
Abstract
The use of high flow nasal oxygen (HFNO) in clinical practice is increasing with robust evidence of its respiratory benefits. Swallowing is known to be heavily coordinated with breathing, in addition to sharing a physical pathway in the upper airway. Applying HFNO via these spaces may also have an impact on the swallowing process. Yet, there is a lack of literature regarding the effect of HFNO on swallowing and on dysphagia. This narrative review aims to summarise the existing literature, draw conclusions on important clinical questions where possible and set the scene for future research. A database search was conducted on 24/01/2024 across CINAHL, Medline and Embase. Due to paucity of literature, studies with adult participants within and outside of ICU were included, and references cross-checked. Conference abstracts were also included. The search was repeated on 5/6/2024. Twelve articles were included in direct data comparison, in addition to studies examining the biomedical effect of HFNO that is, the impact of HFNO on the physiology of the oropharynx and swallow function. The authors conclude that whilst studies are limited in numbers and some results controversial, indications are that HFNO may demand adaptations to swallowing and some patients may not have this capability to adapt. HFNO should not be a barrier to a swallow assessment, irrespective of flow rate and the decision to assess should be based on overall patient presentation, as with any other population. Instrumental swallowing assessment is recommended to confirm any detrimental or beneficial impact of HFNO on swallow function. Robust research and guidelines are needed.
Keywords
Introduction
High-flow nasal oxygen (HFNO) therapy is an increasingly prescribed intervention for acute hypoxia, capable of delivering up to 100% humidified and heated oxygen at a flow rate of up to 60 L/min, via nasal cannulae or a tracheostomy. It has many clinical applications in the intensive care unit (ICU), including acute hypoxaemic respiratory failure, post-surgical respiratory failure, acute heart failure/pulmonary oedema, hypercapnic respiratory failure, chronic obstructive pulmonary disease (COPD) and pre- and post-extubation oxygenation. 1
When effective, HFNO results in physiological dead space washout of waste gases including carbon dioxide (CO2), decreased respiratory rate, added positive end-expiratory pressure, increased tidal and end-expiratory tidal volumes.2,3 The proven benefits have led to the development of international clinical practice guidelines.4 –6 More recently, particularly during and post pandemic, HFNO has become the preferred non-invasive respiratory support system for hypoxaemia, over conventional low flow oxygen therapy, both within and outside the ICU.7,8 Despite some reported drawbacks and potential risks in the ward environment, 9 HFNO use is becoming common.
The route and nature of HFNO delivery means that it is theoretically possible for patients to eat and drink whilst receiving HFNO therapy. However, many patients prescribed HFNO have significant and multiple risk factors for dysphagia, especially in ICU. Systematic reviews report between 3% and 68% of patients in ICU present with dysphagia.10 –16 Common reasons for dysphagia in critical illness include intubation trauma, frailty, ICU acquired weakness, cognitive impairment, multiple neurological and medical comorbidities (such as diabetes), respiratory disease and support (i.e. ventilation and tracheostomy), and reflux.15,17 –22 In addition, dysphagia often goes undetected due to the high prevalence of silent aspiration.13,15,17 Determining its presence and aetiology is more complex due to the cause and effect relationship compromising the respiratory system further.
The swallowing act is rapid and precisely coordinated with breathing and requires pinpoint synchronisation of respiration with the swallowing phases for effective airway protection. In normal swallowing, apnoea occurs during laryngeal closure for a mean duration of 1 s, 23 lasting up to 10 s in sequential drinking, with both swallow duration and apnoeic period increasing with age. The most common respiratory-swallow pattern, as observed in spirometry studies, is ‘expiration – swallow (accompanied by apnoea) – expiration’. This occurs in 83% of healthy adult swallows. 24 The expiratory glottic clearance post swallow supports expulsion of any bolus material remaining in the laryngopharynx. However, when the body is in respiratory distress, the drive to breathe is overriding, which can alter the breath-swallow pattern and increase demand on swallow function. For example, an ‘inspiration – swallow apnoea – inspiration’ pattern was shown to increase aspiration risk due to inhalation of pharyngeal residue post swallow. 24 This dynamic is illustrated in the shared physiological-psychoemotional manifestations of COPD – ‘Mind-body-breath’ which complicates respiratory anxiety, swallowing and dysphagia. 25 HFNO itself may cause a significant change to the precisely coordinated processes of breathing and swallowing in the shared pathway, which ought to then have an impact on both.
