
Abstract
In 2022, the Royal Liverpool University Hospital moved premises. As part of the move, the patients from its existing Critical Care Unit (consisting of an independent Intensive Care Unit, a High Dependency Unit and a Post-Operative Critical Care Unit), had to be transferred from the old hospital to an entirely new one. Whilst relocation of an Intensive Care Unit, its critically ill patients, staff and equipment has undoubtedly happened elsewhere in the past, very little has been written about such an undertaking. On each occasion, therefore, the teams facing this task may be starting afresh without the benefit of knowing what problems others have previously encountered and how they solved them. In an attempt to highlight some of the modifiable risks, this article serves to explain some of the planning we undertook prior to our move (i.e. forward planning), and reflects on some of the lessons learnt in the process.
By failing to prepare, you are preparing to fail
Introduction
The Royal Liverpool University Hospital (RLUH) is a tertiary university teaching hospital in Liverpool, UK. Built in 1978, its 650 beds served Liverpool’s population of approximately 500,000. In 2013, to address the rapidly deteriorating infrastructure of the old hospital, work began on building a new RLUH on adjacent land. After many delays, work was eventually completed in April 2022 and a move date, on which all services would transfer from the old Royal to the new Royal, was planned for September 2022.
The Critical Care Unit in the old Royal was split between three different parts of the building – predominantly because of where the available ward space had been at the time of the conception of each of the three component units. The 18-bed Intensive Care Unit (ICU) was on the first floor; the four-bed Post-Operative Critical Care Unit (POCCU) was adjacent to the theatres on the 11th floor; and the 14-bed High Dependency Unit (HDU) was on the eighth floor. In contrast, the new Royal has 40 critical care beds within one amalgamated unit (subdivided into four pods of 10), and this is situated near the Emergency Department, Operating Theatres and Radiology Department.
Opening the new unit thus mandated transferring up to 36 critically ill patients from the old unit to the new, and this required careful planning both to enable the continuity of care delivered to our patients and to support the staff. 1 The risks associated with the intra-hospital transfer of a single critically ill patient are well described and the incidence of serious adverse events occurring during a transfer range from 4% to 9%.2 –5 Amplify the potential risks involved with moving one patient to the simultaneous transfer of 36 patients with all their equipment, and to a new unit, and the unique challenge of relocating a ICU en masse becomes clear. Relocation of a whole ICU has undoubtedly been done elsewhere: however, given the complexities and associated risks, very little has been written about such undertakings. On each occasion, therefore, the teams facing this task may be starting afresh without the benefit of knowing what problems others have previously encountered and how they solved them.
Knowing that several new hospitals are planned in the United Kingdom,6,7 and in an attempt to highlight some of the modifiable risks, this article explains some of the planning we undertook before our move (i.e. forward planning), and reflects on some of the lessons learnt in the process. We hope this shared learning will help others avoid having to completely reinvent the ‘moving’ wheel.
Forward planning – Considerations and preparations prior to Move Day
Planning for the critical care move started in January 2021. In addition to preparing for the physical move of our patients, we were also aware that the Trust was planning major service reconfigurations following the merger of two Trusts (The Royal Liverpool & Broadgreen University Hospitals (RLBUHT) and Aintree University Hospital (AUH)). Consequently, several surgical specialities were amalgamating their workforces to operate on one site: for example, liver surgery was moving to RLBUHT whilst vascular surgery was moving to AUH, and so we were aware that we would also have to plan for this and upskill our staff to deal with a new patient cohort.
To prepare for the move, a number of issues required consideration and careful planning prior to Move Day.
Leadership roles
Given the complexity of the move, and to avoid repetition/redundancy of task allocation, it was obvious that a clear command structure was needed to plan and manage the move. A senior consultant with leadership experience was appointed to the role of Lead Critical Care Move Consultant and assumed overall responsibility for move-related planning. This person worked closely with a multidisciplinary working group representing all staff members within critical care, and communicated directly with both the Trust and Hospital Leadership Team (THLT), and with colleagues in other departments. Key points of contact included the Medical Director, Critical Care & Theatres Head of Operations, Senior Estates Manager, Move Programme Manager and Move Lead for Nursing. Meetings, with dedicated administrative support to help take and distribute minutes and prepare reports on move readiness for Trust oversight, were initially held at monthly intervals but became more frequent as the move date approached.
