
Abstract
A core part of an intensivist’s work involves navigating the challenges of End of Life Care. While rates of survival from critical illness have gradually improved, 15%–20% of our patients die during their hospital admission, and a further 20% die within a year. 80% of our patients lack capacity to express their wishes with regard to treatment escalation planning. The critical care unit can be an excellent place to provide a good death, however the very nature of critical illness provides some obstacles to this. Prognostic uncertainty, time-pressured critical decision making, and lack of meaningful contact with a patient and their loved ones are but a few. In this article, we compare the ethos of critical care and palliative care medicine and explore how training in both of these specialities could be brought closer together and more formalised such that the intensivists of the future are more strongly equipped with the skills to shape a critical care unit to overcome these challenges and provide the best care to these patients, many of whom may be in the final phase of their life.
Navigating the intricacies of End-of-Life Care (EoLC) in critically ill patients is a core part of the work of an intensivist. Whilst survival after critical care admission has gradually improved over the last few decades, it remains that 15%–20% of our patients die during their hospital admission 1 and a further 20% will die within a year. 2 This palliative facet of our work is only likely to increase, as the age and comorbidity of our patients continues to rise 1 and new treatment options for chronic life-limiting illnesses evolve. This is framed in the knowledge that one in seven patients admitted to general ICUs in Europe have a diagnosis of malignancy, 3 and emergency critical care admission for those with non-haematological malignancy has a 41.7% ICU mortality. 4 In addition, over 80% of critical care patients lack capacity to make important decisions about withholding or withdrawing life-sustaining treatments and only 13% of patients dying in critical care have made any pre-emptive statement regarding their wishes. 5
With this in mind, there is an opportunity for intensive care to enhance training in EoLC, and formalise attainment of these skills, in order to navigate what can be an increasingly challenging but rewarding aspect of our work. In this article, we explore the concept of EoLC in an intensive care setting, the perceptions of palliative care and its utility in ICU, and examine current and future training pathways.
Challenges to providing a good death in critical care
The Faculty of Intensive Care Medicine’s ‘Care at the End of Life’ 6 states that ‘Critical care teams should be aware of the importance of a good death’. This is defined by the Institute of Medicine (1997) as one ‘free from avoidable distress and suffering for patient, family, and caregivers, in general accord with the patient’s and family’s wishes, and reasonably consistent with clinical, cultural, and ethical standards’. 7 Application of this standard presupposes specific knowledge and training which critical care staff may not necessarily possess.
Palliative care is defined by the World Health Organisation as functioning ‘. . .to maintain and improve the quality of life of patients and families through any stage of life threatening illness’. 8 It is clear from this definition that experience in palliative care can lie central to the provision of a good death.
There are two broad categories in which an intensivist may be involved in EoLC.
Withdrawal of life-sustaining therapy (WLST)
More than 80% of deaths in the intensive care unit occur in this way. 9 This may include:
- Palliative extubation
- Withdrawal of non-invasive ventilation or high flow nasal oxygen
- Transfer of a patient to a ward for further End-of-Life Care
- Organ donation in the context of death by either neurological or circulatory criteria
In the UK, these decisions are made together with the capacitous patient, or for patients who lack capacity, in accordance with relevant home nation legislation 10 and ethical guidance. 11 Many of these situations can prove particularly challenging even for the most experienced intensivist. Symptomatic airway obstruction, management of super-refractory status epilepticus, terminal restlessness, complex family dynamics, and ‘awake’ WLST are some examples.
Acute deterioration
Providing good EoLC in these emergency settings can be particularly challenging. Time-critical decision making, paucity of information, uncertain prognosis, patient lack of capacity or advance care planning, and inability to have meaningful contact with next of kin, are but a few of these difficulties.
