
Abstract
Background:
Intensive care unit (ICU) survivors in the United Kingdom (UK) can receive support from ICU follow-up services in their process of recovery and rehabilitation. However, it is unclear whether the COVID-19 pandemic impacted the ability of UK hospitals to provide follow-up. The objective of this study was to evaluate the provision of follow-up services in the UK for adult survivors of COVID-19 critical illness.
Methods:
All adult National Health Service (NHS) ICUs in the UK were invited to participate. Intensive care clinicians aware of follow-up services offered at their site were invited to complete a self-administered online electronic survey. Free text answers were thematically analysed.
Results:
174 of 242 (71.9%) NHS hospitals responded to the survey. 140 (80.5%) of the respondent hospitals had an ICU follow-up service for survivors of COVID-19 critical illness. A new service was created at 28 (16.1%) hospitals during the COVID-19 pandemic. ICU follow-up services were mostly delivered by nurses (125/140, 89.3%), ICU doctors (111/140, 79.3%), physiotherapists (88/140, 62.9%) and psychologists (59/140, 42.1%). Where ICU follow-up services already existed, changes were made in 111 (79.3%) hospitals during the pandemic and these were maintained in 89 (80.2%) hospitals. Funding was a commonly reported reason for whether follow-up services were offered.
Conclusions:
There was an expansion in the number of ICU follow-up clinics, and the multidisciplinary team delivering post-ICU care to patients who survived COVID-19 critical illness. Many changes to clinic operations introduced during the pandemic persisted, including the use of virtual and hybrid follow-up clinic models.
Introduction
Recovery and rehabilitation after an intensive care unit (ICU) admission are important components of a patient’s journey following critical illness. Patients that have survived critical illness may experience physical, cognitive, and psychological sequelae, which are grouped together under the umbrella term Post Intensive Care Syndrome (PICS). 1 Large numbers of patients were admitted to ICU with COVID-19 critical illness and survived to hospital discharge, and the resulting impact on ICU follow-up services has been significant.2 –4 Many of the symptoms experienced as sequelae of COVID-19 critical illness are also present in PICS.1,4 However, the unique factors of the global pandemic are thought to have an additional, multi-factorial impact. Prolonged ICU admission, reduced family contact and social isolation pre- or post-ICU, may have contributed to deteriorations in patients’ mental health.5,6 Furthermore, the physical effects of prone position ventilation and prolonged duration of mechanical ventilation may have increased the need for physical rehabilitation services. Together these factors may have impacted on the independence of patients, their ability to engage in leisure activities and likelihood of return to employment.4,7
ICU follow-up is recommended by the National Institute for Health and Clinical Excellence (NICE) for patients who have an ICU admission of more than 4 days and are considered at risk for PICS. 8 Risk factors for the development of PICS include physical and non-physical factors, including the presence of pre-existing respiratory problems, restricted mobility, intrusive memories, anxiety or panic attacks.8,9 It is recommended that ICU follow-up consists of an appointment with a multi-disciplinary team, 2–3 months following discharge from hospital. 10 However, during a nationwide evaluation of provision of ICU follow-up services in 2020, 27.8% of the 176 respondent ICUs did not offer any ICU follow-up, with multiple limiting factors identified, including lack of funding, shortage of personnel, and infrastructure issues. 7 Furthermore, where ICU follow-up was provided, the services offered were not standardised.7,11,12 Although there is limited evidence demonstrating the benefit of ICU follow-up, the burden of PICS is clear. When survivors of COVID-19 critical illness were assessed 6 months after hospital discharge, psychological distress was prevalent in 12%–32%, 13%–17% had evidence of cognitive impairment and 9%–13% reported symptoms of breathless and fatigue. 2 In addition, at 12 months post-ICU discharge, anxiety, depression and symptoms of post-traumatic stress disorder (PSTD) were found in 24%–43% of survivors of COVID-19 critical illness. 13
Specific follow-up offered to survivors of COVID-19 critical illness has not yet been investigated, particularly within the context of challenges in providing intensive care in a pandemic.7,14 The aim of this study is to evaluate the provision of follow-up services in the UK for adult survivors of COVID-19 critical illness.
Methods
Survey development
The content and format of the survey was designed by the investigators (AACW and BC) to expand upon previous national surveys assessing ICU follow-up services.7,11,12 The survey was iteratively developed. Adaptive questioning was utilised and all survey questions were available on one page. Questions were ordered serially, with single- or multiple-choice questions requesting information about the hospital, professionals involved in ICU follow-up services and service reconfiguration during the pandemic. Free text spaces allowed respondents to provide hospital and contact details, information about changes made to their local follow-up services and additional information to single-/multiple-choice responses. A minimum of 11 questions were posed. The survey was pilot tested by two ICU research nurses and a medical physician, to ensure it was functional and that questions were comprehensible and sensible. The final survey was approved by AACW, BC and IW. The survey (see Supplemental Material) took less than 5 min to complete. Respondents were able to review and alter their answers prior to survey submission. Completion of the survey was taken as implied consent for participation, as per ethical approval by the Health Research Authority (East Midlands - Derby Research and Ethics Committee, reference 20/EM/0247). 15 The survey was hosted by REDCap at the University of Liverpool.16,17
Definitions
During the COVID-19 pandemic, follow-up clinics were created by medical specialists for patients to attend after a hospital admission due to COVID-19 illness. In the survey, this type of follow-up is referred to as ‘non-ICU COVID-19 follow-up’ and is enquired about, separate to ICU follow-up services.