Learning from others
Whilst none of our team had been directly involved with the relocation of an ICU from one hospital to another, we knew that others had and would thus have invaluable knowledge, including what may or may not have worked. A colleague from Liverpool Children’s Hospital, who had been involved in the transfer of paediatric patients to their new unit, attended our planning meetings from the early stages and shared valuable insights. One example was the suggestion to designate a Gold Command Consultant on Move Day – someone whose sole job was to oversee, coordinate, and give the final go-ahead on each patient’s transfer between units. It was stressed that this person must have no other duties or distractions on the day. Without anyone in this role, confusion had previously occurred as a number of people would simultaneously sanction transfers with no oversight of what else was happening, resulting in several patients arriving at the same time, which risked overwhelming the new unit.
When is the right time to move the critical care unit in relation to the hospital as a whole?
The THLT set a 3-week period (i.e. 28th September to 20th October, 2022) for moving all the services. Given the acuity of our patients, we were asked by the THLT when we thought the Critical Care Unit should move in relation to other services within the Trust, and over how many days. We knew that in order to function as a unit in either location, certain services were fundamental, for example, radiology and emergency theatres, and it was therefore agreed that we would transfer after almost all other services had moved, but before the Emergency Department (ED). With the above in mind, and strongly believing that an extended period of double running 2 units would expose our patients to a greater degree of risk and stretch our critical care multi-disciplinary team (MDT) too thinly, we decided to undertake the complete transfer of our Critical Care Unit in 1 day rather than the three which had initially been proposed by the THLT.
Equipping the new critical care unit
In the week before the move, we transferred as much equipment as possible to the new unit, retaining only the minimum necessary to maintain patient care delivery in the old unit. So that equipment could be found quickly in an unfamiliar area, the new unit was stocked with clearly signposted and easily accessible emergency equipment such as defibrillators and airway trolleys, alongside equipment used routinely, for example, central venous catheters. We decided that patients on ventilators would be transferred on portable transport ventilators (Oxylog 3000 Drager, Germany), whilst their bedside ventilator (Evita V500 or V800, Drager, Germany) would be moved at the same time so that it could be set up for them immediately on arrival in the new unit. Routine care would need to continue during the day, and this required forethought about which procedures should be performed before Move Day or deferred until after. In the days leading up to Move Day, clinicians ensured that patients were optimised for the transfer so that treatments such as renal replacement therapy could be omitted or interrupted on the day of the move and recommenced later that day if required.
What services could we, as a tertiary critical care unit, reduce before the move?
On a local level, we emphasised the importance of having a period of reduced elective surgical activity to decrease our post-operative patient numbers (and thus associated workload) on Move Day. Consequently, it was agreed that elective activity requiring post-operative critical care admission would be reduced 9 days before the Critical Care Unit moving day. This enabled us to close the POCCU in advance of the move so that we only needed to move patients from two, rather than three, different units.
On a wider level of service provision, as we are a tertiary referral centre for patients with acute pancreatitis, thrombotic thrombocytopaenic purpura and high consequence infectious diseases (HCID), we liaised with the wider network well in advance and alternative tertiary referral centres were identified to provide cover during this period.
Unit staffing
Since it would be necessary to staff multiple units concurrently for a period of time on Move Day (ITU, HDU and POCCU in the old Royal alongside the one Critical Care Unit in the new Royal), a situation which would be compounded by the fact that staff would have minimal geographical and logistical familiarity with the new unit, much thought was given to staffing.
To aid the transition, we undertook a Staff Familiarisation Process over a number of months prior to Move Day. From early 2022, all staff in the MDT were regularly updated on the intended move plans. Staff were also asked to think about, and share their views, as to how we should, could, and would work differently on a single larger unit. This was particularly important given we were amalgamating three distinct teams, each with its own different familiarities, protocols and working patterns, into one which would work under one roof. Diminishing any anxieties related to this was essential given we had been forewarned by numerous parties not to underestimate how much a change of working pattern and location would affect staff morale and wellbeing. 8 Geographical familiarity was promoted by regular visits to the new hospital in the preceding months. Initially access was restricted to small groups; however, from mid-September onwards, access to the new building was less restricted and we were able to run some familiarisation sessions. These included practical ‘scavenger hunt’ sessions to aid logistical familiarity; for example, staff would be asked to ‘go and find X’ (e.g. a chest drain or a bed sheet). This also indicated where further familiarisation and education were needed.