The increasing availability of ICU-led medical interventions to ‘rescue’ a patient in life-threatening situations makes it more likely that patients will experience an intensive care admission. 1 This consequent uncertainty of outcome is a key reason why many clinicians may be unwilling to introduce or discuss the possibility of dying. This barrier often serves as a powerful justification for clinicians not communicating with a patient’s loved ones that they are ‘sick enough to die’. 12
A comparison of ethos – Two sides of the same coin
The decision to admit a patient to critical care involves a careful assessment of the balance of benefit versus harm by intensivists, referring teams, and the patient (or their advocate). Following admission, the primary focus is usually to correct acute physiological derangement, often in a time-pressured manner. Whilst this physiological focus is appropriate, it may come at a price, as it is possible to overlook the person as an individual. Although much progress to ‘humanise’ the ICU has been made, the ICU of the past was often viewed as a highly complex, efficiency-driven and dehumanising environment.13 –15
Palliative medicine, in contrast, holds the individual person with their particular wishes and goals at its very core: ‘to maintain and improve the quality of life of all patients and their families during any stage of life-threatening illness’. 16 The approach is one into which medical interventions slot as only one aspect of care, considering also a person’s physical, emotional, social, spiritual (not necessarily faith-based), psychological and family needs.
Palliative care physicians and specialist nurses are experts at symptom control, nutrition and hydration decisions, advance care planning and complex communication at the end of life. They are also often very skilled at coordinating input from multiple different medical specialities; all skills very pertinent to critical care.
Intensive care medicine and palliative care can, as such, be viewed as specialities existing on two sides of the same coin, intensive care medicine often has a necessary tendency to focus on the physiological, but increasingly considers more holistic aspects, whereas palliative care began with the person and increasingly encompasses the physical and pathological, as part of that whole.
This idea is neatly described by Byock. The primary goal of each respective specialty, represents the secondary goal of the other. 17
Challenging perceptions of palliative care
Over the last two decades there has been an increasing drive to challenge the traditional model of curative care needing to cease before palliative care can commence. An early consideration of palliative aspects sitting in parallel to curative measures is key to this concept.
The continuum displayed in Figure 1 introduces an approach which acknowledges that the relative emphasis of curative versus palliative strategies may change over the course of an illness. At most points along the way both approaches can sit alongside and complement one another. Early appreciation of goal-setting, symptom control, and assistance with communication, are just a few of the skills traditionally thought to be ‘palliative’ in nature, which can be of benefit much before a patient is considered to be at the ‘end of life’. Clinical prediction of a patient’s closeness to death can be highly varied and often inaccurate, further hindering timely initiation of palliative support. Earlier adoption of these concepts is not a new idea, but has been relatively slow to mature through medical specialities such as intensive care medicine.
