
Abstract
Introduction:
Auto-intoxication represents a considerable number of Intensive care unit (ICU) admissions. Literature focusing on characteristics and outcomes of ICU-admitted auto-intoxicated patients is limited.
Objectives:
We aimed to identify the quantity of intensive care admissions attributable to auto-intoxication in a Belgian tertiary center, to examine characteristics and outcomes of these patients, and to assess the impact of the covid-19 pandemic on these variables.
Methods:
In this retrospective cohort study, all patients admitted to the ICU of JESSA hospital, Hasselt, Belgium with a diagnosis of auto-intoxication between January 1st 2017 and December 31st 2022, were included in the study. We collected data on patient characteristics, comorbidities, type of intoxication and outcomes including the length of ICU and hospital stay and mortality.
Results:
In total, 342 patients were included in the dataset, covering 2.44% of all ICU admissions from January 1st 2017 to December 31st 2022. Although auto-intoxication occurred in all age-categories, the age group from 18 to 29 years old, showed the highest prevalence (24%). More woman (57.6%) than man (42.4%) were included in the study. Of all included patients, 21.6% had a history of previous suicide attempt and 36.5% of previous auto-intoxication. The most common substances ingested were sedatives (44.4%), illicit drugs (20.2%), analgesics (17.8%), and antidepressants (16.7%) whereas in 54.1% of the cases, a combination of substances was ingested. Type of intoxication was separated into four groups: suicide attempt, accidental, iatrogenic and recreational use with suicide attempt accounting for 71.3% of all auto-intoxications. The prevalence of ICU-admitted auto-intoxicated patients remained stable over the 5-year study period. An impact of the Covid-19 pandemic on this prevalence could not be established. Overall mortality was low with an ICU- and hospital mortality of 1.75% and 2.6% respectively. Total mortality at time of dataset closure, on the other hand, was 7.2%.
Conclusions:
The impact of auto-intoxication on ICU resource utilization is relatively high and the risk of recidivism is substantial. ICU- and in-hospital mortality after auto-intoxication is low, although these patients have a substantial risk for death in years to come after hospital discharge.
Introduction
Intentional poisoning is a relevant public health issue responsible for a considerable number of cases of morbidity and mortality worldwide. The percentage of patients presenting with an acute intoxication at the emergency department with need of intensive care unit (ICU) admission is substantial and varies from 3.7% to 40%.1 –4 On average, the prevalence of intoxicated patients within the total ICU population is 1.5%–3.7%. 5 A large Dutch cohort study comprising data of 81 Dutch ICUs found a relatively low in-hospital mortality of 2.1% after ICU admission due to acute intoxication. 1 In contrast, long-term mortality was found to be substantially higher with a mortality rate 9.3% within a 2 year time frame after ICU admission. 1 Therefore, an ICU admission may be interpreted as a warning sign for mortality in the next years.
An Irish study showed that the most common causes for ICU admission due to intoxication are sedative and opioid abuse (30% and 25% respectively). 6 In Belgium, the prevalence of opioid use between 2006 and 2017 reached 10% of all inhabitants7,8 and Belgium ranks 3rd in the list of European countries with the highest daily use of opioids.7,8 Moreover, in 2020, 21% of all Belgian inhabitants used sedatives. 9 Since the use of sedatives or opioids carries an inherent risk of respiratory depression, especially when used in inappropriate (to high) doses, intoxication with these types of medication results frequently in life-threatening situations necessitating tracheal intubation and mechanical ventilation and thus contributes to a high resource utilization and cost.
The covid-19 pandemic may have resulted in an increase of self-poisoning rates and subsequent ICU resource utilization. Stressful life events, extended home confinement, worry, overuse of the internet and social media were all factors that influenced the mental health of adolescents during the pandemic. 10 In view of the pandemic’s impact on mental illness, social disadvantage, and the pandemic’s impact on increased alcohol use, increased suicidal behavior has been suggested. 11 Adolescents were more prone to alcohol and cannabis abuse during the pandemic with 49.3% engaging in drug use alone. 10
To our knowledge, concrete numbers and studies on auto-intoxication necessitating ICU admission are missing within the Belgian context. Insight on the characteristics and outcomes of these patients is therefore limited. Analyzing their characteristics and outcomes may help to identify those patients who may benefit from specialized follow-up aiming to decrease the incidence of long-term sequelae and death.
The aim of this study is twofold: First, to identify the quantity of ICU admissions attributable to auto-intoxications in a Belgian tertiary center and the impact of the covid pandemic on this quantity. Second, to examine characteristics and outcomes of this patient cohort.
Methods
Study design
This retrospective single-center, investigator-initiated, longitudinal cohort study was performed at the Jessa Hospital, Hasselt, Belgium. This study is approved by the ethical committee of Jessa Hospital, Hasselt, Belgium on April 25th, 2023 (f/2023/041), and registered on clinicaltrials.gov on September 15th, 2023 (NCT05933421). Considering the retrospective nature of this study, written informed consent was waived. This study is reported according to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement. 12
Patient selection
All patients diagnosed with auto-intoxication admitted to the ICU of the Jessa hospital between January 1st 2017 and December 31st 2022, were included in the study. There was no age limit. Data from consecutive patients admitted to the ICU were entered into a customized database, which was retrospectively reviewed. Patients were classified into two groups, survivors and non-survivors.
