
Abstract
Introduction
Post-extubation dysphagia (PED) can have serious consequences for critically unwell patients. COVID-19 has resulted in an increasing need for a PED screen in order to effectively identify patients and mitigate risk, whilst balancing under-resourced services. Online training provides the advantage of reducing time pressures on staff and supporting social distancing. This project aimed to adapt the Leeds Post-Extubation Dysphagia Screen (L-PEDS) and the associated training package to be more suitable and effective for use during COVID-19 pandemic.
Methods
The screen was modified to a digital format with additional guidance for users. The training package was shortened and converted to an online package while keeping the interactive mode of training.
Results
Preliminary results of 14 staff members indicate that the median confidence levels for screening patients for PED improved from 5 to 8 (on a scale of 0 to 10) after completing the L-PEDS-COVID training package. Likewise, knowledge of PED improved from a median of 4 to 8 (on a scale of 0 to 10). Training quality was rated at a median of 8 on a scale of 0 to 10 (0 being very poor; 10 being very good).
Conclusions
Preliminary evidence demonstrated increased knowledge of PED and confidence in screening. The development of an adapted version of the L-PEDS and online training package may allow easier implementation of post-extubation dysphagia screening. This could help to compensate for insufficient speech and language therapy critical care staffing, assist in identifying patients at risk and improve outcomes by enabling earlier and safe resumption of oral intake.
Introduction
Post-extubation dysphagia (PED) is a common sequelae of endotracheal intubation. More than half of patients intubated for more than 48 hours will present with PED 1 and incidence increases with duration of intubation. 2 Silent aspiration in this cohort is common,3,4 and the consequences of undetected dysphagia can have serious implications for patient outcomes and healthcare resources. The development of a PED screen was vitally important to detect and prevent aspiration in this patient cohort. A quality-improvement exercise was undertaken to develop and introduce such a screen, the Leeds Post-Extubation Dysphagia Screen (L-PEDS). 5 Piloting and evaluation of this screen on a general critical care unit at Leeds Teaching Hospitals NHS Trust had already commenced when the COVID-19 pandemic arrived.
The pandemic has resulted in an increase in critically unwell patients. This has exacerbated the impact of pre-existing inadequate speech and language therapy (SLT) staffing resource in critical care units across the UK. 6 Combined with shortages of personal protective equipment (PPE)7,8 and a need to reduce movement of staff between COVID wards and non-COVID wards to limit transmission, the pandemic has highlighted the importance of a PED screen that can be delivered by other members of the critical care multi-disciplinary team. An effective PED screen would facilitate earlier return to oral intake and ensure that only patients who are ready for SLT assessment and intervention are referred.
Furthermore, COVID-19 is resulting in a higher incidence of laryngeal oedema post-extubation 9 and can cause damage to the neural network involved in the control of swallowing. 10 These factors are likely resulting in a higher risk of PED in this patient group. Various guidelines have been published during COVID-19 regarding dysphagia management, which include recommending the use of screening.11–13 Widespread adoption of a PED screen would improve identification of patients at risk of aspiration and minimise further complications.
The first version of L-PEDS was paper-based. The training consisted of a 2.5 hour face-to-face training session delivered by an SLT. In the COVID-era of social distancing, stringent infection control processes, and severe resource constraints, revision of the screen and training package were essential. The aim of this project was to modify the L-PEDS screen and training package to be more accessible for staff and easier to implement.
Methods
This project was carried out in three phases.
Phase 1: Revision of L-PEDS
The screen was renamed L-PEDS-COVID to distinguish it from the original screen and training package. However, the screen is designed to be used with all post-extubated patients. The screen was re-formatted into an editable portable document format (PDF).
Phase 2: Revision of the training package
The primary change in the training package was to convert it to an online package using Gomo Learning 2020 software. This was vital to: (a) enable widespread training of staff with a severely compromised SLT staffing resource, (b) maintain appropriate social distancing, and (c) limit the impact on patient care from training multiple staff simultaneously. We also reduced the length of the training package from 2.5 hours to 40 minutes, in order to minimise staff time away from direct patient care and to maximise the number of staff trained.