In an attempt to both minimise disruption to the delivery of patient care, and increase safety during the transition, we made a decision to staff the both the new and old units simultaneously on Move Day. The additional medical and nursing staff required to facilitate this process were obtained through locum and bank shifts with funding agreed in advance by hospital management.
Patient risk-assessment
Our Liverpool Children’s Hospital colleagues had benefitted from moving the lower acuity patients first. This gave the staff time to settle into the unit and orientate themselves these patients before the sicker, higher acuity patients’ arrival. After consideration, we adapted this model to transfer patients in the following order: low risk, then high risk, then intermediate risk patients. As forestated, the benefit of moving low risk patients first was that staff unfamiliar with the new unit would be able to familiarise themselves whilst caring for those patients. Then, as they became more accustomed with the unit, and any problems identified on the day had been addressed, they would be better placed to accept the higher acuity patients. Additionally, it enabled the staff in the old unit to optimise the high acuity patients throughout the day (e.g. insert new lines, organise urgent imaging, etc.) before their transfer, while at the same time, the transfer teams’ familiarisation with the process and confidence would similarly increase. Finally, moving the high acuity patients second (as opposed to third), also allowed enough time to stabilise the sickest patients on their arrival in the new unit before the evening handover.
In order to determine a level of risk for each patient, a simple bespoke risk assessment tool was constructed and subsequently agreed upon after multiple round-robin discussions amongst our Consultant body and senior nurses. This assigned patients’ a value between 0 and 6 based on their current organ support and acuity (0 being lowest and 6 being highest risk for transfer; Table 1).
Royal Liverpool Hospital risk stratification of patients.
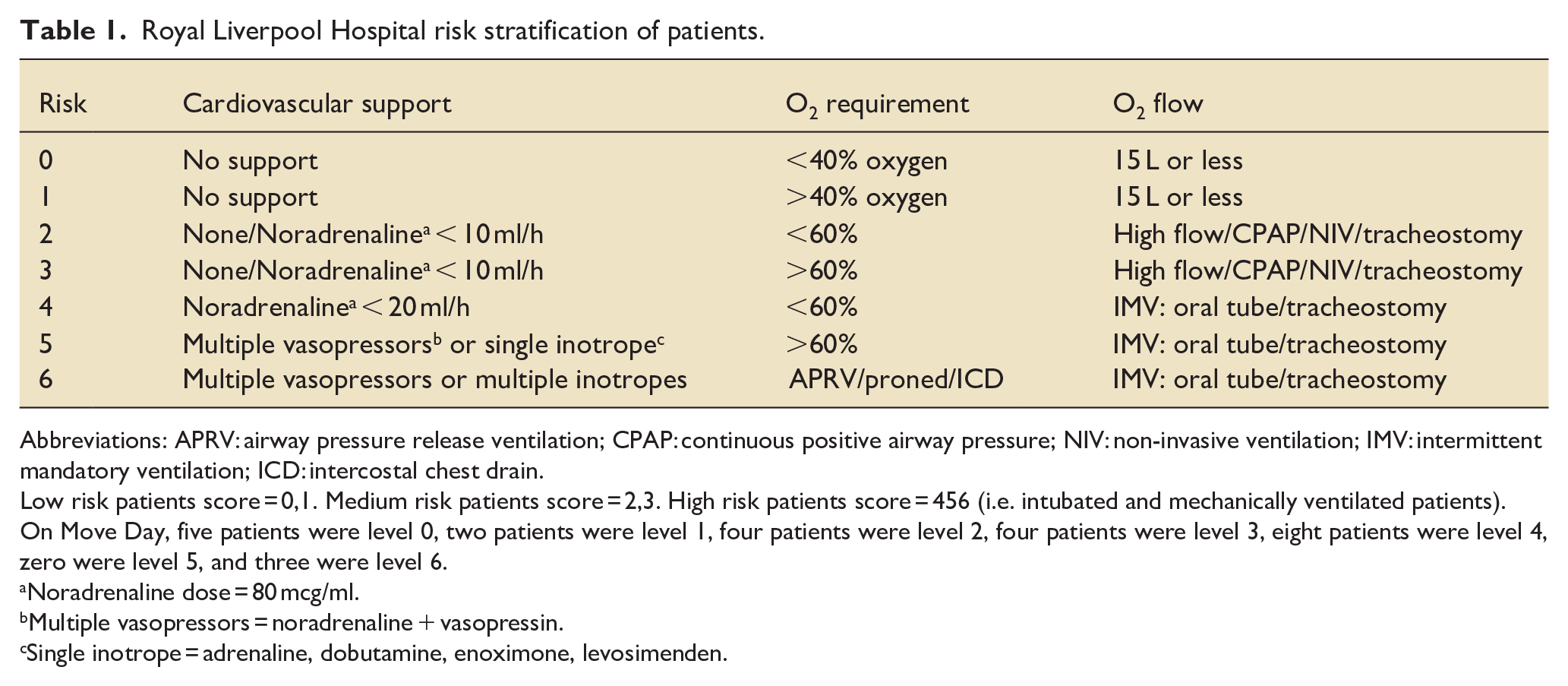
Abbreviations: APRV: airway pressure release ventilation; CPAP: continuous positive airway pressure; NIV: non-invasive ventilation; IMV: intermittent mandatory ventilation; ICD: intercostal chest drain.
Low risk patients score = 0,1. Medium risk patients score = 2,3. High risk patients score = 456 (i.e. intubated and mechanically ventilated patients).
On Move Day, five patients were level 0, two patients were level 1, four patients were level 2, four patients were level 3, eight patients were level 4, zero were level 5, and three were level 6.
Noradrenaline dose = 80 mcg/ml.
Multiple vasopressors = noradrenaline + vasopressin.
Single inotrope = adrenaline, dobutamine, enoximone, levosimenden.