Standard admission and treatment procedures
In the Jessa Hospital, patients were admitted to the ICU when an auto-intoxication with any pharmaceutical or recreational drug with the potential to induce (asymptomatic) organ failure occurred or when confirmed signs and/or symptoms of organ failure (clinical, biochemical, or ECG) were present. In addition, patients who deteriorated at the ER department, that is, paCO2 > 45 mmHg, post-ingestion seizures, unresponsive to verbal stimuli, non-sinus cardiac rhythm, second- or third-degree atrioventricular block, low systolic blood pressure, prolonged QRS,. . . were admitted to the ICU.
The following criteria for the initiation of specific treatments were followed. A dose of 1 g/kg activated charcoal was given within a timeframe of 3 h after toxin ingestion with a maximum dose of 50 g. Sodium bicarbonate was administrated when intoxication with sodium channel blockers was present when an acidemia with a pH < 7.2 occurred or if indicated urinary alkalinization for enhanced elimination of toxins was necessary. About 20 mEq potassium chloride was given orally in patients with mild to moderate hypokalemia (3.0–3.4 mEq/L) two to four times a day. Patients with severe hypokalemia (2.5–3 mEq/L) or symptomatic hypokalemia were given intravenous therapy (10–40 mEq/h depending on the severity). In case of respiratory failure mechanical ventilation was initiated. Antidotes were administrated as described by Tintinalli et al. 13 Hemodialysis was predominantly used for the treatment of renal failure. Antibiotics were administrated only when signs of a bacterial infection were present. Vasopressor/inotropic therapy was administered in case of hypotension with a systolic blood pressure < 90 mmHg, when intravenous fluids failed to restore tissue perfusion, or when aggressive administration of fluids was contraindicated.
Data collection
The following data were collected from the patient files: baseline characteristics comprising age, gender, BMI, comorbidities, previous suicide attempt, previous intoxication, smoking, use of alcohol and home medication; length of stay in the ICU and length of stay in the hospital; cause of admission at ICU; treatment and outcome. Vital sign abnormalities were studied and defined as followed: tachycardia (= heart rate > 100 bpm), bradycardia (= heart rate < 30 bpm) and systolic blood pressure. ECG abnormalities examined included prolongation of intervals (PR > 200 ms, QRS > 100 ms, and QTc > 420 ms). Type of drugs ingested, and number of drugs involved for each intoxication were determined. Type of intoxication was separated into four groups: suicide attempt, accidental, iatrogenic and recreational use. Comparison was made between survivors and non-survivors to identify underlying risk factors. Furthermore, yearly trends and impact of covid-pandemic (2020–2021–2022) were analyzed.
Statistical analysis
Continuous data are shown as median (25%, 75%) and categorical data are presented as frequencies (%). Comparisons between groups were performed with the Mann Whitney U test for nonnormally distributed data. Categorical variables were analyzed with a Chi-Square test. To predict mortality, univariate and multivariate logistic regression was performed for the binary variables and univariate and multivariate linear regression was performed for the continuous variables. All variables with a p-value <0.10 were fitted in the models. A p-value <0.05 was considered statistically significant. All analyses were performed with SPPS Version 28. Graphs were made with GraphPad.
Results
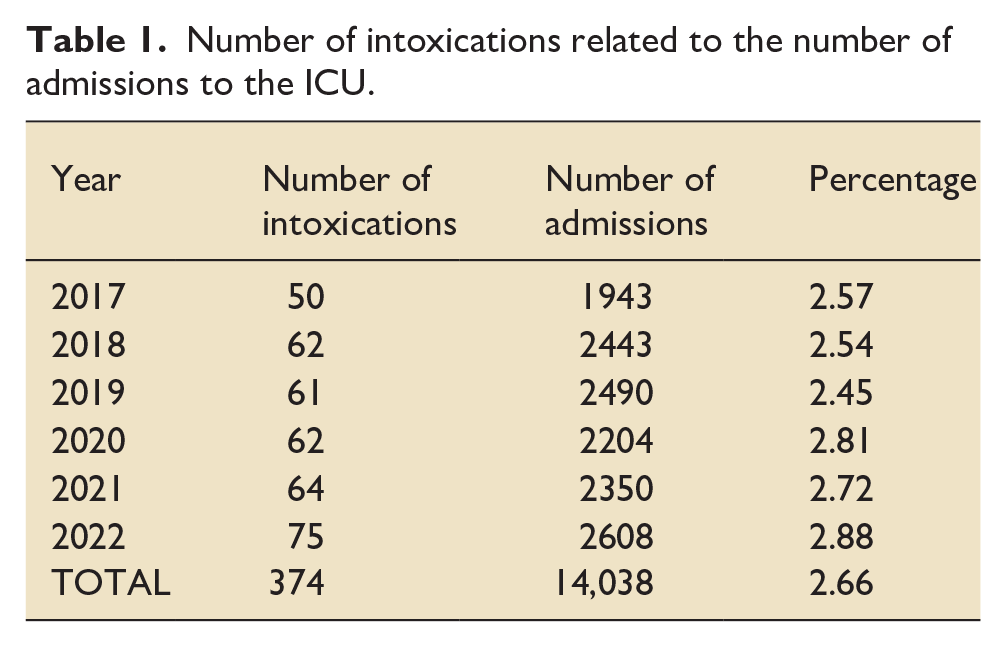
Between January 1st 2017 and December 31st 2022, a total of 14.038 patients were admitted to the ICU, including 374 patients (2.44%) with a diagnosis of auto-intoxication (Figure 1). Within this time frame, 28 patients were admitted more than once because of auto-intoxication (n = 4: three admissions and n = 24: two admissions). Twenty out of 28 patients (71.4%) were re-admitted with the same type of intoxication and toxicological result as the initial admission. Two of these patients died (7.1%). Correction for multiple admissions resulted in data of 342 patients for final analysis. The percentage ICU patients diagnosed with auto-intoxication remained stable over the 6 years of investigation (Table 1).
