
Abstract
Novel coronavirus disease (COVID-19) has resulted in huge numbers of critically ill patients. This study describes the inpatient recovery and rehabilitation needs of patients admitted with COVID-19 to the critical care unit of a 400 bedded general hospital in London, United Kingdom. The rehabilitation needs of our sample were considerable. It is recommended that the increase demand on allied health professionals capacity demonstrated is considered in future COVID-19-related workforce-planning.
Introduction
Long-term recovery patterns of patients admitted to critical care (CC) with COVID-19 are unknown, but critical illness can result in poor nutritional status, dysphagia and reduced mobility.1,2 Understanding patterns of recovery in CC COVID-19 survivors may inform future inpatient rehabilitation service provision and lessen morbidity.
Method
A non-blinded, retrospective, observational study was conducted at a general hospital in North London. All patients admitted to CC with COVID-19 between 06/03/20 and 09/05/20 and surviving to hospital discharge were included. Patients who transferred to other acute hospitals or died before hospital discharge were excluded. Two researchers extracted data from an electronic clinical database compiled by the CC therapy team. Anomalies and missing data were cross-referenced against individual patient’s medical notes for accuracy. Data retrieved included patient demographics; key CC and COVID-19 interventions; therapy input; discharge destination; anthropometry; duration of nutrition support; the use of modified consistency diets and time to achieve pre-defined mobility outcomes following cessation of mechanical ventilation. Data was summarised as means, medians and ranges or percentages using SPSS. 3
Results
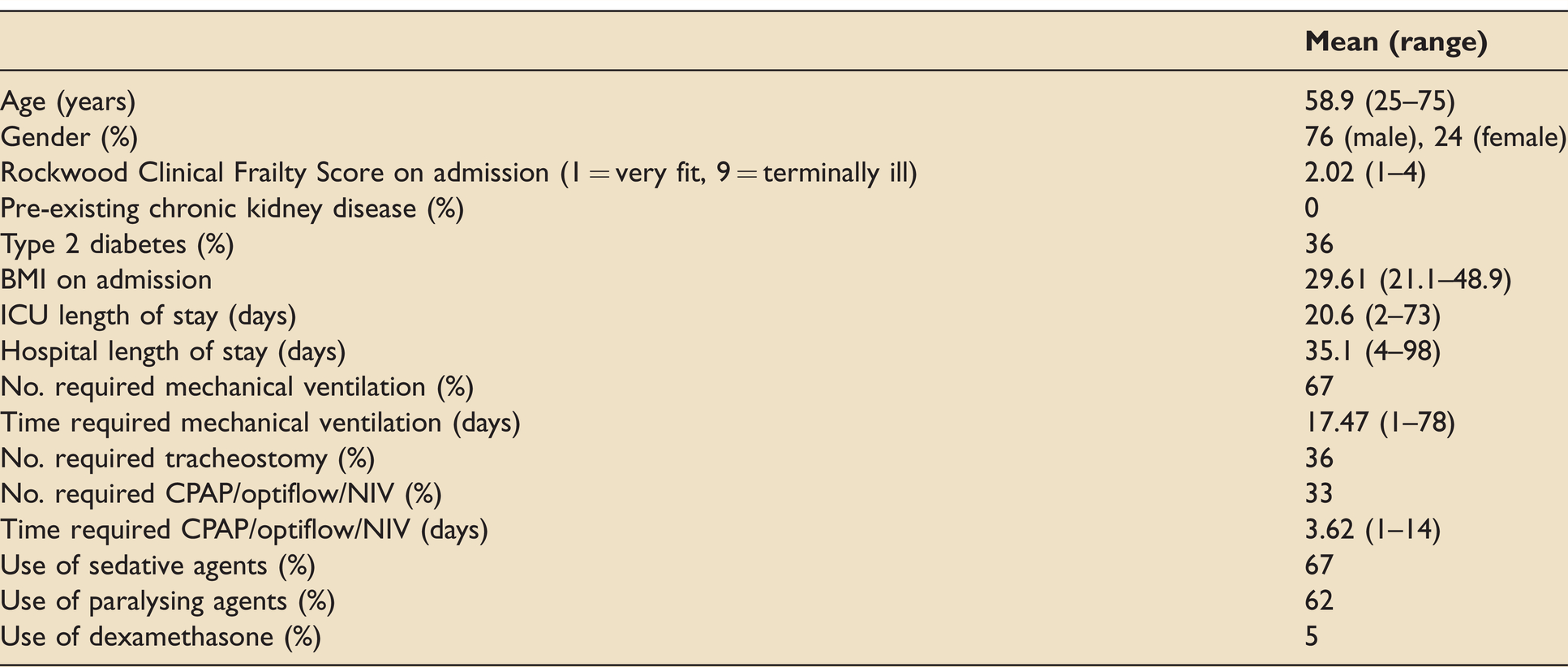
Patient demographics and CC treatments are outlined in Table 1.