Identification of hospitals
Intensive care units and high dependency units (HDUs) at 242 NHS hospitals were identified, which contribute to the Intensive Care National Audit and Research Centre (ICNARC) Case Mix Programme and the Scottish Intensive Care Society Audit Group.18,19 NHS Trusts serve geographical regions within the UK and there may be multiple hospitals within a single Trust. The 242 hospitals identified were located at 155 NHS Trusts. All hospitals were invited to participate in the survey.
Survey distribution
The survey was shared via the UK Critical Care Research Group mailing list, social media including X (previously Twitter), regional WhatsApp groups for intensive care clinicians and was shared with study teams participating in the PIM-COVID study, a multicentre, observational, longitudinal study to assess the psychological outcomes of patients that survived an ICU admission for COVID-19. 15 The survey was also publicised at the Intensive Care Society’s State of the Art Congress in June 2023. A snowballing approach was also embedded whereby colleagues were encouraged to promote the survey to colleagues in other hospitals. Where a response was not obtained for a hospital, the ICU team was contacted directly to highlight the opportunity to participate in the survey. Contact was made by email, where an email address for a follow-up service was available online or by phone, via the hospital’s switchboard. The survey was voluntary, with no incentive for completion. Information was included at the start of the survey in lieu of an information sheet. Any member of the ICU multi-disciplinary team who could answer questions related to the follow-up service at their site, was invited to complete the survey. The required number of responses was determined a priori, with >70% being the desired response rate. 20 The survey ran from April to November 2023, with each respondent being recontacted at least once if no response was received in the initial survey wave.
Data management and analysis
Responses were screened manually for duplicates and amalgamated where appropriate. Sites were contacted for clarification if there were conflicting answers from multiple respondents. For incomplete survey responses, respondents were contacted regarding missing or conflicting data via email or telephone and entries were corrected. Survey responses were saved onto password-protected devices and documents. Descriptive statistics were used to analyse the quantitative data using Microsoft Excel (Microsoft Corp, Redmond, WA, USA). Quantitative data are reported as n (%). Qualitative free-text data was thematically analysed by two researchers (CO and JXY), who independently coded the free-text answers and subsequently met to create a shared coding frame to generate descriptive themes. 21 The data were then reanalysed with the shared framework and the final analytic themes were jointly agreed by CO, JXY and AACW.
Patient and public involvement
The public were involved in the development of the PIM-COVID study through input from members of ICUSteps, a peer support charity for patients, family members and carers who have been directly or indirectly impacted by an ICU admission. The trustees of the charity are 50% ICU patients or family members. ICUsteps also has research volunteers, who are a mix of patients and relatives. The research manager for ICUsteps asked the trustees and research volunteers for feedback on all documentation for the PIM-COVID study and any comments were sent to the study organisers.
Results
Responding institutions
In total, 174 of 242 (71.9%) individual NHS hospitals responded to the survey. These hospitals were located in England (where 138/193 [71.5%] hospitals with an HDU/ICU responded), Scotland (19/26 [73.1%] hospitals responded), Northern Ireland (9/9 [100.0%] hospitals responded), and Wales (8/14 [57.1%] hospitals responded). Hospital categories for which responses were provided included district general hospitals (107/174, 61.5%), university teaching hospitals (55/174, 31.6%), and specialist centres (9/174, 5.2%). The survey responses accounted for 123 (79.4%) NHS Trusts across the UK. There were 16 duplicate responses. The professions of survey respondents are provided in Table S1 in the Supplemental Material.
ICU follow-up service availability
An ICU follow-up service that survivors of COVID-19 critical illness could access was available in 140 (80.5%) UK hospitals. Examining this availability at a national level, amongst hospitals with an HDU/ICU, eight (88.9%) hospitals offered an ICU follow-up service in Northern Ireland, 113 (81.9%) in England, six (75.0%) in Wales and 13 (68.4%) in Scotland.
An existing ICU follow-up service was already in place in 112 (64.4%) UK hospitals prior to the COVID-19 pandemic; in six (75.0%) hospitals in Wales, 95 (68.8%) hospitals in England, nine (47.4%) hospitals in Scotland and two (22.2%) hospitals in Northern Ireland. As such, a new ICU follow-up service was created in 28 (16.1%) hospitals (18 in England, six in Northern Ireland, four in Scotland) during the COVID-19 pandemic.
ICU follow-up service structure
Table 1 outlines the characteristics of the ICU follow-up offered to survivors of COVID-19 critical illness. Multiple eligibility criteria were used by 76 (54.3%) ICU follow-up services, and as such the sums of reported percentages are greater than 100%. The most common characteristics determining invitation to ICU follow-up clinic were referral by a clinician (36.4%) or an ICU admission of ⩾ 72 h (30.0%). At 26.4% of ICU follow-up clinics, all survivors of COVID-9 critical illness were invited, whilst 17.9% allowed patients to self-refer.