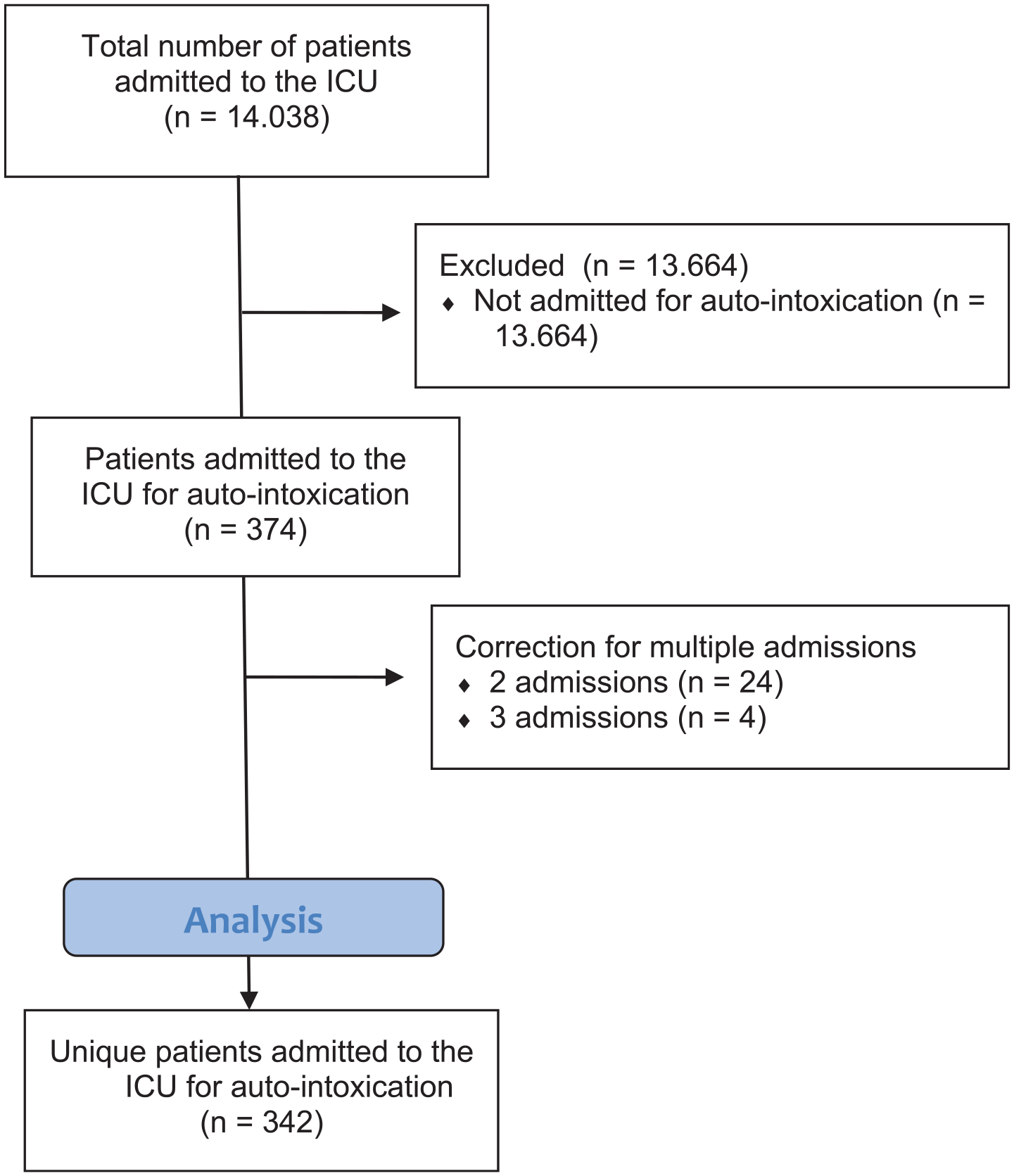
STROBE flowchart depicting inclusion and exclusion.
Number of intoxications related to the number of admissions to the ICU.
Baseline patient characteristics are presented in Table 2. Of all patients admitted, 145 (42.4%) were male and 197 (57.6%) female. The age distribution is shown in Figure 2. The mean age at admission was 39 years. 21.6% of included patients had a history of previous suicide attempt and 36.5% of previous auto-intoxication.
Baseline patient characteristics.