We subsequently modified this score to give more weight to non-ventilated patients on high levels of oxygen as it felt more risky to move these patients than ventilated patients on less than 60% oxygen but on more vasopressors. For example, we graded patients on CPAP with high inspired oxygen concentrations as high risk, since a decision would have to be made about whether to intubate them for transfer. Patients for whom ceiling of care decisions had been made were also allocated to a high-risk group.
Whilst all patients were allocated a risk score (and thus category) on the day preceding the move by the consultants supervising the unit that week, the final categorisation of patients was confirmed on the morning of Move Day by the Gold Command Consultant.
Planning the route
Unfortunately, since the transfer route was not accessible to us until a few weeks before the move date, there was little time for insitu simulation exercises. The route included taking a lift down eight floors, travelling along a purpose-built transfer tunnel 600 m long (Figure 1), and ascending four floors in a lift in the new hospital. On an initial walk through of the route, it quickly became apparent that the narrow tunnel would be unsuitable for stopping to provide in situ treatment. An Emergency Stop-Point (ESP) was therefore set up just before the tunnel entrance (approximately halfway along the total route) in an old theatre recovery suite. Piped gas and centralised suction were available in this location and we equipped it with emergency equipment including an airway trolley, monitoring equipment, defibrillators and drugs commonly used on critical care such as spare propofol, along with emergency medications. On the day of the move, two anaesthetists staffed the ESP and remained there all day to aid familiarity with what was, and was not available to work with, so that quick decision-making was possible if extra resources were not available, and to act as extra pairs of hands on the day if required.

Transfer of a ventilated patient through the transfer tunnel.
The transfer teams
As many of the critical care staff would be busy with either pre-transfer reviews of patients on the old unit, or post-transfer reviews of patients on the new unit, our anaesthetic colleagues and operating department practitioners, freed up by the cancellation of elective operating lists, were utilised to form transfer teams. Using an Adult Critical Care Transfer Service was considered, however due to logistical and pragmatic reasons, we opted to use local staff. We calculated that four teams would make it possible to simultaneously have one moving outbound with a patient, one handing over on arrival, one returning inbound with equipment and one preparing to set off.