Characteristics of ICU follow-up services offered to survivors of COVID-19 critical illness.
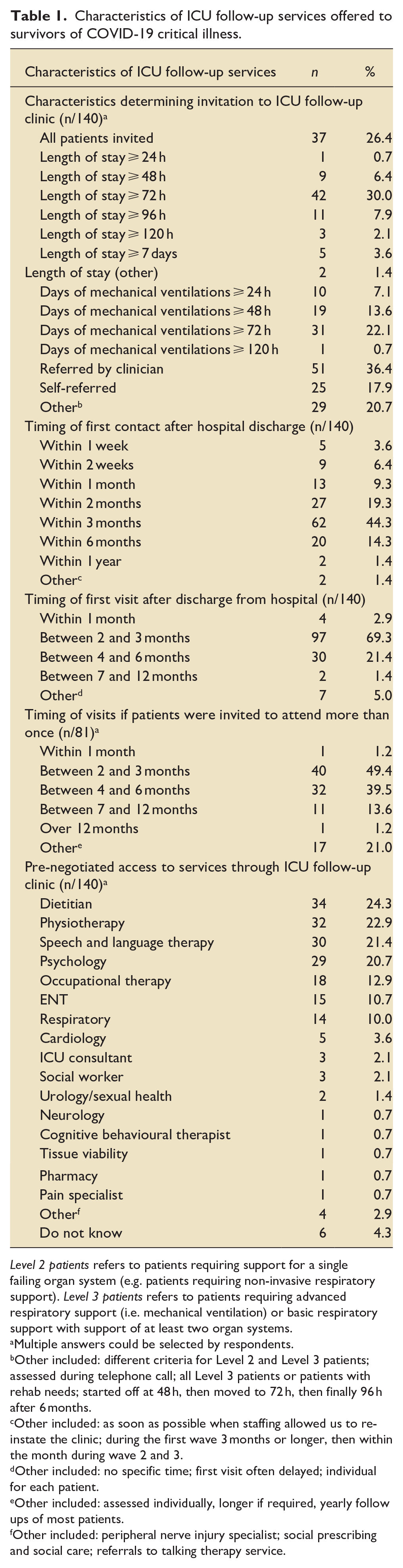
Level 2 patients refers to patients requiring support for a single failing organ system (e.g. patients requiring non-invasive respiratory support). Level 3 patients refers to patients requiring advanced respiratory support (i.e. mechanical ventilation) or basic respiratory support with support of at least two organ systems.
Multiple answers could be selected by respondents.
Other included: different criteria for Level 2 and Level 3 patients; assessed during telephone call; all Level 3 patients or patients with rehab needs; started off at 48 h, then moved to 72 h, then finally 96 h after 6 months.
Other included: as soon as possible when staffing allowed us to re-instate the clinic; during the first wave 3 months or longer, then within the month during wave 2 and 3.
Other included: no specific time; first visit often delayed; individual for each patient.
Other included: assessed individually, longer if required, yearly follow ups of most patients.
Other included: peripheral nerve injury specialist; social prescribing and social care; referrals to talking therapy service.
Most patients were contacted by ICU follow-up teams within 3 months of hospital discharge (82.9%), whilst 10% of follow-up teams contacted patients within 2 weeks of hospital discharge. The most common timing of an initial ICU follow-up clinic visit was between 2 and 3 months (69.3%). In 81 (57.9%) hospitals, survivors of COVID-19 critical illness were invited to attend more than one ICU follow-up clinic appointment.
Where professions are not part of the ICU follow-up team, pre-negotiated access to specialist services may have been arranged locally. This allows direct referral by the ICU follow-up team instead of a patient needing to be referred by their general practitioner. The most common pre-negotiated access to specialist services was to dietitians (24.3%), physiotherapists (22.9%), speech and language therapists (21.4%) and psychologists (20.7%).
Professions involved in delivery of ICU follow-up clinics
In 126 (90%) hospitals, the ICU follow-up service involved a multi-disciplinary team (MDT). Table 2 outlines the professions involved, which ranged from two professions in 22.1% of hospitals to 13 professions at one hospital. The members of the MDT most commonly present in ICU follow-up clinics were nurses (89.3%), ICU doctors (79.3%), physiotherapists (62.9%) and psychologists in 42.1% of ICU follow-up clinics. Figure 1 illustrates the new professions added to existing follow-up services during the COVID-19 pandemic. The most common additions were occupational therapists (11 hospitals), physiotherapists (10 hospitals), psychologists and respiratory physicians (both, eight hospitals).
Professions involved in UK intensive care unit (ICU) follow-up clinics.