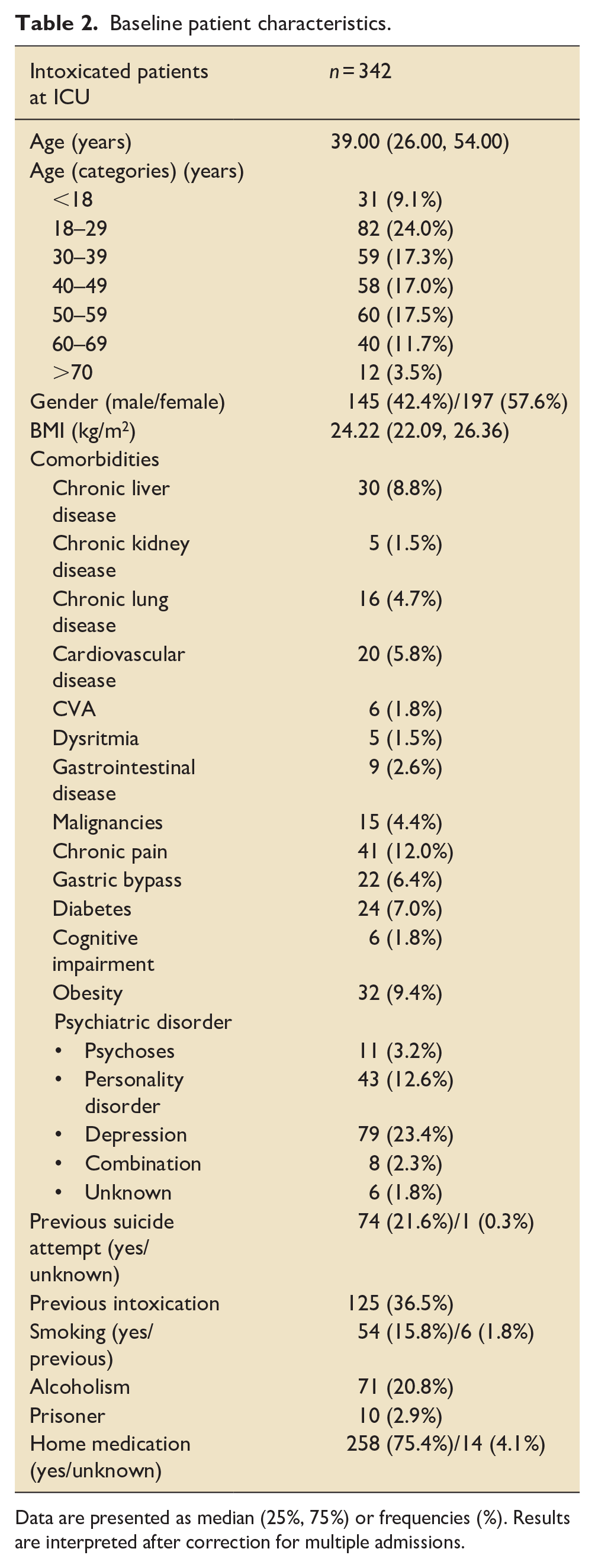
Data are presented as median (25%, 75%) or frequencies (%). Results are interpreted after correction for multiple admissions.
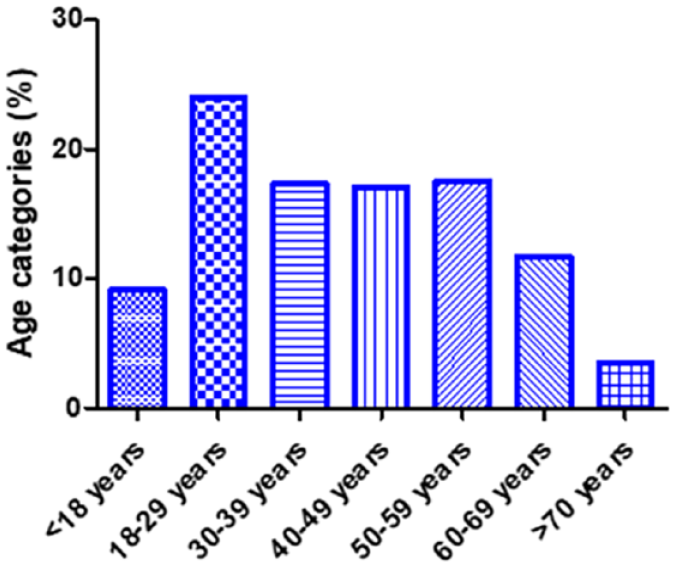
Age distribution of patients admitted to ICU with auto-intoxication.
On ICU admission, the mean SOFA and APACHE IV score was 3.00 and 44.00, respectively (Table 3). The majority of patients (66.4%) were admitted for monitoring of vital parameters, 20 (5.8%) patients were admitted because of respiratory failure and 49 (14.3%) because of coma. The most common substances ingested were sedatives (44.4%), illicit drugs (20.2%), analgesics (17.8%) and antidepressants (16.7%). The least frequent type of intoxication was poisoning (3.5%; ammonia, ethylene glycol, glycophosphate, formic acid and other household products). In 54.1% cases, a combination of substances was ingested. Type of intoxication was separated into four groups: suicide attempt, accidental, iatrogenic and recreational use with suicide attempt accounting for 71.3% of all auto-intoxications.
Clinical parameters and description of intoxication.
