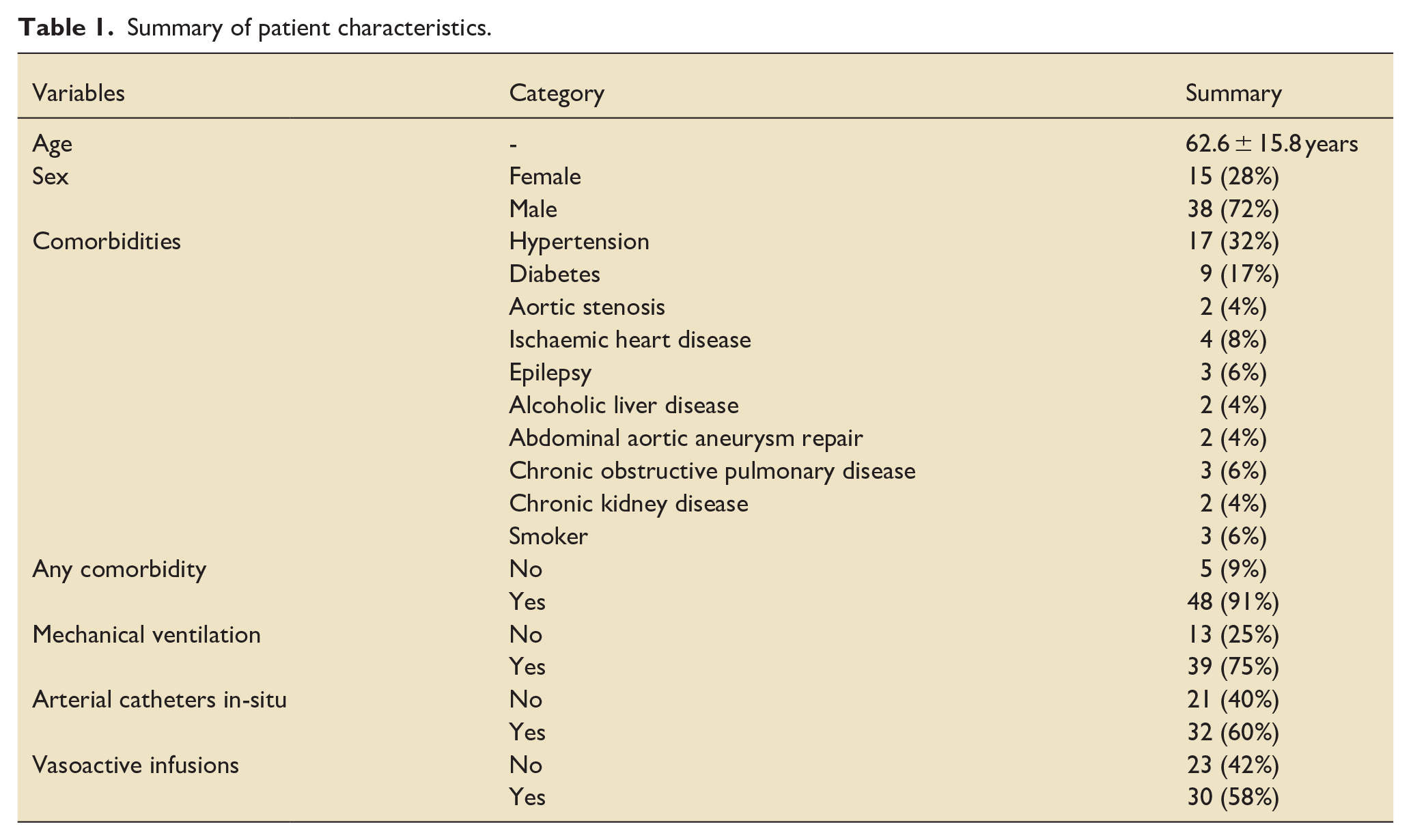
Fifty-three patients in total were included in total and 105 upper limbs were analysed for radial and ulnar arterial presence, diameter and flow. A summary of the demographic characteristics of the patients is shown in Table 1. The population assessed had a mean age of 62.6 years and was mostly male (72%). Ninety-one percent of patients had a major co-morbidity, the commonest of which were hypertension (32%) and diabetes mellitus (17%). Seventy-five percent of patients were mechanically ventilated, and 58% were receiving vasoactive infusions.
Summary of patient characteristics.