Phase 3: Piloting of the online training package
The online training package was trialled with a group of critical care nurses at Leeds Teaching Hospitals NHS Trust. Staff were requested to complete a pre-training evaluation, a post-training evaluation and a feedback form.
Results
Phase 1: Revision of L-PEDS
The editable PDF version could be completed online and was uploaded onto hospital systems (Supplementary Material 1). This was to reduce the infection control risk inherent with paper documentation. A guidance section was included to aid staff completing the form and reduce the need for SLT support post-training completion.
Phase 2: Revision of the training package
The shorter training package resulted in significant changes to content (Figure 1). The training in normal swallowing and general dysphagia was shortened to include the most important information only, and the theoretical section focussed purely on PED. The practical session of trialling the screen with other trainees was no longer possible, and the five video practice attempts were reduced to one.
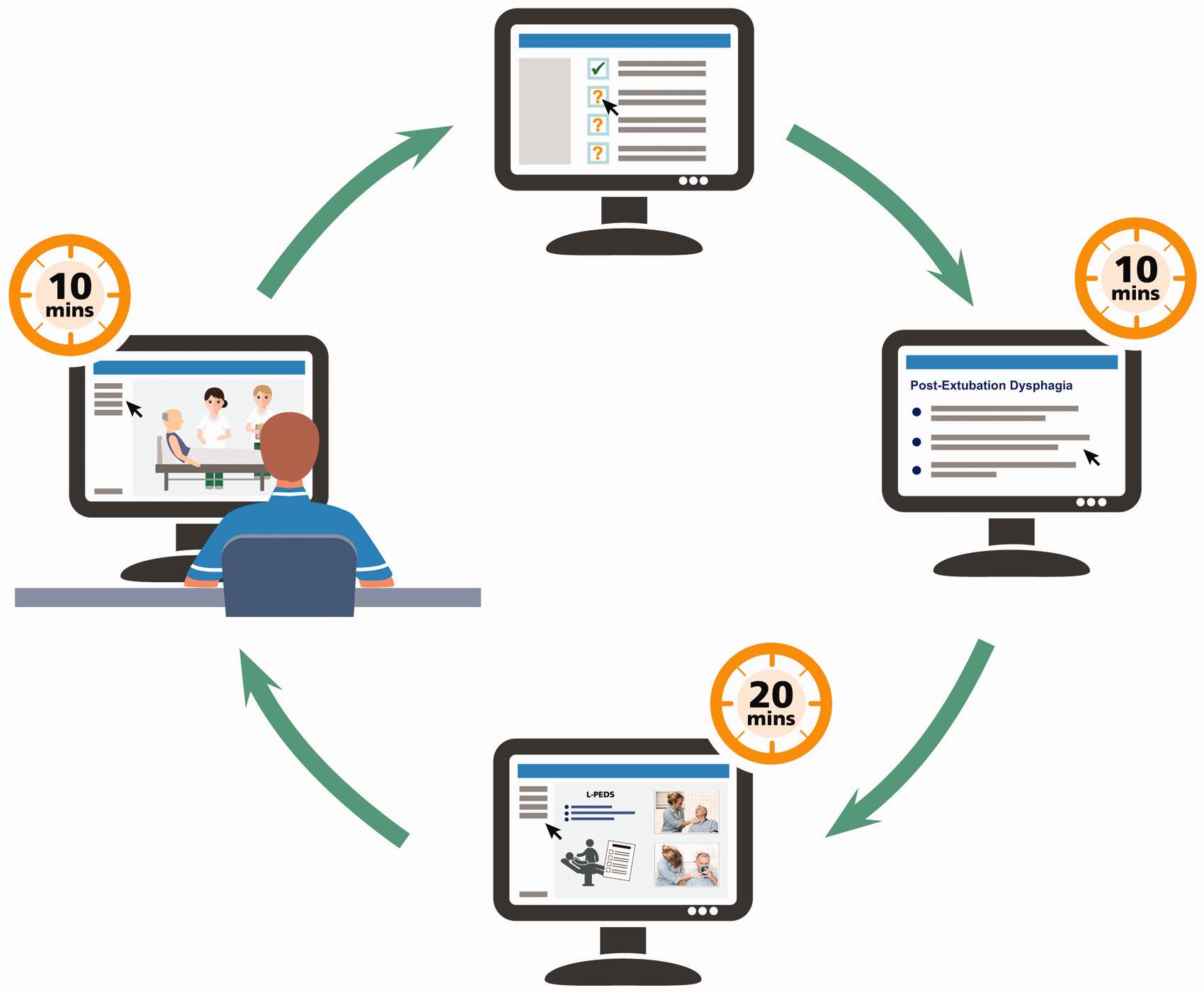
Composition of the 40 min L-PEDS-COVID online training.