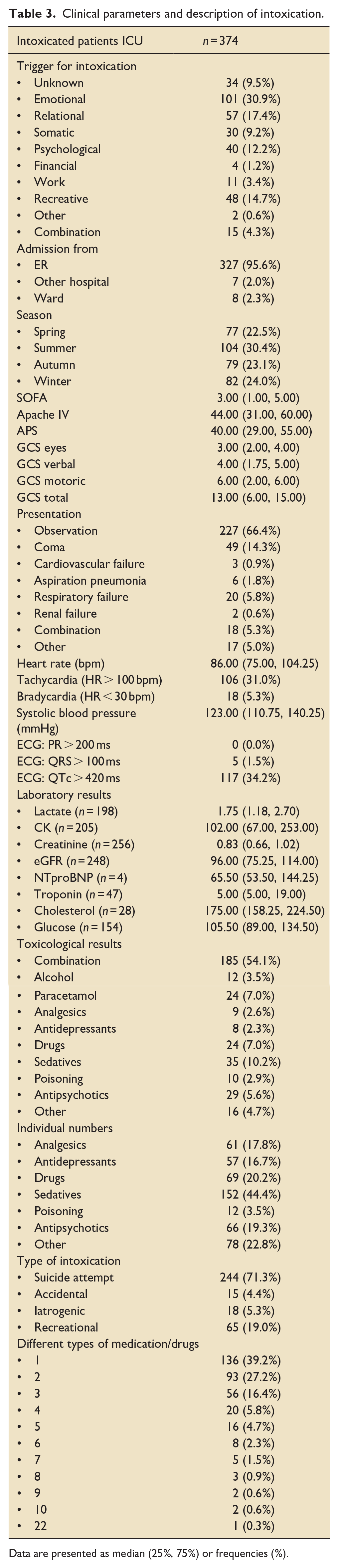
Data are presented as median (25%, 75%) or frequencies (%).
Clinical parameters and treatment strategies applied at the ICU are listed in Table 4. In total, 87 (25.4%) patients needed mechanical ventilation, 40 (11.7%) were treated with vasopressors or inotropes and 3 (0.9%) with hemodialysis. An antidote was given in 126 (36.8%) patients. About 29.1% of the cases only needed monitoring of vital parameters and no further intervention was applied. A sub-analysis was performed between these patients who were admitted for observation (n = 109, 29.1%) versus patients who received treatment (n = 265, 70.9%). No differences were found in age, gender, BMI, and most comorbidities (Supplemental Table 1). In the observation group, more patients were cognitively impaired compared to the treatment group (5 (4.6%) vs 3 (1.1%), p = 0.04). The length of stay in the ICU and the hospital was significantly shorter in the observational group compared to the treatment group (Supplemental Table 2).
Clinical parameters and treatment strategies applied at the ICU.
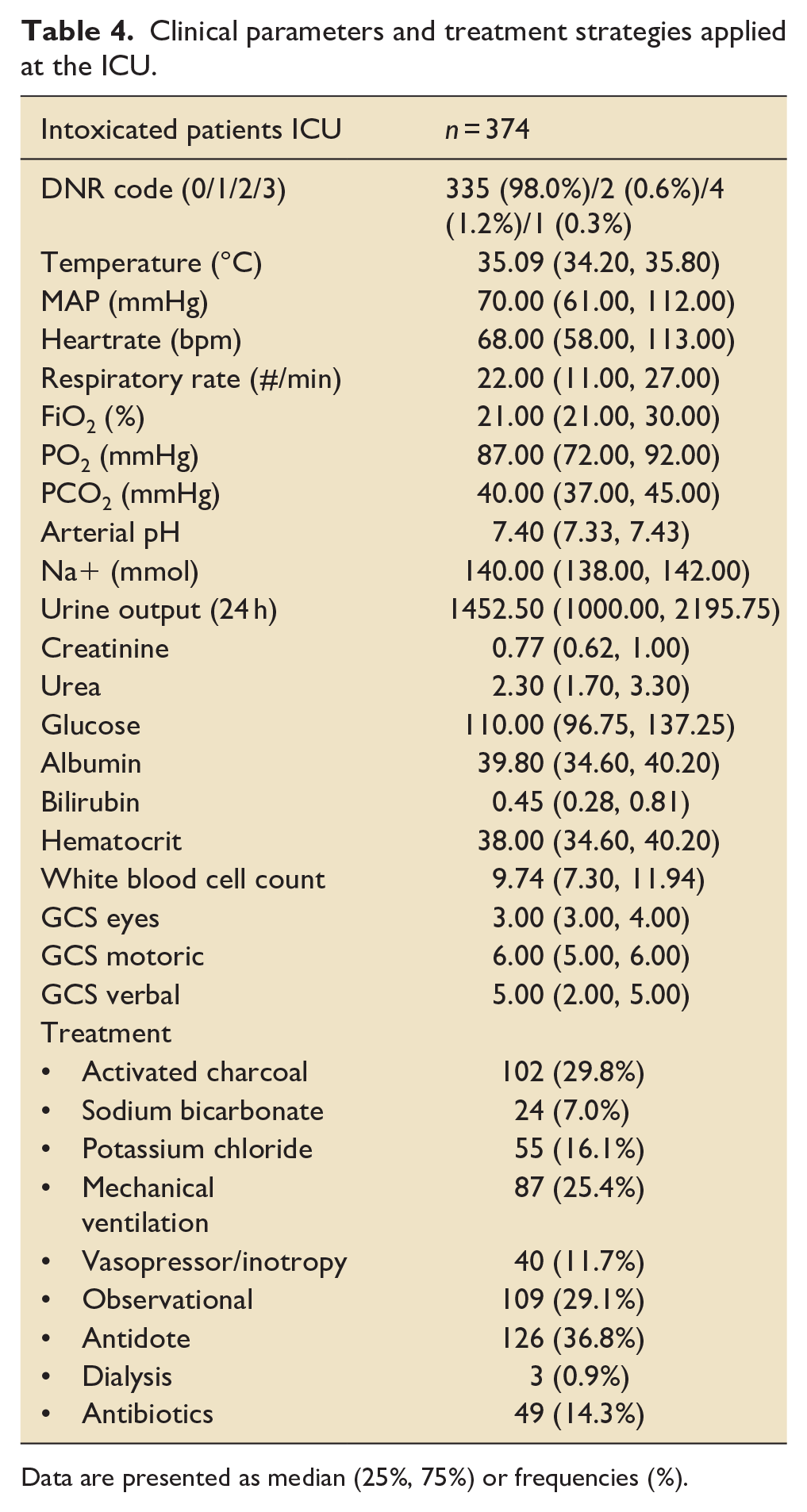
Data are presented as median (25%, 75%) or frequencies (%).