The mean time for each doctor to fully assess one limb (presence of ulnar artery, size and flow of both radial and ulnar arteries) was 2 min. Each doctor was deemed as being competent in the vascular ultrasound assessment after a 2-week training period consisting of scanning 15 ICU patients. Once deemed competent, both doctors were then able to independently scan and collect the data. Competency assessment included correct identification of radial and ulnar arteries, correct longitudinal and transverse measurement of both arteries and application of colour doppler over the vessels with accurate grading of colour flow.
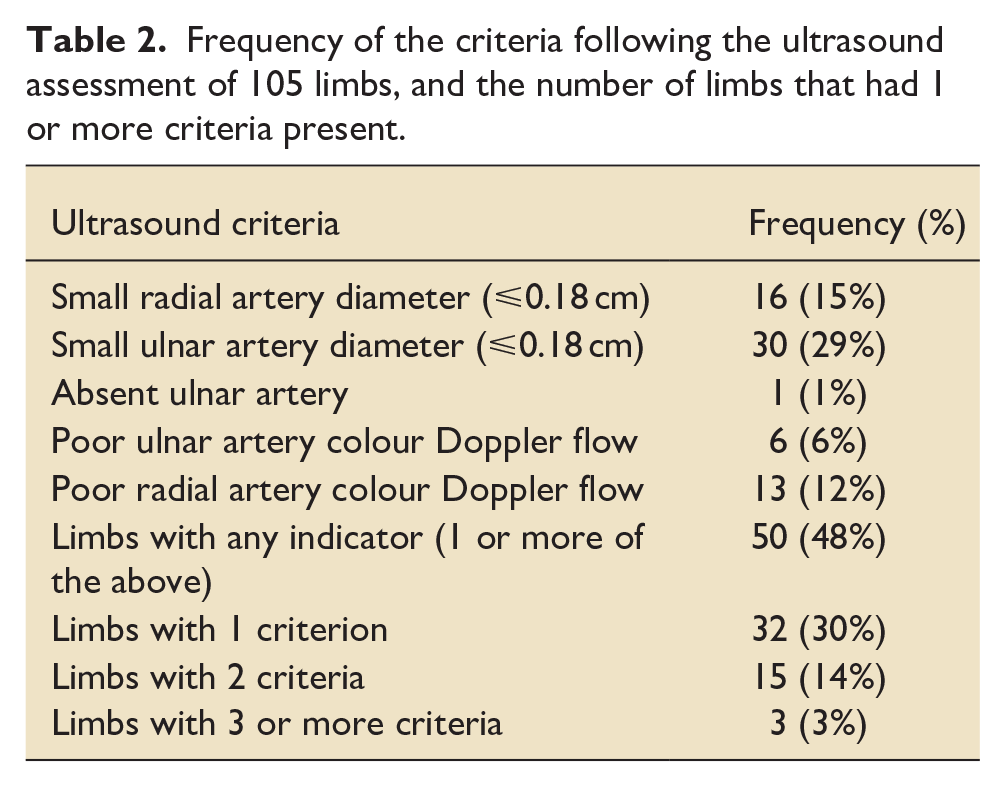
There were 50 limbs in 34 patients that had at least 1 ultrasound criterion identified. The most common criterion, present in 29% of limbs assessed was a small diameter ulnar artery. The least common criterion was an absent ulnar artery, which was found in only 1% of limbs assessed. Of the 50 limbs with at least 1 criterion noted, 32 (64%) possessed only 1, 15 (30%) had 2 and 3 (6%) had 3 or more criteria (Table 2).
Frequency of the criteria following the ultrasound assessment of 105 limbs, and the number of limbs that had 1 or more criteria present.
When reviewing the use of arterial catheters, 34 of the 105 limbs assessed (32%) had a radial arterial catheter in-situ at the time of assessment. The majority of these were in limbs without the ultrasound criteria identified. Thirteen were in limbs with at least one criterion present. There were eight arterial catheters in limbs with one criterion and five arterial catheters in limbs with two criteria. None of the limbs with three or more criteria had a catheter in-situ. There were no ischaemic or major complications from arterial catheters noted in any of the patients studied.