Our previous face-to-face training incorporated a pre- and post-training quiz using the online presentation software, Mentimeter®. In our online training the pre- and post-training quizzes were modified and embedded into the training using Google Forms®. We also included a feedback form. There were two question sections within the training, the first included questions verifying the trainee’s understanding of how to use the screen, and the second asked patients to complete the screen for a practice video. Staff were required to achieve at least 80% in each section before the training could be completed. The requirement for staff to complete a minimum of one SLT-observed screen with a patient was removed due to staffing and PPE constraints.
Phase 3: Piloting of the online training package
Fourteen nursing staff completed the pre-training evaluation, 10 completed the post-training evaluation and 10 submitted the feedback form.
Eighty-six percent (n = 12/14) had never used a swallowing screen before. The median confidence level for trying a patient with something to eat or drink for the first time was 5 (range 1–10) on a scale of 0 to 10 (0 being very unconfident; 10 being very confident). This increased to a median of 8 (range 0-9) post-training. Having completed the training 90% (n = 9/10) reported that they felt that their pre-training reported confidence levels were accurate, with one respondent stating their pre-training confidence level was rated too low. The median knowledge of post-extubation dysphagia was 4 (range 0-10) on a scale of 0 to 10 (0 being very poor; 10 being very good). This increased to a median of 8 (range 1-10) post-training.
The quality of the training was rated as a median of 8 (range 5-10) on a scale of 0 (very poor) to 10 (very good). Staff were extremely likely to recommend this training to other friends or colleagues, with a median of 9.5 (range 6-10) on a scale of 0 (extremely unlikely) to 10 (extremely likely). Sixty percent of staff (n = 6/10) stated that the training was just the right length, 30% (n = 3/10) stated it was too short, and 10% (n = 1/10) thought it was too long. Staff provided positive feedback regarding the depth of the course, the clear explanations and visual materials used. Suggestions were made to increase the duration and content of the course, as well as incorporating additional visual illustrations.
Although 10 staff completed the post-training evaluation form and the feedback form, the training software indicated that only three of these staff had completed the training and were signed off as competent.
Discussion
There has been considerable demand for a PED screening tool during the COVID-19 pandemic. However, currently there is no widely accepted PED screen available in the UK, or internationally.14,15 A recent UK survey of critical care SLT staff 6 revealed that 72% of services (n = 46) do not use a post-extubation screen (unpublished data). Of the 18 respondents who stated that they were using a screen, most were using locally devised screens and no two respondents were using the same screen.
Preliminary results from the 14 staff that started to complete the training package indicate that the training package is acceptable to staff. Staff reported the training was of good to very good quality and were extremely likely to recommend to other colleagues. Furthermore, the confidence levels for screening and knowledge of PED improved post-training. These improvements in confidence and knowledge are comparable with the findings from our face-to-face training, where confidence improved from a median of 7 to 9 and knowledge from 5 to 8.5 The four staff who completed the pre-evaluation training, but did not complete the post-evaluation training might be explained by the training being available to all hospital staff without restriction. Some staff completing the training were not from critical care, and were redeployed staff e.g. from theatres. However, it is likely that some staff were exploring the training, before deciding that it was not appropriate for them.