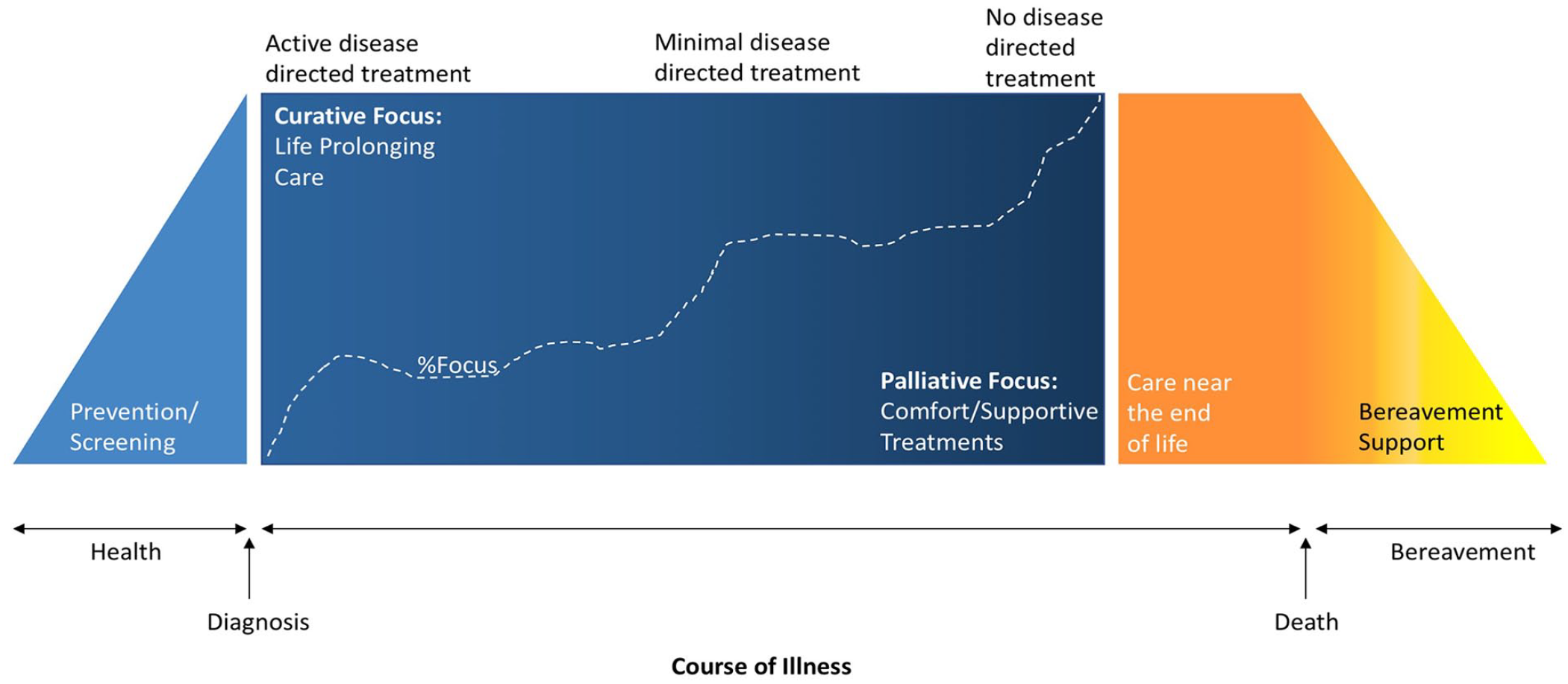
Palliative Care Continuum describing the parallel relationship between curative and palliative care during the course of illness.
This move is exemplified by Rao et al. who describe palliative care referral made for their patients at the time of decision to start Extracorporeal Membrane Oxygenation (ECMO) for SARS CoV2 infection and refractory hypoxaemia. This was done after recognition that this patient cohort had high morbidity and mortality, and was associated with improved symptom control and overall satisfaction of patient and family. 19
Other vital areas where this parallel approach can prove useful include 20 :
- Early and skilled application of ethical and legal frameworks of decision-making
- Transition-planning
- Management of family conflicts
- Support for families during the dying process
- Support for both patient and family if there is significant morbidity suffered after critical illness
Upskilling the intensivist
The Faculty of Intensive Care Medicine (FICM) defines EoLC as a ‘core skill’ for the intensivist. The new 2021 curriculum capabilities include:
- ‘Facilitating discussions focussed on how to manage end of life care with patients and their families’.
- ‘ The process of withholding or withdrawing life-sustaining treatments and providing palliative care whilst maintaining respect for cultural and religious beliefs’
- ‘Managing the withholding or withdrawal of life-sustaining treatment, discussing end of life care with patients and their families and facilitating organ donation where appropriate’.21,22
Specialty Training in Palliative Medicine has modernised to involve a dual CCT with General Internal Medicine. The ethos driving this shift is ‘increasing evidence to support early palliative care involvement’ across a wider range of patient groups. 23 The new curriculum reflects an evolution towards providing palliative care in parallel with curative intent, whilst simultaneously managing symptoms, expectations, and complex decision-making. It also places a formal emphasis on the ability to support colleagues in challenging situations and patients with complex psychosocial issues. Dealing with patient death has been identified as a major factor in the growing problem of physician burnout. The principles of compassionate leadership, interdisciplinary teamworking, and not seeing patient death as a failure, all form part of a palliative care ethos which can help developing intensivists deal with the emotional stresses of this work. 16
Traditionally, EoLC training for critical care clinicians in the UK, has involved observation and participation in the management of critically ill patients transitioning to EoLC. Experience is often dependant on unit case mix and acuity rather than structured training per se. There are obvious limitations to this model. Although the less summative design of the new (2021) UK ICM curriculum allows a more patient-focussed and streamlined approach, a formative approach to experience potentially risks greater variability in EoLC exposure and training across the UK (or even within regions themselves).21,22
In addition to the core curriculum, trainees on a single CCT training pathway in ICM will undertake a Specialist Skills Year (SSY) in one of 12 areas, one of which is in ICM ‘Partner Specialities’. SSYs can be undertaken in highly specialised areas of ICM such as Extracorporeal Membrane Oxygenation (ECMO), pre-hospital medicine and home ventilation.