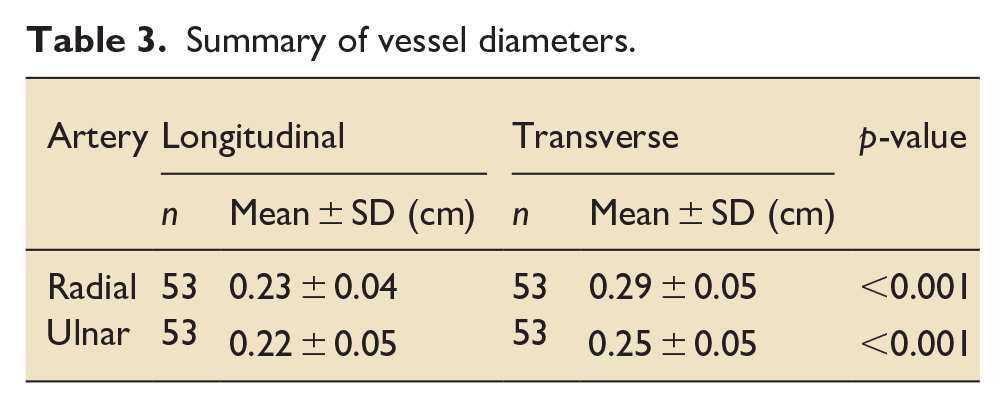
A summary of the vessel diameters is shown in Table 3. There was no difference in the arterial diameter between the left and right side. There was also no difference in diameter between radial and ulnar arteries when measured in the longitudinal axis. When measured in the transverse axis the ulnar artery was smaller than the radial artery (0.25 cm ± 0.05 vs 0.29 cm ± 0.05, p < 0.001). In both vessels the diameters were larger in the transverse axis than the longitudinal axis (0.23 cm ± 0.04 vs 0.29 cm ± 0.05 Radial, 0.22 cm ± 0.05 vs 0.25 cm ± 0.05 Ulnar, p < 0.001). The distribution of the vessel diameters is shown graphically below in Figure 5.
Summary of vessel diameters.
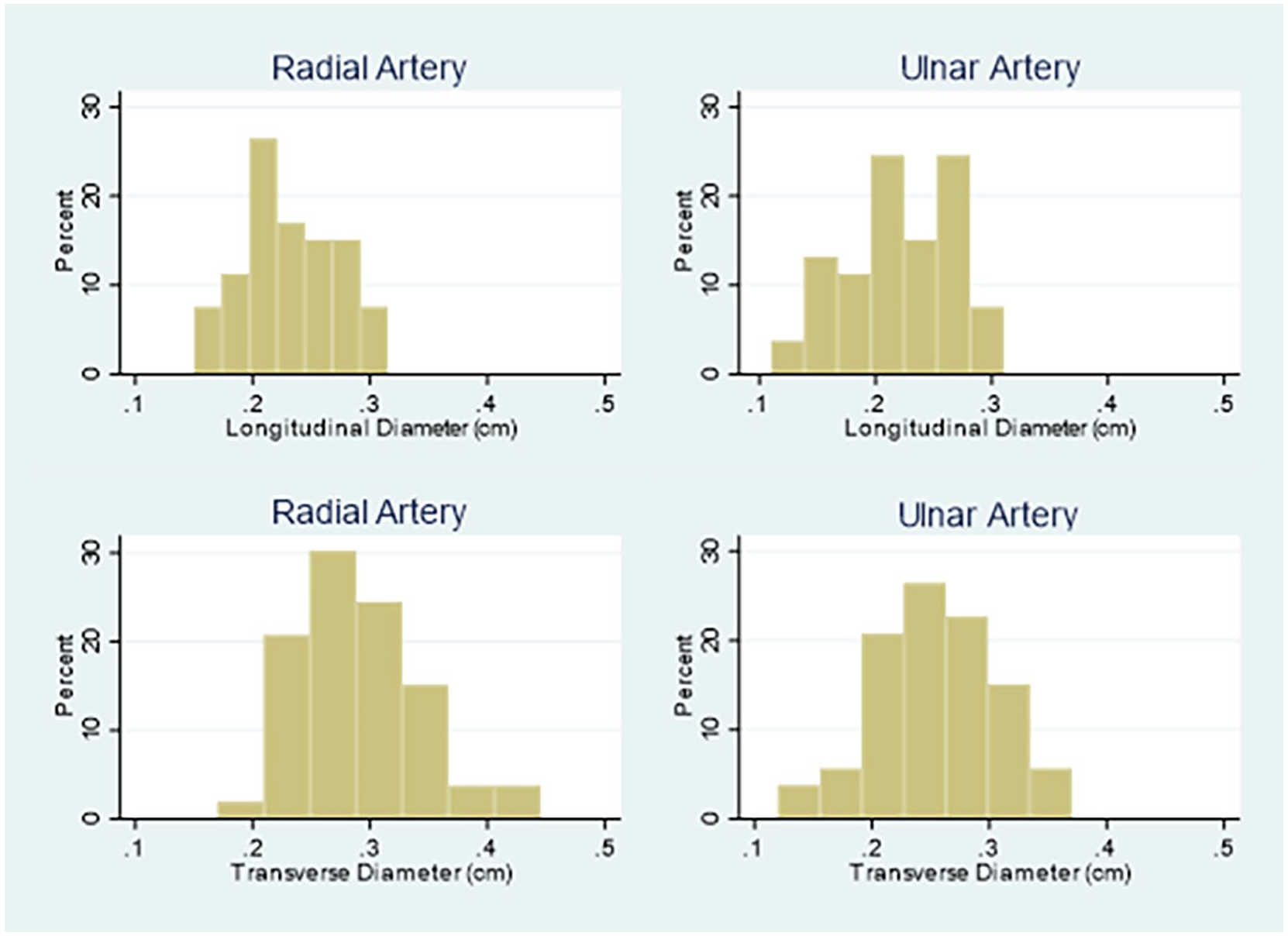
Distribution of measured vessel diameters of the radial and ulnar arteries in the longitudinal and transverse axis.
Discussion
This is the first ICU service evaluation to show that delivering advanced vascular ultrasound assessment by ICU trainees is feasible. The mean time for full vascular assessment by 1 trainee for 1 ICU patient was 2 min, showing this to be efficient, quick, repeatable and facilitated at the patient’s bedside. A 2-week training period was determined to be adequate to obtain competency. This demonstrates that with the guidance of a FUSIC accredited supervisor, competency is achievable. This assessment could be a useful addition to the FUSIC vascular module, especially for use prior to the insertion of radial arterial catheters.
According to literature only 0.09% of patients suffer ischaemic complications following radial arterial catheter placement. 8 These complications can be significant however, resulting in gangrene, compartment syndrome and amputations.13,14 Although the frequency is low, given the high frequency of arterial catheter insertions in ICU and anaesthesia settings both nationally and internationally, the total number of ischaemic events is potentially significant, representing a considerable health and economic burden. 15 This highlights the importance of appropriate risk assessment.