Dysphagia in ICU is known to be associated with adverse clinical outcomes, including increased aspiration risk, aspiration-induced pneumonia, delayed resumption of oral intake, malnutrition, decreased quality of life, prolonged ICU and hospital length of stay, and increased morbidity and mortality.19,26,27 Importantly, the impact of HFNO on dysphagia, and clinical outcome, whether supportive or detrimental, is not well understood. Whilst there is an abundance of literature supporting the benefits of HFNO from the respiratory standpoint, there is very little published to date on the impact of HFNO on swallowing and dysphagia. This is a clinically important topic given the increased frequency of HFNO use, and warrants exploration. A narrative review was chosen for this purpose due to insufficient literature to justify a meta-analysis, with acknowledged potential for bias. 28
Aims
This narrative review aimed to summarise the available evidence relating to HFNO, swallowing and dysphagia in ICU, to identify knowledge gaps and discuss the current implications for clinical practice. Clinical recommendations and potential future directions have been suggested as far as possible.
Five specific questions were considered in examining the literature: How does HFNO impact normal swallowing?; Does HFNO cause dysphagia or exacerbate dysphagia?; Does HFNO support and assist swallow function?; Are some patients on HFNO more at risk of dysphagia than others and if so, what patient risk factors matter?; What is the state of clinical practice?
Methods
An electronic database search was conducted on 24/1/2024 across CINAHL, Medline and Embase using terms ‘dysphagia’ OR ‘swallow*’ AND ‘high flow’ OR ‘HFNO’ OR ‘HFNC’ OR ‘NHF’. Abstracts were screened and duplicates removed. Due to paucity of literature studies with adult participants both within and outside of ICU were included, including conference abstracts and grey literature, and references cross-checked. The search was repeated on 5/6/2024.
Results
Twelve published studies29 –40 were included in direct data comparison (see Table 1 below). Additionally, 28 studies41 –69 were included in the narrative. These examined different aspects of the upper airway function, including oropharyngeal physiology, and swallow efficiency and safety, which may potentially be impacted by the presence of HFNO. The published literature has variable study design (one RCT, mostly retrospective and prospective cohort studies) and has mostly been conducted on healthy participants (n = 215). The five patient studies reported in the table have a combined cohort of 114 adult participants, however, all studies focussed on different outcomes (number of days eating and drinking on HFNO; successful commencement of eating and drinking with HFNO; diet and fluid specifics; swallow latency time during 3 ml of water; number of swallows and breathing pattern during continuous infusion of 10 ml of water).
Studies investigating HFNO and swallowing.