Palliative Care is not currently listed as one of these medical specialities. 24
Current views of UK ICM specialty trainees
To explore the training needs of ICM trainees, the authorship distributed a survey, available to all ICM specialty trainees in the UK. Of the 784 specialty trainees currently noted to be in training, we received responses from 75 (9.6% return rate).
We gained a breadth of training stages, with median clinical experience in critical care of 5 years (mean = 5.16, IQR = 4). Table 1 gives a breadth of the responses to questions about training in EoLC. Common themes included the inherent uncertainty of prognosis and inability to directly communicate with patients as barriers to decision-making. Over a third of responses strongly agreed that observed conversations with palliative care specialists would be beneficial to their training. Some of the non-medical benefits of this mentioned included teaching on the non-medical aspects of dying, such as financial support for families, and complex discharge planning.
Comments from UK ICM specialty trainees regarding End of Life Care (EoLC).
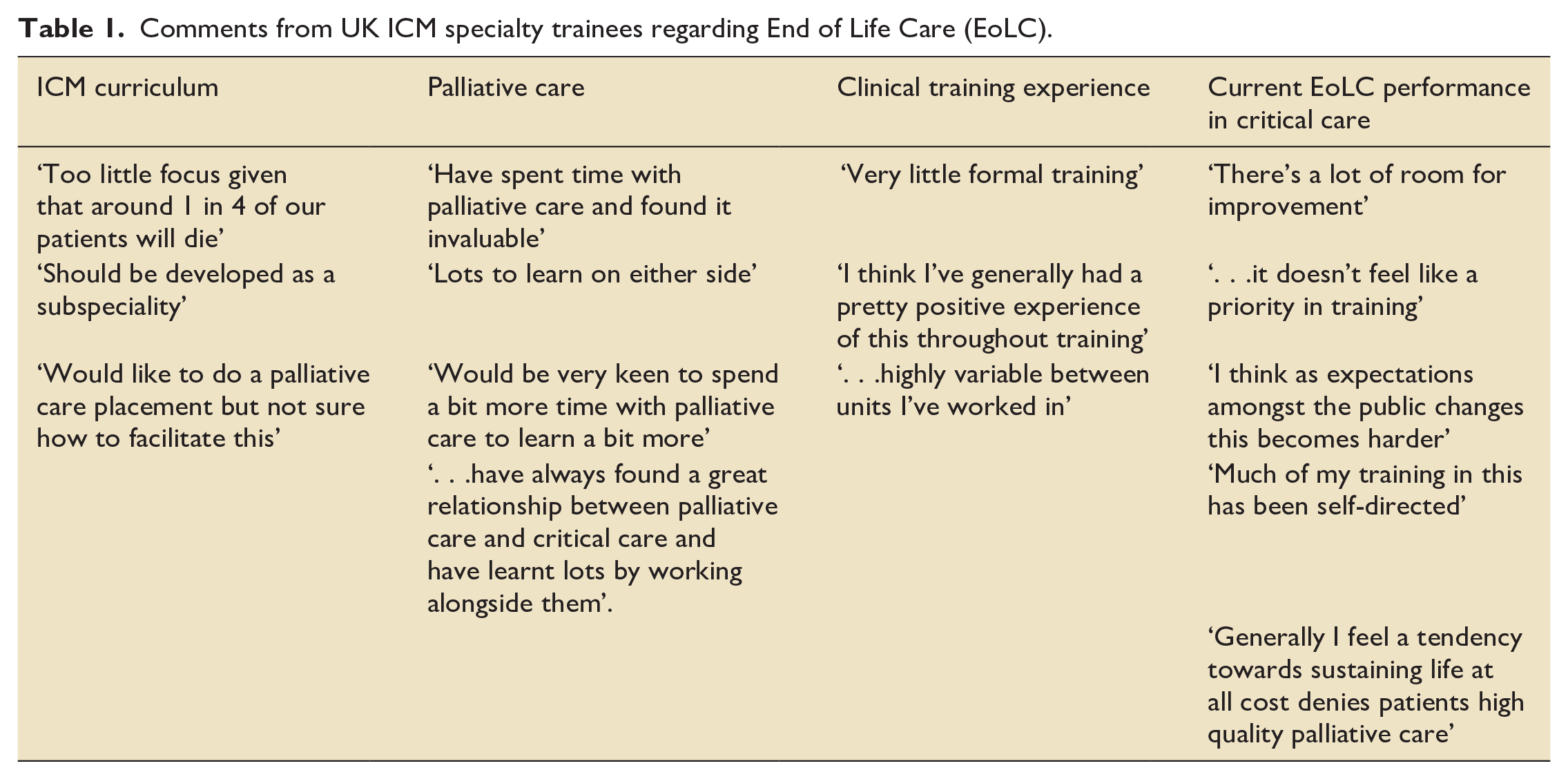
Over half of the trainees who responded did not feel confident about making decisions regarding hydration or nutrition at the end of life. This was noted to be a topic of contention with families or loved ones, as it is often feared that the patients may be ‘starved to death’ at the end of life.