Allen’s test is the clinical test used to assess for adequacy of ulnar collateral blood flow into the hand prior to radial arterial catheter placement and it’s use is well documented. The use of ultrasound to assess the adequacy of flow through cannulated and un-cannulated radial arteries and to assess ulnar artery collateral flow in patients on the intensive care unit has been infrequently described in the literature. This service evaluation looked at 5 ultrasound criteria for radial and ulnar arteries. These measurements have not been validated although could potentially help identify patients at risk of digital ischaemia. This service evaluation was underpowered and so it is unclear as to whether these ultrasound criteria can identify patients at risk of limb ischaemia prior to arterial catheter insertion. Multi-centre studies will be needed to assess these criteria to ascertain whether there is association of risk of limb ischaemia with each criterion.
Regarding defining the size of the radial and ulnar artery for assessment; there is an accepted consensus to use a catheter/vessel ratio of <45% when inserting venous catheters.16,17 Although no such consensus exists for peripheral arterial catheters, radial arterial flow has been shown to be greatly reduced with a catheter/vessel ratio > 45% and there is an increased risk of complications from radial arterial cannulation in vessels with a diameter of <0.2 cm.9,18 The authors suggest therefore, for ease of recall, accepting a catheter/vessel ratio of <50%. Based on this, limbs with vessel diameter ⩽ 0.18 cm were defined as at-risk limbs for ischaemic complications based on the external diameter of a standard 22 g arterial cannula of 0.09 cm. Ultrasound machines now include a software package that delineate the degree that increasing gauges of catheter will occlude a potential site vessel, using accurate measurement functions (GE Healthcare Venue machine – Amersham Place, Little Chalfont, Buckinghamshire. HP7 9NA).