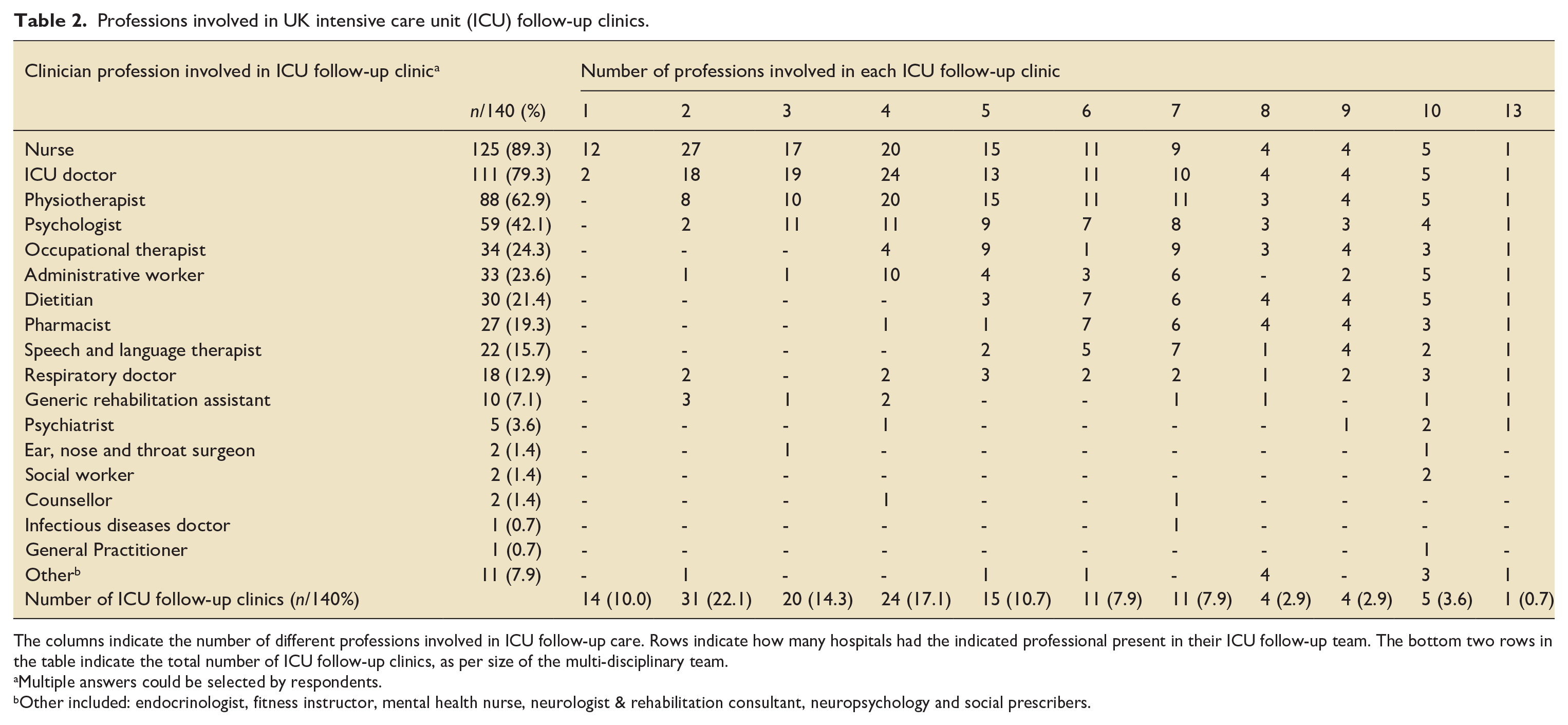
The columns indicate the number of different professions involved in ICU follow-up care. Rows indicate how many hospitals had the indicated professional present in their ICU follow-up team. The bottom two rows in the table indicate the total number of ICU follow-up clinics, as per size of the multi-disciplinary team.
Multiple answers could be selected by respondents.
Other included: endocrinologist, fitness instructor, mental health nurse, neurologist & rehabilitation consultant, neuropsychology and social prescribers.