The median length of stay in the ICU was 1 day, whereas the median length of stay in the hospital was 3 days (Table 5).
Outcomes.
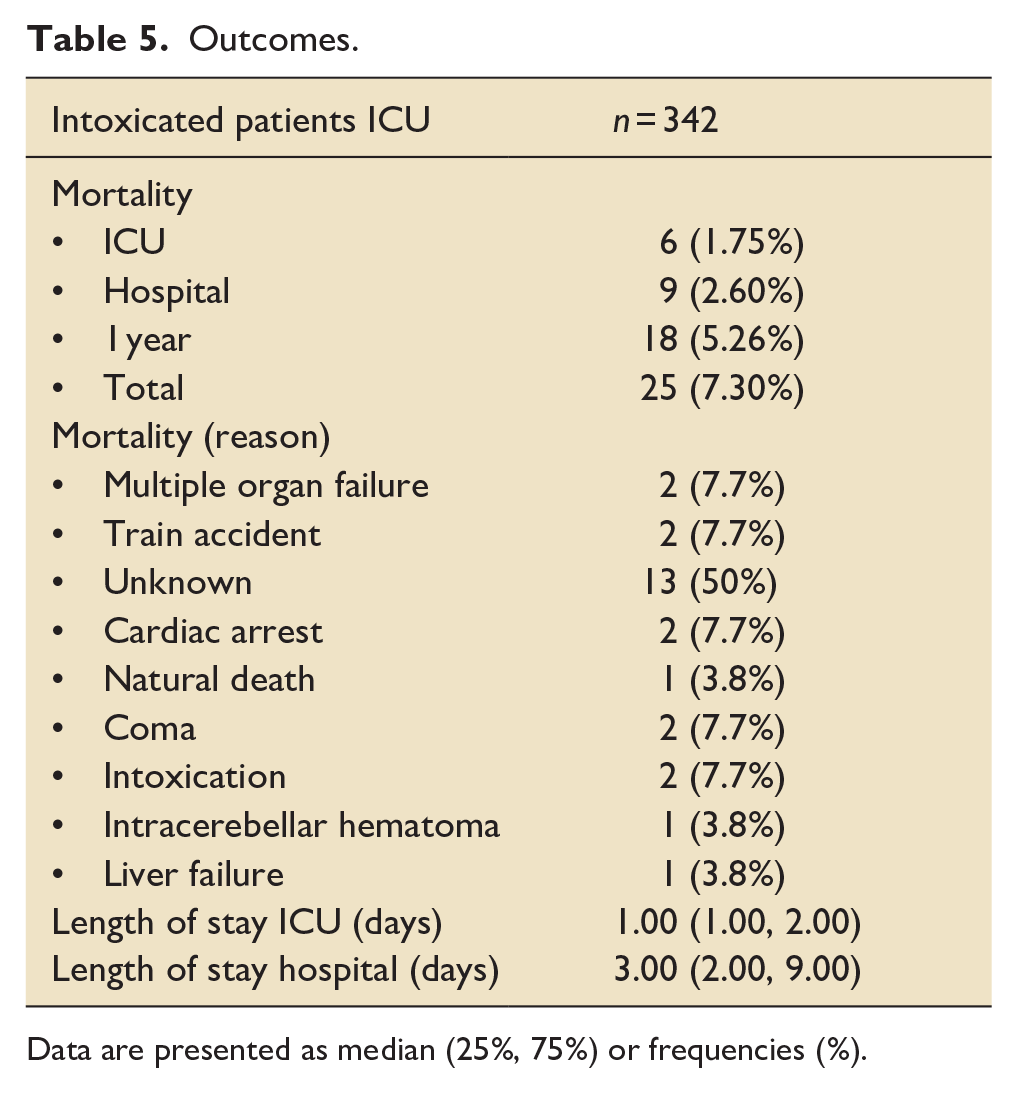
Data are presented as median (25%, 75%) or frequencies (%).
A total of six patients died in the ICU (ICU mortality rate, 1.75%), three patients died after ICU admission while they were still in the hospital (in-hospital mortality rate, 2.60%), as shown in Table 5. Another nine patients died 1 year after admission, with a total 1-year mortality of 18 patients (5.26%). Total mortality 1 year after dataset closure (March 31st 2023) was 7.30% (n = 25). In 50% of these cases, the reason for mortality was unknown. One-year mortality (n = 18, 5.26%) was significantly higher than in-hospital mortality (n = 9, 2,60%), p < 0.001 (Chi-square).
To identify risk factors for mortality, a comparison was made between survivors and non-survivors (Table 6). In the non-survivor group, 13 (52%) patients were male and the median age was 48 years, compared to 132 (41.6%) male patients with a median age of 38 years in the survivor group (p = 0.31 and p < 0.01 respectively). No significant difference in surviving rate was found for intoxications during the corona pandemic versus before (p = 0.80). Chronic liver disease, CVA and cardiovascular disease are comorbidities which are significantly related to a higher mortality. No significant difference in mortality was found in presence of a psychiatric disorder.