Our results have highlighted an issue with the training software. There is a large difference between the numbers of staff having completed the post-training evaluation and feedback form and the numbers of staff identified by the software as having completed the training. There are various possible explanations for this disparity: 1) staff may have inadvertently not pressed the “Exit” button at the end of the training which registers completion 2) staff may have skipped parts of the training via the menu page. It will be vital to resolve this issue so that we can be assured that staff have fully completed the training and are competent to use the screen with patients.
This revised PED screen, L-PEDS-COVID, is an easy to use digital form which will be straightforward to implement in critical care units. The online training package is more accessible to staff than the previous L-PEDS face-to-face training package and reduces pressure on under-resourced SLT staff to provide training. The training will also allow more staff to be trained whilst maintaining social distancing and limiting viral transmission risk. Although this project focused on training of nursing staff, this screen has the potential to be used by any member of the critical care multi-disciplinary team who have undergone the training package.
Limitations
As yet, we have limited data on the effectiveness of the training and issues with the training software have been detected. The e-learning software used did not have the capability to provide information regarding the reason for the disparity between staff registered as having completed the training versus staff who had completed the post-training evaluation. It is important that future versions of the training prevent staff from skipping through the training to ensure that all sections are completed. Reducing the length of the training and the opportunities for staff to practice using the screen with each other, and using example videos, may result in lower levels of knowledge of PED and confidence in screening patients. Furthermore, the lack of opportunity to conduct an SLT-observed screen with a patient may also result in reduced confidence in screening and incorrect use of the screening tool.
Conclusion
The development of the Leeds Post-Extubation Dysphagia Screen for COVID with online training package will allow easier implementation of a user-friendly, evidence based PED screen. Modification of the online training package is required to ensure appropriate use and robust data collection. Further research is needed to evaluate the effectiveness of the updated online training package, the effectiveness of the screen in improving patient outcomes and a validation study is needed to quantify the sensitivity and specificity of L-PEDS-COVID. In the future, widespread adoption of L-PEDS-COVID could facilitate improved quality of life and better outcomes for patients by enabling earlier and safe resumption of oral intake.
Supplemental Material
sj-pdf-1-inc-10.1177_1751143721998140 - Supplemental material for The adaptation of the Leeds Post-Extubation Dysphagia Screen: Lessons learned during the COVID-19 pandemic
Supplemental material, sj-pdf-1-inc-10.1177_1751143721998140 for The adaptation of the Leeds Post-Extubation Dysphagia Screen: Lessons learned during the COVID-19 pandemic by Claire S Mills, Emilia Michou, Andrea Hanratty, Abby Gibson and Mark C Bellamy in Journal of the Intensive Care Society
Footnotes
Acknowledgements
We are grateful to the Intensive Care Foundation Nurse and AHP Foundation Fellowship for funding the initial development of the Leeds Post-Extubation Dysphagia Screen (L-PEDS). The authors thank Lucia Hudson-Evans, Kerry Hunter and Helen Timmins for their input into the development of L-PEDS. The authors also thank the Royal College of Speech and Language Therapy Tracheostomy Clinical Excellence Network committee for the use of unpublished survey data. We are grateful to Charben Alilio and Jennifer West from Organisational Learning for their support in creating the online learning package. We also thank Lucia Hudson-Evans, Kerry Hunter, Sarah Moss, Lydia Rawnsley, Chris Wiseman, Louise Shelley and Emma Taylor for their feedback on the online training package.
Declaration of conflicts of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Intensive Care Foundation Nurse and AHP Foundation Fellowship. Claire Mills is funded by a National Institute for Health Research (NIHR) Clinical Doctoral Research Fellowship.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.