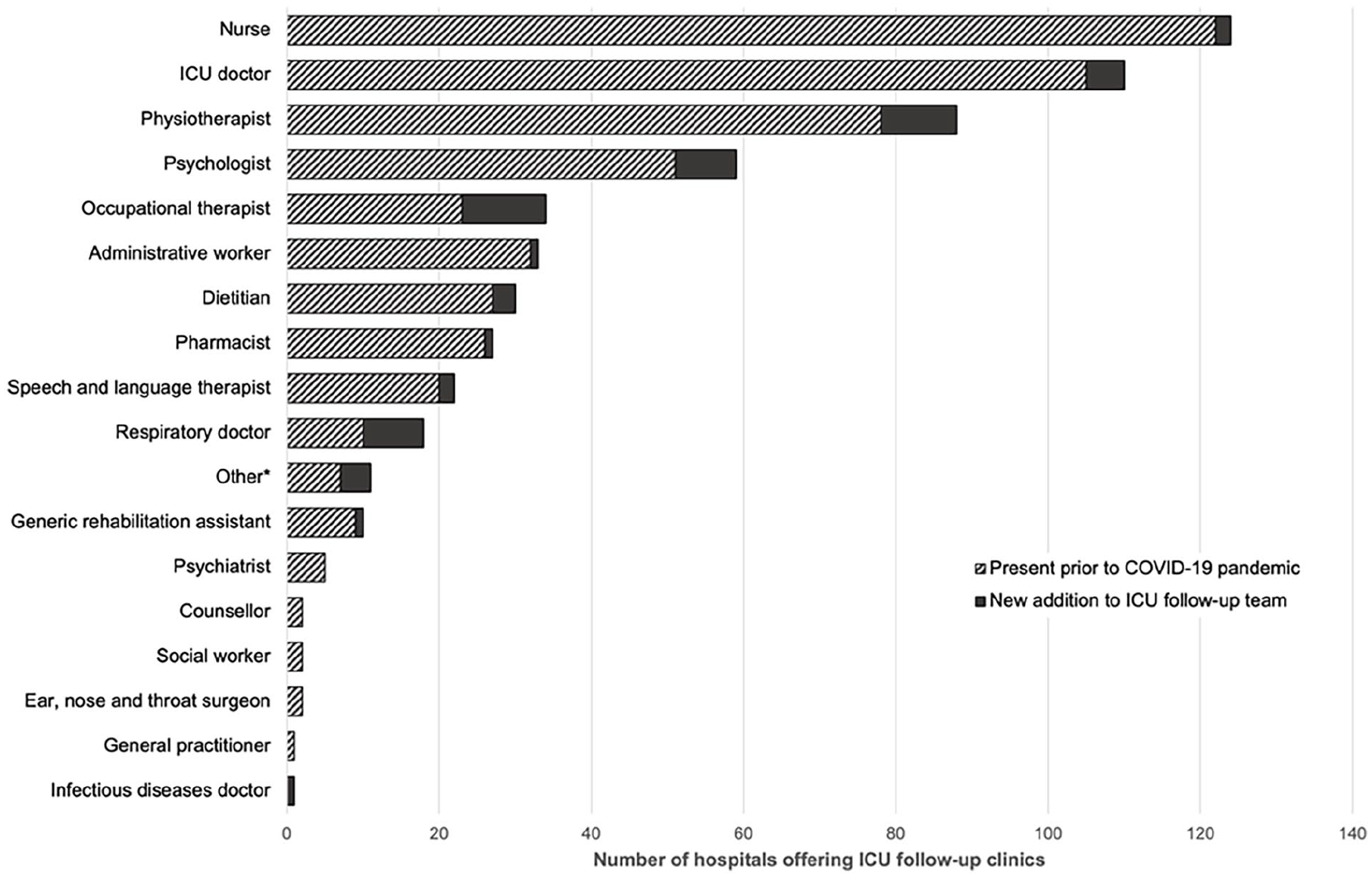
New additions to ICU follow-up services by profession during the COVID-19 pandemic.
Non-ICU, COVID-19 follow-up services
In total, 72 (41.4%) hospitals had a non-ICU, COVID-19 follow-up clinic that survivors of COVID-19 critical illness were invited to attend. A non-ICU follow-up service was not offered at 89 (51.1%) hospitals, while 13 (7.5%) hospitals responding to the survey did not know if there was a separate non-ICU, COVID-19 follow-up clinic. Amongst the 34 hospitals that did not have an ICU follow-up service, survivors of COVID-19 critical illness at 11 (32.4%) of these hospitals were not offered any follow-up, whilst those at the remaining 23 (67.6%) hospitals were followed up by a non-ICU follow-up service. The most common profession to lead a non-ICU COVID-19 follow-up clinic was respiratory physicians, in 62 (86.1%) of the 72 hospitals offering this service (see Table 3).
Non-ICU, COVID-19 follow-up services. a
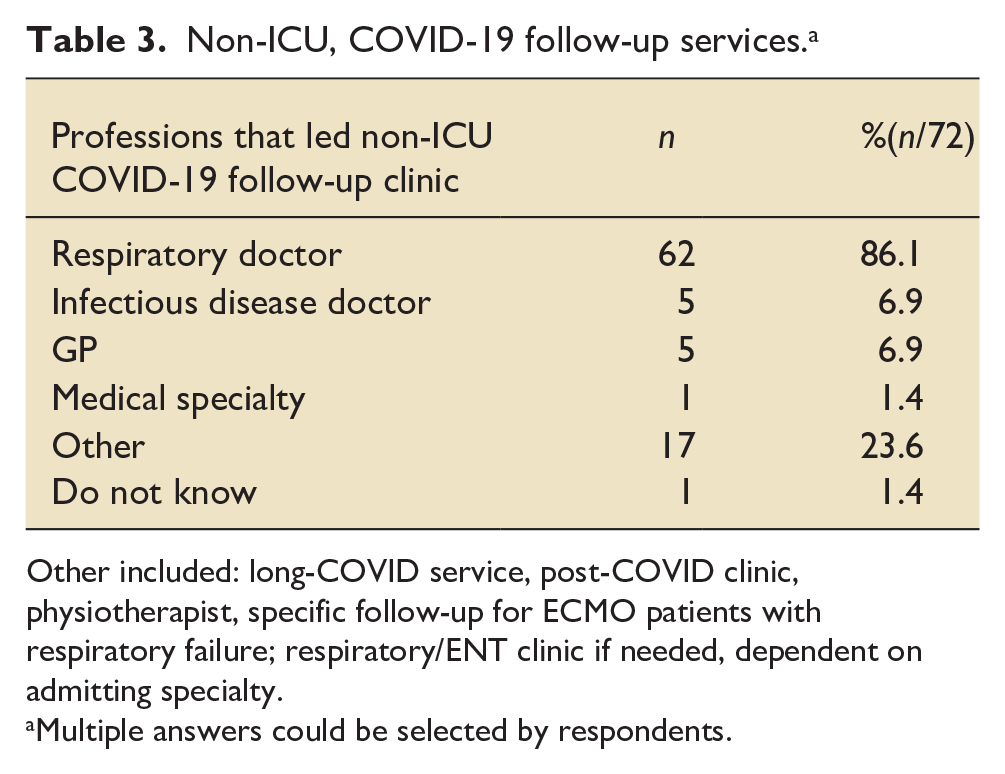
Other included: long-COVID service, post-COVID clinic, physiotherapist, specific follow-up for ECMO patients with respiratory failure; respiratory/ENT clinic if needed, dependent on admitting specialty.