Each team had a designated team leader who was ultimately in charge of the decision-making en route in order to avoid multiple opinions being given at the same time (with the end result of nothing being done). Since the narrow tunnel allowed only one-way travel and transfer teams therefore had to return to the old unit with their equipment a different way, each team also included a member of staff who had already walked the complete route. For patients who were not for cardio-pulmonary resuscitation or treatment escalation from their status quo, a critical care consultant who knew the patient well was purposely chosen as their transfer team lead. We hoped this would diminish the chances of inappropriate treatment escalation en route.
A standardised Critical Care Transfer Checklist was written for patient transfers, and this was refined in response to feedback from the simulated transfers (Appendix 1). The checklist included the destination room number and contact numbers for the Command Centre, old units, new unit, and the emergency bay on the transfer route. We also provided a map of the new unit with room numbers and the transfer route printed on it. A standardised handover template was also formulated so the receiving clinical teams could be fully updated on the patient. On the transfers, full ICS/FICM monitoring standards and record keeping requirements were adhered to at all times
Communication with families
Alongside the necessity for clear communication between ourselves, we also recognised the risks associated with an intra-hospital transfer of patients and the anxieties this may provoke in patients and families. For this reason, we made a concerted effort to communicate openly and clearly with patients and their relatives on the unit. In the preceding weeks, information posters were put up in the relatives’ waiting rooms detailing the upcoming move and closer to the time individual letters were given to patients and their relatives explaining the move. Additionally, on the back of conversations with colleagues who had been involved in other hospital moves, we had made the decision that all patients would be transferred to the new hospital on the 1 day irrespective of how unwell they were. We were cognisant that the reason for the move was logistical as opposed directly necessary for patient care, however we also appreciated that any patient left behind would have limited access to clinical staff, equipment, and complimentary medical services and as such the risks associated with this outweighed the benefits of not moving them. This decision, and our rationale for making it, was again communicated to all patients (where possible) and family members in the days preceding the move.
We did not allow visiting on Move Day (though had anticipated to allow visitors for ‘end of life’ patients that morning if required), and one member of staff was allocated the role of informing the next of kin after each patient had safely arrived in the new unit.
Training and simulation
Simulation played a key role both in planning for Move Day and minimising anxieties. A Simulation Lead was appointed whose initial task was to anticipate both clinical and logistical issues related to the transfer, and then initiate monthly simulations of transfers in order to familiarise the team with the route and identify any unanticipated risks. Examples of questions to which we hoped to get answers from the three planned simulation exercises can be seen in Appendix 2.
In terms of the practicalities of conducting simulation sessions, in the preceding 3 months different scenarios were planned (Appendix 3) and appropriate transfer teams were chosen to suit the scenario. A high-fidelity mannequin was operated remotely by the Trust Simulation and Clinical Education Team who also filmed the exercise, logged events, and provided feedback. From consecutive simulation sessions we were able to identify some significant problems and consequently modify our plan and refine our Critical Care Transfer Checklist accordingly.
Move Day
On the day of the move a Command Centre was set up in an office on the old ICU. The Lead Critical Care Move Consultant acted as Gold Command and staffed the Command Centre along with Matron and Critical Care Head of Operations.
At 0700 the Move Lead went round the patients to finalise each patient’s risk score. The finalised list of patients, their risk categories, order of transfer, and destination bed in the new building was updated on a board in the Command Centre. Any necessary interventions for patients were considered and the order of transfers was adjusted accordingly.
Shortly after, the transfer teams all met on HDU for a briefing given by Silver Command, a role that was assigned to another critical care consultant responsible for co-ordinating the transfer. The timings of the day were outlined, including planned breaks. These breaks, in which breakfast, lunch and snacks were provided by the Trust, were essential not only to allow staff a period of rest, but also to give the receiving unit time to address any problems encountered and feed them back to the Command Centre in order to identify any emerging issues. The breaks also enabled teams on the old unit to prepare their patients following the morning clinical review.
Access to the transfer tunnel was confirmed by the Trust Move Lead and permission for an 0800 start was given. The Trust Move Lead was stationed at the entrance to the transfer tunnel, and as there was no mobile phone signal in the tunnel, communicated with the Gold Command via walkie-talkie.
To avoid confusion about whether the new unit was ready to receive another patient, constant communication was maintained between a single person at the old site and a single person on the new site (Gold Command and Admitting Consultant respectively). This ensured accountability for the decision-making process and allowed us to slow the pace of transfers between sites in the event of any unforeseen circumstances.