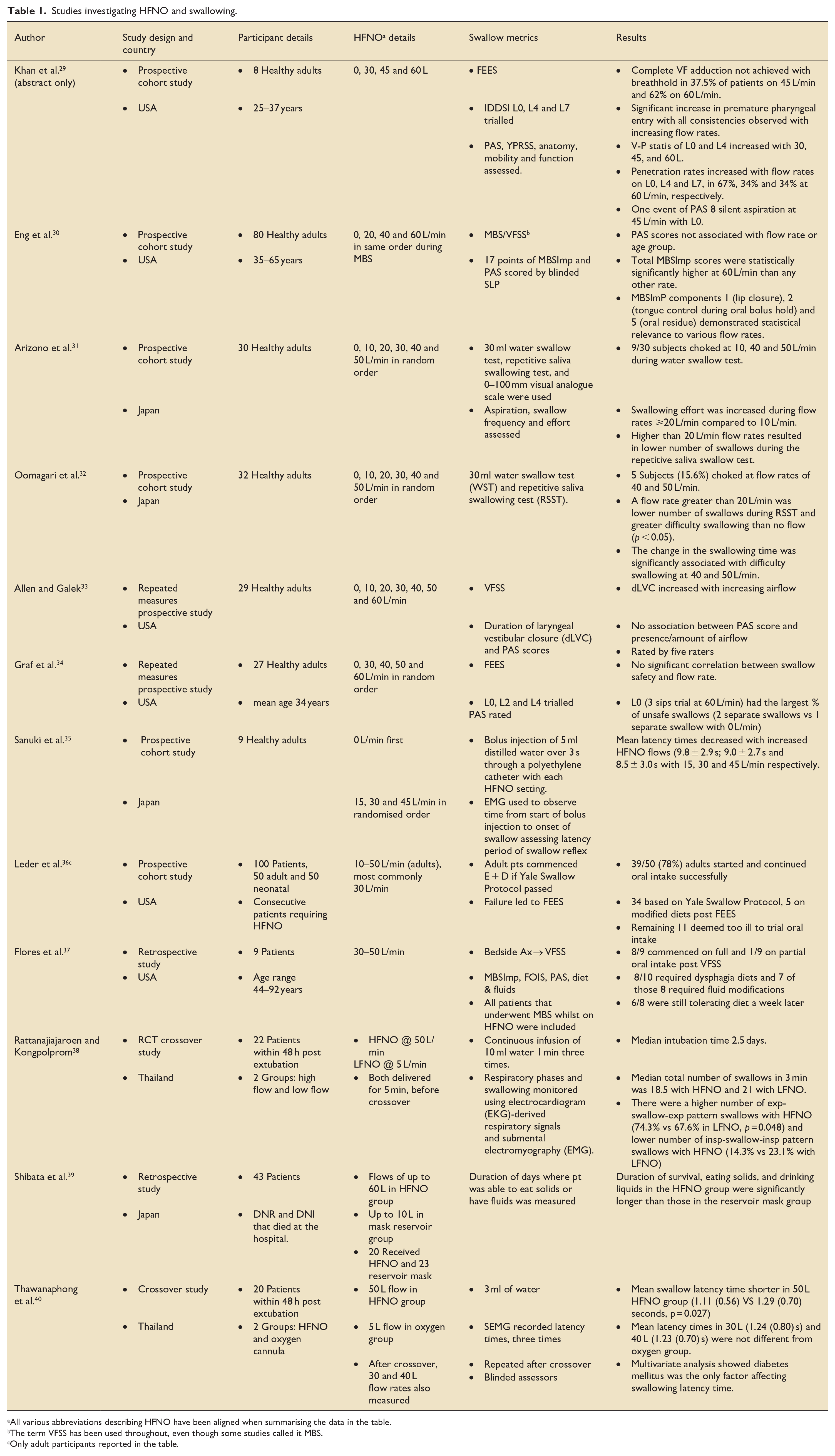
All various abbreviations describing HFNO have been aligned when summarising the data in the table.
The term VFSS has been used throughout, even though some studies called it MBS.
Only adult participants reported in the table.
How does HFNO impact normal swallowing?
During normal swallowing the vocal folds close, false vocal folds approximate and the arytenoids come together towards the inverted epiglottis to protect the airway during bolus passage through the pharynx into the oesophagus. 41 It is theoretically possible however that HFNO may ‘blow’ the glottis open and/or ‘push’ swallowed material and secretions into the airway before, during, or after the swallow. Khan et al 29 reported difficulty in achieving complete airway closure with higher flow rates (37.5% were unable to achieve closure on 45 L/min and 62% on 60 L/min) which led to increased residue and risk of penetration and silent aspiration in a small group of eight healthy adults aged 25–37. In contrast, Allen et al 33 found that HFNO did not stent the airway open during swallowing in their study with 29 healthy adults. This study postulated that healthy adults adapt the duration of laryngeal vestibular closure (dLVC) to the amount of airflow, to ensure airway protection is achieved during the swallow. Even so, higher flow rates (50 and 60 L/min) lead to a greater variability of dLVC and participants reported an increased difficulty swallowing. Variability of dLVC at higher liter per minute may be evidence for the increased effort required to maintain airway closure during the swallow.