Multiple answers could be selected by respondents.
Described changes to ICU follow-up services during the COVID-19 pandemic
Out of the 140 hospitals with an ICU follow-up service, 89 (63.6%) reported that changes made to their ICU follow-up service have remained in place. In 22 (15.7%) hospitals changes were not maintained and at 29 (20.7%) hospitals no change was made to their pre-existing ICU follow-up service. Optional space for free text allowed respondents to provide additional information about the changes to their ICU follow-up services. The 93 free text responses have been analysed and grouped into five main themes: funding, eligibility for follow-up, method of follow-up, staffing and bridging services (see Table 4). Hospitals reported learning and adapting their follow-up service based on feedback from the survivors of COVID-19 critical illness and their loved ones.
Described changes to ICU follow-up services during the COVID-19 pandemic.
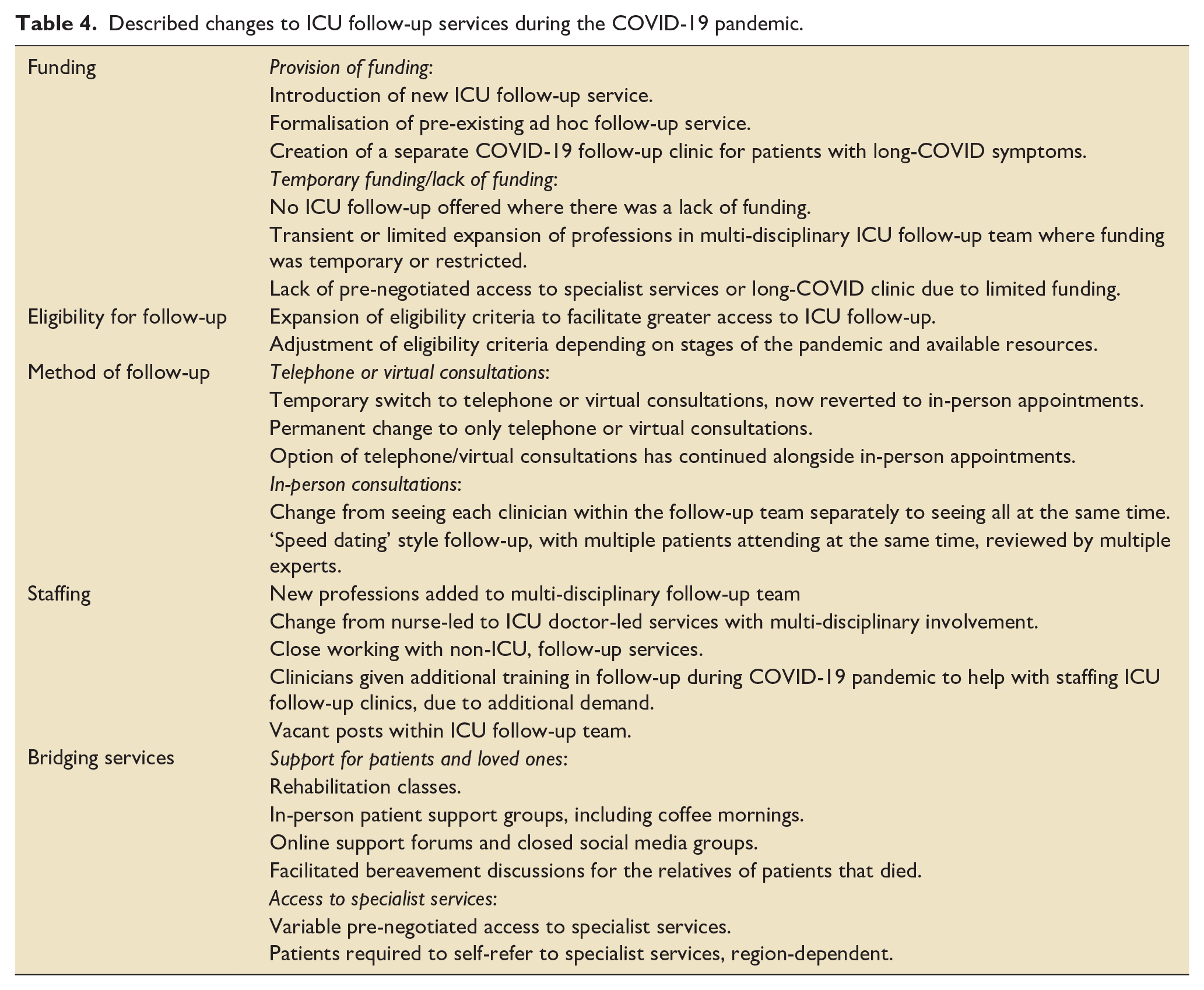
Funding
An injection of funding during the COVID-19 pandemic allowed the creation, expansion and formalisation of ICU follow-up services. However, not all hospitals received funding and at some sites it was temporary or conditional, which was reported to be a source of frustration for respondents. Whether changes made to follow-up services during the COVID-19 pandemic were maintained was dependent on continued funding.