Survivors versus non survivors.
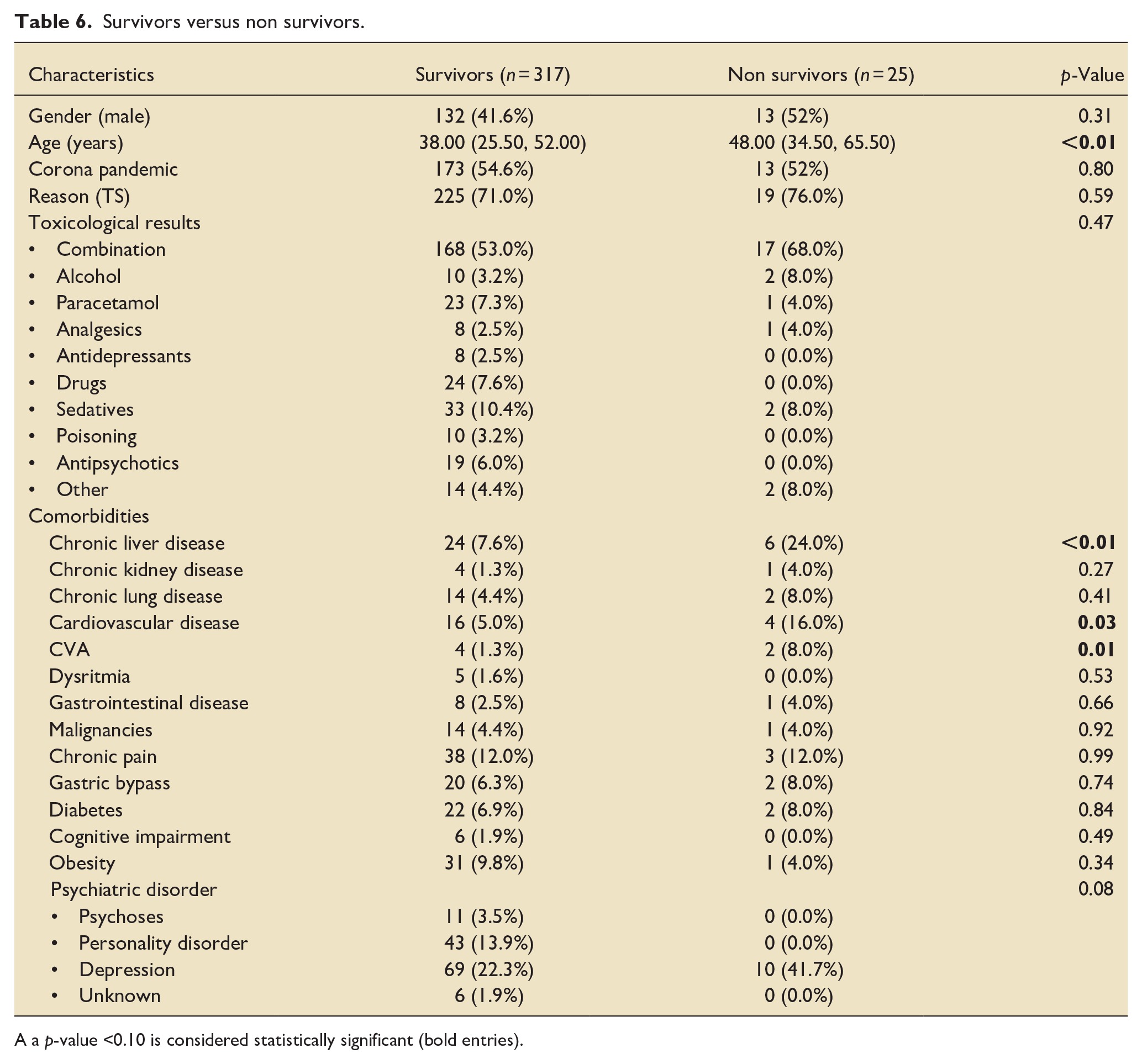
A a p-value <0.10 is considered statistically significant (bold entries).
Univariate analysis of risk factors for mortality is presented in Supplemental Table 3 showing that a higher age, the presence of a chronic liver disease, a CVA, and chronic cardiovascular disease are associated with higher mortality. Supplemental Table 4 presents the multivariate analyses showing no significant differences.
Discussion
To our knowledge, this is the first cohort study performed to date, assessing the impact of auto-intoxication on ICU resource utilization and identifying the characteristics and outcomes of these patients in a Belgian context. In our center, a large district hospital with tertiary referral function, 2.66% of all ICU admissions were attributable to auto-intoxication and this percentage remained stable over the years.