Patient demographics and critical care treatments.
Therapy requirement was high with 95%, 67% and 98% patients receiving dietetics, speech and language therapy and physiotherapy input, respectively. Weight loss was high with a mean change of -11.3% (median -11.5%, range 32.5%) body weight during admission. Over half (55%) of patients needed modified diet and/or fluids on transition to oral diet. Patients took 8.9 days (median 5, range 0-85) to safely recommence oral intake post cessation of ventilation via endotracheal tube (or managing over 12 hours on a tracheostomy mask). One patient remained nil-by-mouth on discharge from hospital. Average duration of nasogastric feeding was 38.6 (median 30, range 2-74) days. Two patients received gastrostomy feeding tubes. Oral nutritional supplements were prescribed for 88% of patients however only 31% patients were able to meet their full nutritional requirements on hospital discharge.
Time from ventilation cessation to sitting unsupported, standing and mobilising 10 metres was 3.5 (median 4, range -40-24), 6.1 (median 4, range -7-31) and 12.1 (median 8, range 0-33) days respectively. Some patients were able to engage in therapy prior to cessation of ventilation. All patients were able to breathe independently, sit unsupported and stand at hospital discharge and 86% were able to mobilise over 10 metres. Patients were discharged directly home (60%) or to an inpatient rehabilitation facility (40%).
Discussion
Our patient demographics mirror national averages of those admitted to CC for age, sex, length of stay and respiratory support. 4
Timing of tracheostomy was later than recommended in the literature, 5 primarily due to avoidance of disease transmission to clinicians and high ventilatory requirements. This may have had significant impacts on recovery due to higher doses of sedative and paralytic agents and prolonged presence of an artificial airway through the larynx, pharynx and oral cavity. 6
Resumption of oral intake post ventilation appeared to be slower than reported in non-COVID-19 CC groups. 7 Requirement for modified consistency diets matches that reported in patients who require prolonged intubation, 8 which supports our theory that the delay in tracheostomy insertion may have contributed to the resulting impairment. The association between prolonged sedation and delirium 1 is also likely to have been a factor, indeed, one patient believed staff were poisoning his food and was afraid to eat and drink. Anecdotally, the prevalence of delirium appeared high. Again, this may be related to prolonged sedation as well as staff use of extra personal protective equipment, fear of a new and unknown disease and lack of visitors.
Poor nutritional intake lasted until discharge for most patients. High rates of dysphagia and delirium are possible causes, but appetite and difficulties self-feeding are also likely to have had an impact. It was noted by therapy staff that visitor restrictions appeared to exacerbate social isolation and limit access to culturally appropriate and familiar foods. The impact of families on achieving adequate nutrition intake in hospital has perhaps been greatly under recognised until now.
Overall, patients were slow to regain mobility. Therapists noted that reduced consciousness and breathlessness delayed physical progress. Interestingly, several patients’ mobility was further hindered by new peroneal nerve injuries, which have been reported elsewhere in relation to COVID-19 9 when ventilated and sedated in CC.
In conclusion, the rehabilitation needs of patients requiring CC in relation to COVID-19 are considerable and require extensive allied health professional input. It is recommended that the increased demand on allied health professionals capacity demonstrated in this study is considered in future COVID-19-related workforce-planning.
Additionally, further research is required to identify risk factors for and potential preventative measures against developing COVID-19-related CC illness. However, it is suggested that medical and therapeutic interventions should aim to minimise the prevalence and effect of delirium in order to maximise functional outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.