Eligibility for follow-up
Many units expanded the eligibility criteria for invitation to their ICU follow-up clinic. Similar themes were observed in patients reviewed in non-COVID ICU follow-up, but there was a recognition that patients who received non-invasive ventilation had similar follow-up needs to those who were mechanically ventilated. Teams reported adjusting their follow-up provision at different stages of the pandemic and depending on available resources, changing the eligibility from any patient with COVID-19 critical illness, to criteria based on length of stay in ICU, or length of time receiving mechanical ventilation.
Method of follow-up
Follow-up services were adapted out of necessity during the COVID-19 pandemic, embracing the use of telephone or virtual consultation when hospital attendance restrictions were in place. Telephone-based screening tools were implemented to identify which patients would benefit from support. An improvement in attendance to follow-up appointments was observed with telephone and virtual consultations, which both increased accessibility to follow-up for patients. Despite the post-pandemic relaxation of restrictions, hospitals reported continuing a virtual/telephone-only follow-up service or offering patients the option of virtual, telephone or in-person consultations with a minority reporting a return to solely in-person consultations.
Staffing
There was an expansion of multi-disciplinary ICU follow-up teams with the addition of new professions. The addition of, and better access to, psychologists and physiotherapists were highlighted. Vacant posts within the follow-up team were mentioned, though reasons were not offered for the vacancies.
Bridging services
In-person and virtual community-based programmes were created by ICU follow-up teams, through rehabilitation classes, coffee mornings and support groups to allow patients to discuss their shared experiences in a supportive environment. One follow-up service reported that dedicated resources were used to facilitate bereavement discussions for the relatives of patients that had died and who were not allowed to visit during the COVID-19 pandemic. A mixture of experiences were reported by respondents in terms of accessing specialist services, with some reporting easier access during and since the COVID-19 pandemic and other respondents unable to access specialist services for community-based follow-up, requiring patients to either self-refer or seek referral by their GP.
Discussion
Findings from this national survey provide a comprehensive evaluation of the changes made to follow-up services for survivors of COVID-19 critical illness in the UK. The results demonstrate that there was an expansion in both the number of ICU follow-up clinics, and in the members of the MDT involved in delivering support to survivors of COVID-19 critical illness, during the COVID-19 pandemic.
Funding has consistently been reported as a barrier to delivering ICU follow-up services.7,11,12 In this survey, hospitals reported that the COVID-19 pandemic brought an injection of funding, which facilitated the introduction of ICU follow-up services, formalisation of previously ad hoc follow-up or expansion of an existing service to include additional professions within the multi-disciplinary team. There has been a consistent increase in the reported provision of ICU follow-up in the UK over the past decade, from 27.3% of hospitals in 2013 11 to 73.9% in 2021 7 and 80.5% in this study, though this peak in provision may be transient in view of the temporary funding provision reported by sites.