The results presented here revealed that the ulnar arteries were relatively smaller than radial arteries in the group of UK patients studied. This finding has shown to be subject to geographical variation and is of uncertain significance. 19 In the assessment of the 53 patients presented in this study, there were no recorded ischaemic limb complications in any of the patients, including the patients with radial arterial catheters in limbs with multiple risk criteria. This is likely to be due to the small sample size of the study and the low incidence of ischaemic complications as described above, meaning this service evaluation was underpowered to detect ischaemic complications.
Landry et al. found that 80% of patients assessed for finger ischaemia in a single vascular centre were receiving vasoactive medications at the time of diagnosis. 13 In this study 58% of patients were receiving vasoactive infusions, which is a risk factor for digital ischaemia due to the vasoconstriction and/or shocked state of the patient with reduced perfusion to the limbs distally. This highlights the importance of assessing ITU patients for risk of ischaemic complications.
In patients with high vasopressor requirements, distal arterial flow may be compromised leading to lower pressure readings.20,21 Identifying small or poorly perfused vessels using ultrasound could influence the decision to cannulate a more proximal artery, such as the femoral artery, to ensure reliable haemodynamic monitoring and potentially facilitate vasopressor dose reduction. Future studies could assess whether targeted ultrasound assessment prior to cannulation reduces vasopressor dosing by informing site selection.
This service evaluation proposes that vascular ultrasound is easy to learn, non-invasive and quick to use at the bedside to assess the radial and ulnar arterial presence, size and flow prior to radial cannulation. This identification of risk could allow for modification of the approach to reduce ischaemic complications such as alternative vessel or limb selection or enhanced monitoring. A significant proportion of ICU patients have risk factors for limb ischaemia and so assessment in the described method prior to arterial catheter insertion could be an area of research in the future to assess whether there is an association with digital limb ischaemia.
The two trainees who performed the assessments were trained for 2 weeks by a FUSIC supervisor, which the authors feel is an adequate time to be competent in assessing radial and ulnar artery size and flow. The mean time for assessment was 2 min, showing that with adequate training, this vascular assessment can be used for radial arterial catheter insertion in emergent, time-critical scenarios. With the increasing numbers of FUSIC mentors and supervisors throughout the UK, the authors feel that this vascular assessment prior to radial arterial catheter insertion is an achievable and efficient way to reduce potential complications in ICU’s, operating theatres and other locations where these catheters may be inserted. The inclusion of this bolt-on assessment to the FUSIC vascular module would be welcomed.
Limitations
This is a single centre service evaluation that was underpowered to detect ischaemic complications, due to the small sample size and low reported incidence. Although this study identified anatomical features that might increase the risk of ischaemic complications, it did not evaluate the impact of altering cannulation strategies based on these findings. Future studies are needed to determine whether ultrasound-guided site selection improves clinical outcomes, and larger multicentre studies would be needed to develop validated risk prediction tools.
Only one FUSIC supervisor took part in supervision. To minimize subjectivity multiple supervisors should be utilized going forward. The site where the evaluation took place is a busy district general hospital and an out of hospital cardiac arrest centre. A significant proportion of these patients admitted to this ICU will have cardiogenic or distributive shock requiring vasoactive drugs, and/or will have vascular risk factors such as atherosclerosis, peripheral vascular disease and smoking history. These are all risk factors for ischaemia; therefore, the studied population may represent a particularly high-risk group.
This service evaluation focussed primarily on ultrasound identified criteria. A combined ultrasound and patient criteria tool could be more discriminatory in identifying those at risk of ischaemic complications of arterial cannulation. This could be a potential area of future research. The vessel diameter threshold (⩽0.18 cm) used to define ‘small’ arteries was pragmatically selected based on catheter size considerations and existing practices but has not yet been prospectively validated in the context of arterial cannulation.
The assessments utilized a qualitative analysis of colour Doppler to identify flow through the radial and ulnar arteries. Each trainee was taught how to assess flow prior to undertaking the assessments and deemed as competent in doing so prior to data collection, however the subjective nature of this assessment has potential for error or variability in assessment.
Conclusion
This service evaluation has shown that advanced vascular ultrasound can be taught on ICU. It is feasible to teach novices within a 2-week period, with n = 15 patients required for competency. The demonstrable 2-min duration for the assessment highlights that it is a quick, repeatable and simple technique to perform, prior to radial arterial catheter insertions. Future studies are needed to determine whether ultrasound-guided site selection improves clinical outcomes, and larger multicentre studies would be needed to develop validated risk prediction tools.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.