Whilst HFNO is known to create positive airway pressure, the cmH2O per flow rate is reportedly variable and relies upon a mouth closed position. Reports include 0.5–1 cmH2O of positive airway pressure with every 10 L/min, and upto 8.7 cmH2O at 60 L/min. 42 Some patients with dysphagia and oromotor weakness will be unable to achieve mouth closure and will therefore lose some of the pressure. Oral stage dysphagia may therefore prevent them from achieving the full benefits of HFNO, and vice versa – higher flows may further prevent patients from keeping the lips closed meaning difficulties with bolus acceptance and control.
Eng et al 30 examined swallow physiology during HFNO therapy. Eighty healthy adults underwent a videofluroscopic swallow study (VFSS) with HFNO rates of 0, 20, 40 and 60 L/min. Using the MBSImP™ scoring system the authors showed significantly higher total scores (meaning reduced efficiency of the oropharyngeal structures involved) at the highest flow rate of 60 L/min compared to other flow rates. These findings, however, did not lead to an increase in Penetration Aspiration Scale (PAS) scores, likely indicating that participants were adapting and compensating for swallowing changes at these higher flow rates. Graf et al 34 also reported no significant correlation between swallow safety and flow rate in their study with 27 healthy adults. Furthermore, Thawanaphong et al 40 found that swallow latency was reduced with the highest flow rates of 50 L/min in their crossover study with 20 patients at 48 h post extubation.
In contrast, choking was reported by Arizono et al 31 in 30% of 30 healthy participants, who demonstrated choking at 10, 40 and 50 L/min flow rates when undertaking the 30 ml water swallow test. In addition, the frequency of saliva swallowing was reduced. This increased aspiration risk, with the reduction in swallow function most marked above 40 L/min flow rate. Similar findings were also reported in an earlier study by Oomagari et al 32 where 15.6% of 32 participants choked at flow rates of 40 and 50 L/min.
Further studies43 –46 show that reduced integrity of the laryngeal cough reflex, pulmonary compromise and an inability to cough against the positive pressure created by HFNO, may contribute to silent aspiration. This is not reliably detected by swallow screening but can be indicated by skilled swallow assessment, and accurately assessed by FEES or VFSS.
Laryngopharyngeal afferent sensory function is also fundamental to a safe and efficient swallow yet is often deficient in patients in critical care. Afferent sensory input via the trigeminal, glossopharyngeal and vagus nerves is required to trigger the complex pharyngeal swallow reflex. Sensory input may be tactile (pressure), chemical or thermal. 47 A high prevalence of laryngeal sensory deficits is reported in mechanically ventilated patients post-extubation and is significantly associated with secretions, aspiration, and need for modified diet recommendations, even following short intubation period. 48 Absence of the laryngeal adductor reflex, a common indicator or impaired sensation, is associated with laryngeal penetration, aspiration and pneumonia development49,50 Whilst there is a lack of research on the direct impact of HFNO on laryngopharyngeal sensation, Arizono et al 31 did report the sensory metric of reduced swallow frequency and ‘urge to swallow’ in 30 healthy adults over 20 L/min flow rate. In contrast, Sanuki 35 and Thawanaphong 40 with colleagues reported reduced latency of swallow onset with higher flows, in 9 healthy participants and 20 post-extubation patients, respectively.
The question remains whether patients in respiratory distress requiring HFNO, can make the necessary swallow adaptations and demands required in the same way as healthy adults. Overall, the effect of escalating and de-escalating respiratory support on swallowing is currently not known and needs research.
Does HFNO cause or exacerbate dysphagia?
The research is currently inconclusive. Limited data indicate that even healthy participants are at risk of aspiration with higher flow rates of nasal oxygen. However, studies have found that swallow adaptations happen in healthy 29 and patient population 40 on higher flows. A small study with eight healthy participants by Khan et al 29 suggests that dysphagia symptoms (such as pharyngeal residue, which creates an aspiration threat) occur during HFNO use in healthy adults. 29 There are no published studies on patients with a known dysphagia to establish whether HFNO may exacerbate existing dysphagia.