Psychologists were previously the most frequently cited missing member of the ICU follow-up team, present in only 17 out of 127 hospitals (13.4%) in 2021 7 compared to 42.1% in this survey. Whilst this improvement is encouraging, it still falls short of NICE quality standards and guidance from the Intensive Care Society and the Faculty of Intensive Care Medicine, which recommend the inclusion of a psychologist in the ICU follow-up team.10,22 Psychologists are invaluable members of the multi-disciplinary ICU follow-up team, able to provide tailored, evidence-based interventions for anxiety, depression and PTSD, in addition to offering support to patients with psychological and emotional needs during their rehabilitation and recovery after ICU discharge.4,8,10 The significant psychological burden on survivors of COVID-19 critical illness has been reported and emphasises the vital role psychologists have within the ICU follow-up team.2,23 –28
In comparison to patients admitted to ICU with viral pneumonia, patients with COVID-19 required advanced respiratory support for longer, which will have contributed to longer overall ICU admissions observed during the pandemic.3,29 As such, although our survey did not evaluate the volume of patients seen in ICU follow-up clinics, it is likely there was an increase in the number of eligible patients, applying NICE eligibility criteria for ICU follow-up and in particular considering the widening of eligibility that respondents described.8,9 Nationally and internationally, there is no consensus on which patients should be invited for ICU follow-up, nor the modality for follow-up that should be used at different timepoints. The wide variety of inclusion criteria in global studies that assessed the presence of PICS in survivors of COVID-19 critical illness, matches the practices reported by ICU follow-up services in this study, and reflects the lack of consensus.5,23 –27,30 –35
Pandemic restrictions forced ICU follow-up clinics to adapt. The introduction of virtual and telephone consultations facilitated the delivery of post-ICU care and were noted to improve attendance to clinic appointments. The requirement for in-person attendance has previously been described as a barrier to engagement in follow-up services.36,37 The improved engagement amongst patients belonging to ethnic minority groups, described by one hospital in this study, when a hybrid model for follow-up was applied has been discussed previously. 4 Remote consultations offer patients greater flexibility in the timings of appointments and can negate the hidden challenges of an in-person hospital appointment, whether physical, temporal or financial.4,37,38 There is also evidence that the inclusion of families can improve post-ICU care, especially if the patient was isolated during their ICU stay. 39 Equity of access to follow-up should be considered, including the provision of interpreters, translated materials and/or use of text transcription services in virtual consultations.4,37
Strengths and limitations
This study has several strengths. Firstly, respondents included multi-disciplinary team members from all devolved nations within the UK. Second, each hospital was contacted directly, after the survey was shared through cascading measures, which facilitated a high response rate, exceeding our a priori threshold. Third, use of free text answers provided the opportunity to provide additional information and allowed us to capture a nuanced snapshot of the range of changes hospitals made to their ICU follow-up service during the pandemic, and whether such changes persisted. Fourth, this survey built upon previous national surveys assessing ICU follow-up services in the UK aligning the questions used and using similar methodology to allow comparison of ICU follow-up services in the UK across the past decade.7,11
Limitations of the study are firstly that the survey was open for 6 months to reach the a priori threshold for responses. It is possible that the ICU follow-up service configurations reported by earlier respondents may have changed by the time the survey closed. Second, whilst we limited the number of questions to increase the likelihood of survey completion, some questions may have been subject to individual interpretation. In addition, free text spaces were optional and although a minority of respondents chose not to provide additional information explaining the changes made to follow-up services in their hospital, this data was not collected quantitatively. We are unable to quantify the representative nature of the qualitative data provided for hospitals across the UK, including the number of hospitals that have been impacted by funding increases or restrictions for example. Third, there is a potential risk for unreliable survey responses, which may not have been detected with our pragmatic approach of seeking a single survey response per hospital. Finally, the data provided is specific to the UK, where ICU follow-up services are established and well characterised.
Conclusion
There was an expansion in both the number of ICU follow-up clinics and the number of professions delivering post-ICU care to survivors of COVID-19 critical illness in the UK. Most of the changes to ICU follow-up services have persisted. There continues to be much variation in the provision of ICU follow-up. The lack of evidence for the timing of follow-up or the professions required within a follow-up team have made the development of national and international consensus challenging. This study has demonstrated that despite national guidance for the standard of care, ICU follow-up services are applying a more personalised approach. Future research should examine the impact of online or hybrid models on equity of access to follow-up services, patient recovery and level of patient retention compared to in-person, hospital-based interventions.
Supplemental Material
sj-docx-1-inc-10.1177_17511437251334354 – Supplemental material for Provision of follow-up services for survivors of COVID-19 critical illness: A UK national survey
Supplemental material, sj-docx-1-inc-10.1177_17511437251334354 for Provision of follow-up services for survivors of COVID-19 critical illness: A UK national survey by Jin-Xi Yuan, Constance E D Osborne, Ibrahim Almafreji, Bronwen Connolly, Andrew J Boyle, Mary Gemma Cherry, Brian W Johnston, Karen Williams, Christina Jones, Peter Fisher, Ingeborg D Welters and Alicia AC Waite in Journal of the Intensive Care Society
Footnotes
Author contributions
Conceptualisation: equal contribution from AACW and IDW, supported by BC, BJW and AJB. Data curation: equal contribution JXY and CO, supported by AACW. Formal analysis: equal contribution from JXY and CO, supported by AACW. Funding acquisition: equal contribution from AACW, MGC and IDW. Investigation: led by JXY and CO, with supporting contributions from IA and AACW. Methodology: led by AACW, supported by BC and IDW. Project administration: led by AACW, with support from KW. Supervision: AACW. Visualisation: led by JXY and CO, supported by AACW. Writing - original draft: JXY and CO. Writing - review & editing: led by JXY, CO and AACW, with equal contribution from BC, AJB and MCG, and supporting contributions from CJ, PF, BWJ, IA, KW and IDW.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported through funding from the Intensive Care Society (ICS) New Investigator Award. Additional charitable funding was provided by the Mersey School of Anaesthesia (MSA) upon application. Neither the ICS, as the primary funding source, or the MSA had a role in the design of this study or any role during its execution, analysis or in the decision to submit results.
Research ethics approval
The study was approved by the Health Research Authority (East Midlands - Derby Research and Ethics Committee, reference: 20/EM/0247).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.