Respondents commonly spoke of a lack of formal training and a tendency towards only observational learning, remarking that previous exposure to palliative care through working in general medicine translated well to critical care.
Shared learning for the future
It is now ‘widely accepted that ICU clinicians need training and expertise in primary palliative care skills’. 20 Much as in other subspecialities of ICM, we are expected to become ‘medical experts’ 21 in EoLC. Given the exceptional challenges we may face to provide a good death for each of our patients, it could be argued that there is an opportunity to enhance our training experiences in this area.
The potential benefits of a model of closer co-working between specialities was exemplified during the COVID-19 pandemic. Many critical care departments invited their palliative care colleagues into their units to not only help with increased workload, but to aid with improvement in symptom management, decision-making, difficult conversations via telemedicine, and bereavement support for families and professionals. 25
This crossover of training between ICM and Palliative Care has the potential to share mutually beneficial learning. Clonidine, for example, has been in long-established use in critical care for its role as a sedative and analgesic. It is now being trialled in patients with life-limiting illness, who suffer complex pain in palliative care settings and has so far been shown to be safe with promising indications of efficacy. 26 There is evidence that intensivists are good at recognising when a patient is dying, but only do so when the individual is very close to death. This naturally means that these patients have variable consideration for symptomatic relief and hydration/nutrition decisions in their final hours, or days. 27 This could be remedied by understanding how to recognise this process earlier. Both specialities face the challenges of supporting colleagues in what can be very challenging and emotional circumstances. Robust support systems, both personal and departmental, are vital to managing complex ethical scenarios when practising modern critical care; formal education, or clinical experience of this, could be gained through learning from our palliative care colleagues. 28
One example of this is in the training of critical care nurses to become ‘palliative care champions’ by palliative care colleagues. This interdisciplinary model has been shown to improve regularity of communication with patient relatives, regularly update staff on modern palliative care practices, and establish peer support mechanisms within the department. 29
Recommendations
Given the concepts discussed above, we recommend:
- It would be useful to explore ways in which training can formally integrate time within palliative care. This could include a recognised Special Skills Year (SSY) module or time spent during the Stage 1 Medicine component
- Integration of palliative care teams within the education of the critical care unit. This could include components of regular teaching within specialty training or CPD.
- Consideration of the value of collaborative work within local unit guidelines. For example, clinical guidance for end of life care of withdrawal of life sustaining therapy within critical care written with palliative care input.
Conclusion
The intensive care unit can be a well-equipped, well-trained, and highly personal place in which to provide a good death. It can also be an excellent place to conduct reasoned and nuanced discussions surrounding patients’ wishes and goals in their last year of life. Despite these common themes, it is easy to see critical care and palliative care as two polar opposites (the technical medicine vs the talking medicine). However, selected adoption of an early combined curative and palliative approach can produce significant benefit for our patients . ICM doctors in training spend many years learning a meticulous approach to organ support and complex decision making. In the coming years, the modern intensivist will face increasing challenges surrounding treatment escalation and death in the critical care unit, for which enhanced cross specialty palliative care training can only be of benefit.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.