Does HFNO support and assist swallow function?
In a patient that has been orally intubated, the upper airway is likely to be affected by lack of airflow passage over time. In addition to laryngeal injury 12 and disuse muscle atrophy, the mucous membranes and cell rheology are likely to be altered. The impact of assisted breathing on the nasal air-conditioning function has not been fully investigated but it is known that changing the humidity and temperature of inhaled gas affects the mucosal surface mass and heat transfer. 51 Rouadi at al 52 reported that by increasing the flow of cold dry air both the water content and temperature of inspired gas decreased. No such changes were seen with hot humidified gas delivery in the nasopharynx. Contrary to standard oxygen therapy, HFNO provides heated heavily humidified gas to the upper airway, a location where the healthy mucosa is well hydrated and moist. Although, to the authors’ knowledge this has not yet been investigated, setting up a physiologically more normal environment in the laryngopharynx through HFNO may be key to a safer swallow. This concept may be especially relevant to patients with severe oropharyngeal dysphagia where secretion management is impaired, and nil by mouth and poor oral hygiene status are confounding factors.
There are a few studies that indicate a supportive role for HFNO and swallowing in patients. Rattanajiajaroen and Kongpolprom 38 conducted a crossover RCT (HFNO and low flow nasal oxygen, LFNO) of 22 patients within 48 h of extubation. In the patients on HFNO an expiratory-swallow pattern was more common (74% HFNO vs 68% LFNO) than an inspiratory-swallow pattern (24% HFNO vs 23% LFNO). Since an inspiratory-swallow pattern is more likely to lead to inhalation and aspiration post swallow, this study indicated that HFNO might reduce aspiration risk compared to LFNO. Allen et al 33 reported that the presence of HFNO could make swallowing safer by maintaining a longer duration of laryngeal closure, thereby sustaining airway protection for longer in their study with 29 healthy adults. Extrapolating from this finding, there is a possibility that the increased dLVC with some flows could act as a dysphagia compensatory or rehabilitation exercise to improve airway protection in some patients. Thawanaphong et al 40 and Sanuki et al 35 also concluded from their studies on 20 post-extubation patients and 9 healthy volunteers, respectively, that higher HFNO flow rates may enhance swallow function, by observing reduced latency of the swallow reflex with increasing flow rates. Latency or a delayed swallow can lead to pre-swallow aspiration or bolus stasis related aspiration, so improving timing of swallow initiation is a potentially beneficial compensation on higher flows.
If HFNO reduces overall respiratory effort and work of breathing hence the burden on breath-swallow synchronisation is likely lifted. Patients tend to inhale post swallow when the swallow-apnoeic period is poorly tolerated, such as in COPD, 25 increasing their aspiration risk. It is therefore possible that HFNO can support breath-swallow synchronisation and swallow-apnoea endurance in some patients. This deserves more investigation, since if HFNO can reduce dysphagia in certain patient groups, this would assist clinicians to effectively target those at risk of dysphagia and aspiration for a swallow assessment and facilitate earlier safe oral intake in others.
Are some patients on HFNO more at risk of dysphagia than others and if so, what patient risk factors matter?
The published literature on HFNO is currently insufficient to fully answer this question. However, it is well understood in the ICU-related dysphagia literature that there are specific medical markers which increase the risk of dysphagia for patients. Intubation is a significant factor; specifically, duration, reintubation, emergent intubation, difficulty of intubation and size of the endotracheal tube, which all contribute to laryngeal structural injury and desensitisation.12,15 –17,19 –22 Structural and sensory impairments interfere with both swallow safety and efficiency. For example, laryngeal oedema is often associated with intubation and laryngopharyngeal reflux, can reduce airway patency, airflow and subsequently laryngeal closure and sensory response to aspiration.22,53 Vocal fold immobility/palsy is both common following intubation and is associated with significant risks of aspiration.53,54
Medical and surgical issues commonly seen in ICU that also affect swallowing include ARDS, sepsis, diabetes, hypertension, COPD, ICU polyneuropathy/myopathy, reflux, frailty, cardiac disease, Covid-19, cardiothoracic surgery and peri-operative stroke.10,11,18,56 –62 A systematic review and meta-analysis by Hou et al 63 also determined age, APACHE II score, intubation duration and tracheostomy as significant risk factors for dysphagia. Other diseases known to commonly cause dysphagia include neurological conditions, head & neck cancer, burns facial/inhalation injury.64 –66 Many patients on HFNO will present with these medical conditions and patient factors, in addition to delirium or cognitive impairment, which carry dysphagia risks. Clinicians managing patients on HFNO should be aware of the other risk factors and take an individualised patient approach.