On reflection
In seven and a half hours we were able to safely transfer 26 critically ill patients and all their associated equipment from the old Critical Care Unit to the new Critical Care Unit. No patients deteriorated en route. Transfer of all 11 HDU patients was completed by 9am and the transfer of the 15 level three patients (high and intermediate risk score) commenced at 09:30 and was completed by 15:30 (allowing for a lunch break). Following the move, a formal debrief session was held and everyone involved with the process was invited to attend. Feedback on both what went well, and what proved challenging or could have been improved upon, was sought. Examples of positive feedback included that the transfer checklists provided assurance and made staff feel more secure when moving the patient, and the numerous simulation sessions were invaluable and undoubtedly enabled us to avoid many pitfalls. Challenges included overcoming transient IT failures upon our arrival (i.e. our patient notes software and printers were not working), and despite our best efforts, that we still encountered logistical problems on the day. One example of this related to the fact that it was taking longer to hand over each patient than had been anticipated and timetabled for, and thus we were at risk of creating a backlog of patients arriving in the new unit with others waiting precariously mid-transfer. Fortunately, having listened to others about the importance of clear communication on the day, involving only a single voice at each site giving the final go-ahead for transfer (as opposed to sticking to pre-planned timetabled departure times), we were able to adapt and stagger patients’ departures to allow for this.
In hindsight, perhaps one of the most underestimated yet fundamentally important impacts of the move was the depth of connection the staff felt with the old Unit. Despite being four walls made of brick and mortar, some of the staff had spent their whole career working on the old Unit and within that time had dealt with hundreds of patients and their families, each with their own stories and emotional journeys, highs and lows. Due to the recurrent delays in the opening of the New Royal, a sense of lassitude was present amongst the staff as they had come to believe that ‘we will never move in’, ‘it will be delayed again’, and we feared this would compound the problem and sense of loss. Efforts were thus made to try and mitigate this sense of loss from the outset. Early active engagement through regular communication with staff on the unit provided them with an opportunity both to express their concerns regarding the move and also to put forward their ideas – many of which the management team had not thought of. Familiarisation visits (as described above) provided opportunities to address the denial response (as anticipated according to Bridges’ model of transition, 9 and in the final week before the move a Goodbye Party was arranged to which many retired staff who had worked on the unit over the years were invited. At this, people were offered the chance to share their memories and staff left their handprints on the walls of the old ITU, complete with the number of years worked there (Figure 2). Despite all these efforts, in the weeks that followed the move it became evident that whilst the practical and logistical sides of the move had been accomplished successfully, much more still needed to be done regarding the human factors and to ensure that staff were happy and settling into the unfamiliar environment. Undoubtedly, whilst some thrived in the new unit, for others morale dipped and so the ward managers engaged in a pro-active programme of work centred around open communication, regular meetings and team building. As with the clinical medicine delivered on Critical Care, this process required patience and time, and now, reflecting after nearly 2 years have passed, this process of ’bedding in the staff’ seems to have been a success and the unit is thriving.

Saying goodbye to the old unit.
Conclusion
Given the potential risks associated with moving critically ill patients, it is somewhat surprising that very little has been written on the process of moving an Intensive Care Unit en masse. Admittedly, whilst some might argue that relocation of an entire unit between hospitals is an extremely rare circumstance and thus the manner in which it is done is not necessarily noteworthy, the requirement to relocate a unit quickly secondary to a major incident is quite plausible and therefore many of the lessons highlighted could be applicable in this set of circumstances.
In this article we have highlighted numerous matters that require consideration and careful planning in advance of the move, and Table 2 features our ‘top ten’ learning points. Clear communication and learning from others who had undertaken similar moves proved indispensable for us in the preparation stages, as did transfer simulation and the utilisation of a refined Critical Care Transfer Checklist. On reflection, one of the most underestimated, yet fundamentally important impacts of the move was the depth of connection the staff felt with the old unit and familiar colleagues. We had anticipated this and tried to prepare the staff accordingly; however, in the months that followed it became increasingly evident that much more work was required to ease the transition of people. This pro-active process required patience and time, and only now, some 2 years later, can we look around and see that the dust has settled.
Our top 10 considerations and learning points.
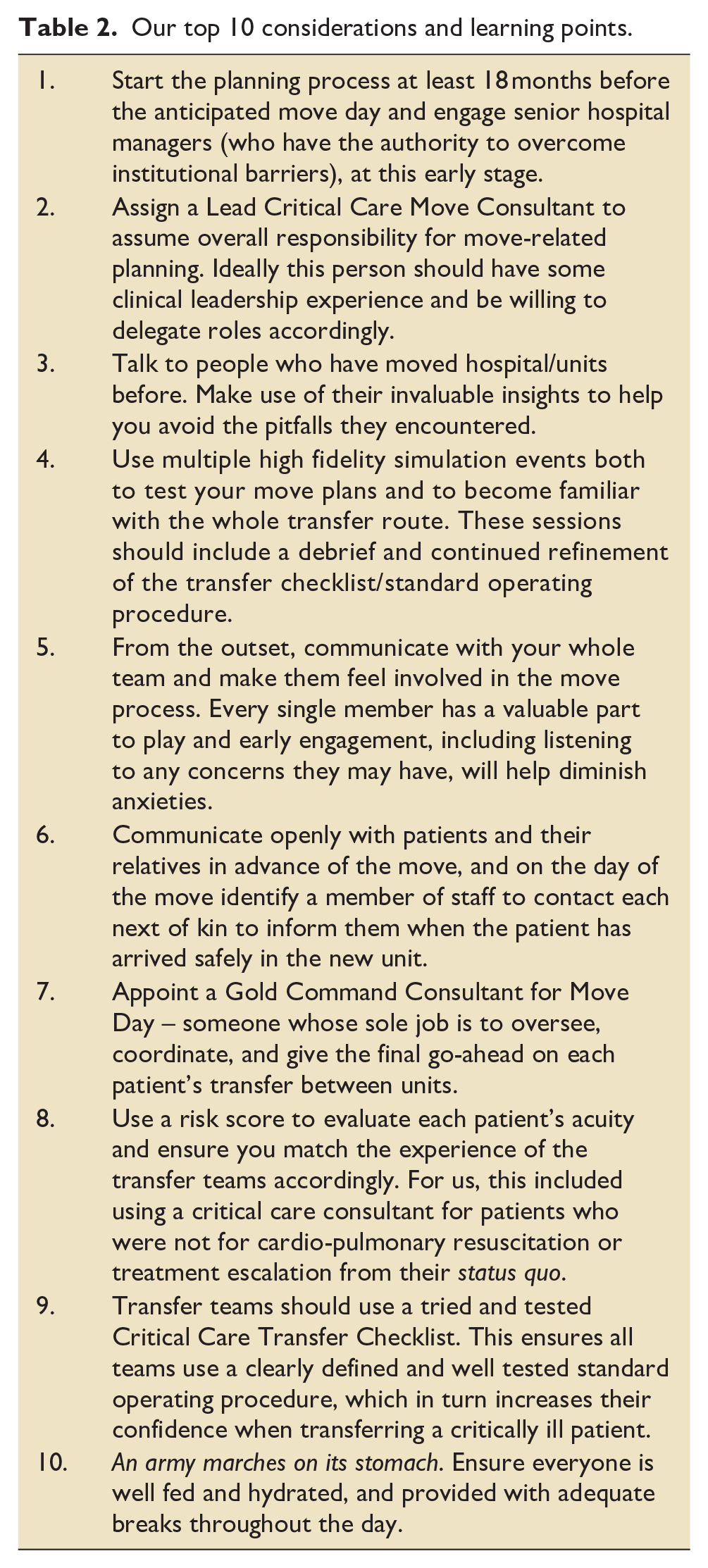
We hope this shared learning will help others avoid having to completely reinvent the ‘moving’ wheel.
Give me six hours to chop down a tree and I will spend the first four sharpening the axe.
Footnotes
Appendix 1
Royal Liverpool Hospital critical care transfer checklist.
Appendix 2: Simulation material
Examples of questions to which we hoped to get answers from the three planned simulation exercises:
*This was essential as it provided us with the reassurance that the whole unit (N = 36) would be transferred in 1 day.
**Should, for example, only clinicians who have cared for the patient in the days prior conduct the transfers of this group of patients?
Appendix 3
Three scenarios used for simulation testing alongside issues identified and learning points.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.