Patient’s dysphagia characteristics are useful to consider when thinking about the potential impact HFNO may have on dysphagia severity; some symptoms may improve with presence of HFNO, and some may worsen. Clinical bedside indicators of dysphagia, such as weak or wet voice, weak cough, excess upper airway secretions, coughing or aspiration signs on oral intake, should be monitored closely and patients referred to SLT early when any concerns arise.
The question remains whether patients can achieve the swallow adaptations reported in the research carried out on healthy participants. If a patient has breath-swallow pattern incoordination, due to an underlying respiratory disease such as COPD,25,67 then HFNO may assist swallow by propping up respiration and normalising the breath-swallow pattern. But if there are significant dysphagia symptoms, due to critical illness, comorbidities or other causes, then supporting respiratory function with HFNO is unlikely to be sufficient to achieve safe swallowing. Therefore, appraising the clinical picture and medical trajectory are more important than making oral feeding decisions based on presence and amount of high flow alone.
What is the state of clinical practice?
Currently there are no national clinical guidelines for evaluating swallow function in adults in the presence of HFNO. However, a retrospective analysis carried out by Flores et al 37 in the USA found that decisions regarding safety of oral intake should be based on the overall clinical picture, cognitive status, physical status and instrumental evaluation of swallowing (VFSS). A study of clinical practice in Australia amongst SLTs showed a lack of knowledge of the current research as to the impact of HFNO on swallowing, and wide variability in decisions around swallow assessment (4% did not assess, 25% offered assessment, 71% assessed based on patient factors). 68 With increasing flow rates more clinicians chose not to assess (68% on 50 L/min) and less than a third assessed regardless of flow rate. There is a real need to increase clinicians’ knowledge of HFNO, improve confidence to proceed with swallowing assessment and to base recommendations on the holistic picture not purely on flow rates.
Discussion
Knowledge on HFNO and its impact on swallowing/dysphagia is limited to a low level of available evidence. Overall, there are a small number of single-centre based studies published investigating small cohorts of mostly healthy populations, using variable methodologies with contrasting results. This makes it challenging to apply evidence-based decisions in the ICU HFNO cohort.
The aetiology of dysphagia in individual ICU patients is often multifactorial and complex and can be acute, acute on chronic, transient or persistent. Dysphagia can be motor, sensory or both, but the degree of either is difficult to measure. The addition of HFNO via the upper airway, can make analysing dysphagia symptoms more difficult. The need for accurate instrumental swallow assessment for the HFNO population is therefore vital. Both VFSS and FEES are suitable tools to investigate the potential impact of HFNO on swallowing. VFSS may be preferred to visualise and quantify laryngeal closure during the swallow as in Allen et al 33 study, but rarely feasible for patients in ICU. FEES is highly suitable for ICU patients, when laryngeal injury is suspected, in cases of severe dysphagia and secretion management issues and contributes to feeding and weaning decisions.
The impact of nasendoscopy, on HFNO flow and pressure has not been directly studied, although it is known that pressure mainly depends on flow rate and nares occlusion, 69 with the gas following the path of least resistance. FEES has been shown to be safe and effective in the presence of HFNO in healthy adults. 28 It is likely that the presence of the nasendoscope (in addition to a nasogastric tube and any upper airway oedema) reduces the flow rate and pressure towards the airways, but the extent will be patient specific. The need for, safety and efficacy of increasing flow rates to compensate for the nasendoscope presence and facilitate a FEES is unknown. Although both authors use FEES routinely in the presence of HFNO, there are currently no published studies involving patients where FEES has been used to diagnose and quantify dysphagia in this population.
Whether HFNO could cause or exacerbate dysphagia was not able to be determined based on the available evidence. In our clinical observations, if a patient already has dysphagia (i.e. post-extubation and on HFNO in ICU), then HFNO may exacerbate some of their dysphagia symptoms. For example, someone with poor oral control of the bolus and reduced pharyngeal sensation; both common post extubation, 14 can have increased anterior spill from the mouth, posterior spillage pre-swallow and penetration of residue into the pharynx and airway post swallow, due to high gas flow in the shared pathway. The authors recommend that determining certainty regarding whether the impact on airway protection is detrimental or supportive, requires visualisation and measurement during FEES or VFSS. Prevention of further respiratory infection and compromise due to swallow dysfunction and aspiration is clearly key to successful weaning off HFNO and patient recovery.
Current clinical challenges
Staff awareness and understanding of HFNO, and its potential impact on swallowing as known to date needs improvement. SLTs face several professional challenges including lack of clarity and subsequently confidence around assessing these patients. This can lead to an overcautious approach to oral feeding and a prolonged Nil By Mouth status, which is detrimental to patients and should be avoided. Instead, SLTs should support MDT staff to recognise who is more at risk and who to refer to SLT for assessment, enabling safe and appropriate oral feeding decisions. Despite the lack of research there is still an MDT training need to support management of the HFNO in this sick cohort of patients in ICU. Training should incorporate information on dysphagia red flags and clinical signs of dysphagia and indicators for referral. Instrumental assessment is much needed and would expedite decisions but is currently under resourced and underutilised. We can extrapolate from the data that in the absence of any clinical guidance in the UK, SLTs and the MDT are often unsure how and when to proceed with oral feeding in the presence of HFNO.
Limitations
The nature of a narrative review significantly increases author bias, and the less systematic approach mean that not all of the available evidence may have been addressed.
Conclusions
The existing research on HFNO, swallowing and dysphagia is somewhat limited and conflicting which leads to an unclear understanding of the potential risk for dysphagia in this ICU cohort. Whilst clinicians are often concerned about feeding patients on HFNO, there is a lack of knowledge on how best to manage eating and drinking safely. Based on the available data, it is evident that HFNO should not be seen as a barrier to swallow assessment, irrespective of flow rate. The decision to assess should be based on the overall patient presentation, as with any population.
In the authors’ opinion, the most important considerations which influence the patients’ ability to make swallow adaptations on HFNO in the ICU, are health status, medical condition, dysphagia risk factors, frailty and whether the medical and respiratory trajectory is escalating or improving. A deteriorating picture with worsening respiratory compromise would constitute red flags for dysphagia with or without HFNO. It is strongly suggested that instrumental swallowing assessment be used with this population. Robust studies considering different flow rates, patients with dysphagia risk factors, respiratory trajectory and patient experience of eating and drinking on HFNO are needed to assist clinicians with decision making and inform clinical guidelines.
Future directions – What are we going to do about it?
A few recommendations are suggested by the authors:
There is a need to develop a research priority strategy promoting studies on different ICU populations on HFNO. A consistent approach to dysphagia assessment and outcome measures requires a consensus project with critical care dysphagia experts to identify the optimal approaches. A Delphi methodology or similar would support a strong foundation for building a robust evidence base. The heterogeneity of patients requiring HFNO creates both challenges and opportunities drawing on the body of established dysphagia research.
The research should aim to clarify variability in dysphagia risks in the presence of comorbidities and known red flags, to investigate the potential impact of different flow rates on swallowing in patients with critical illness, which patient groups are able to make swallow adaptations in response to HFNO and under which conditions does HFNO improve swallowing and dysphagia.
Producing preliminary clinical guidelines on dysphagia and HFNO for adults is a priority for SLTs working with this population.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.