Literature has shown that auto-intoxication may account for 3.4% to 17.3% of all ICU admissions, with the majority of studies reporting rates between 3% and 6%.6,14 –17 Hence, the observed ICU admission rate in the present study is slightly lower than expected. A possible explanation might be the higher threshold for ICU-admission after auto-intoxication in our hospital, since ICU-occupancy was mostly over 80% in that time-period, with the inherent problem of a shortage of ICU-beds. However, median SOFA scores and APACHE IV-scores in our patient population are comparable with those reported in a previous large study. 15
The annual prevalence of ICU admissions due to auto-intoxication remained stable over the years in our center. Hence, the Covid-19 pandemic seemed not to have contributed to an increase in ICU admission rates. Other studies have reported comparable findings: McCluskey et al. 18 showed a stable admission rate to the pediatric intensive care unit for adolescents (12–18 years) after a suicide-attempt. Also, data on the national rate of suicide and suicide attempts during the pandemic, regardless the need for ICU admission, showed no impact on the prevalence as compared to years before the Covid-19 pandemic. 19 This is rather surprising in view of the pandemic’s detrimental impact on mental illness, social disadvantage and reported increased alcohol abuse. 11 In contrast, different studies executed prior to the onset of the Covid-19 pandemic, did show an increase in suicide attempts and auto-intoxication: Kasemy et al. 20 observed an incremental rise in suicide attempts across time in Egypt during a 4-year period (just prior to the Covid-19 pandemic), predominantly in the younger aged (<25 years). These findings were confirmed by various American studies: between 2000 and 2010, Baker et al. 21 reported a 16% increase in suicides (including auto-intoxications), whereas Spiller et al., 22 found an increase in suicide-attempts by auto-intoxication specifically in adolescents and young adults in the period between 2000 and 2018. As an explanation for this observed rise in suicide attempts, mainly economic reasons were mentioned, 21 which is confirmed to be an important risk factor for suicide attempt in a more recent study. 23 Other factors, contributing to this observed increase in suicide attempts are of a psychosocial and technological nature.24,25 Also, society-shifting changes (including the advent of social media and smartphones) are mentioned as a probable etiology in the younger age category. 22 However, data comparing the prevalence of suicide attempts and auto-intoxication as well as their underlying causes before, during and after the Covid-19 pandemic are currently lacking. It is therefore difficult to certify why the etiologies mentioned above did not seem to apply to our data. We presume that differences in cultural and socio-economical aspects might play a role. Hence, data from other countries or continents cannot automatically be applicated to other settings because of these important socio-economic discrepancies between continents, countries and even between cities and regions. Moreover, the highly accessible health care system in Belgium – even during the Covid-19 pandemic – might have been a protective factor, although we have no firm data to support this statement.
Another primary goal of this study was to examine characteristics and outcomes of patients admitted to the ICU due to auto-intoxication. The characteristics (age, gender, BMI and laboratory values at presentation) of our study population are highly comparable to those mentioned in other observational trials. Females were slightly overrepresented in this patient cohort and age distribution was rather constant. Certainly, the higher female/male ratio is a recurring phenomenon as most cohorts display this distribution in previous studies examining self-poisoning.3,6,15,20,22 This trend is also present when looking into the national data on suicide attempts, 19 as well as compared to international data on sex distribution.26,27
In terms of age distribution, young adults between 18 and 29 years old comprise the largest majority in our cohort. Kristinsson et al. 3 reported a comparable age distribution concerning acute poisonings in Iceland and a reported median age around 41 years old at admission to ICU due to intoxication in the United States, is also similar to our findings. 15 Furthermore, if we mirror our results of age distribution and median age to general suicide attempts in Flanders, Belgium; again there is no difference in results. 19
Suicide attempt by self-poisoning and (recreational) drug abuse were the two major causes of auto-intoxication in our patient cohort, accounting for more than 90% of cases. Recidivism was noted in almost 40% of included patients and a previous history of suicide attempt was present in more than 20% of patients. A psychiatric disorder was diagnosed in half of the patients, alcoholism in more than 20% of patients and chronic pain in more than 10% of patients. In line with our results on recidivism, it has been consistently demonstrated that patients with a history of suicide attempt are at higher risk to reattempt.3,28–32
Almost a quarter of the admitted patients in our cohort was known with depression, and over 40% with a psychiatric disorder (Table 2). Emotional (30.9%), relational (17.4%), and psychological (12.2%) problems are the most common precipitating factors indicated by the patients for self-poisoning in our results (Table 3).
In the present study, treatment comprised administration of activated charcoal in 30%, an antidote in one-third of patients, mechanical ventilation in 25%, antibiotics in 15%, vasopressors or inotropic agents in 12% and hemodialysis in less than 1% of patients. Notably, in 30% of patients, treatment was only observational of nature. The rather rare need of invasive measures in this study is also reflected in a short ICU (1 day) and hospital (3 days) length of stay. Consistent with our results, small and large scale studies also observed this rare need for invasive measures and a short length of stay.3,6,15,33 In 2016, Brandenburg et al. 5 developed a model that predicts the need of ICU treatment (receiving mechanical ventilation and/or vasopressors) in intoxicated patients. They concluded that clinical use of the prediction model, with a high negative predictive value (98.7%), would result in 34.3% less observational admissions. 5 Our results also suggest that implementation of this model in our hospital has the potential to safely reduce the number of ICU admissions, resulting in a cost reduction due to intoxication of almost one-third.
In this study, the ICU mortality rate was only 1.75%, and in-hospital mortality rate was 2.60%. These results are well in line with mortality rates in comparable studies.1,3,15,33,34
The reason for low hospital mortality rates, as well as the rare need for invasive measures and short length of stay, is found in the relatively young age and absence of somatic co-morbidities in most patients. They usually present with an acute event with well-known pathophysiology and clinical course. Rezar et al. 15 compared the patient population admitted to the ICU with intoxication versus other diagnoses and also concluded the intoxication-patient group to be “less ill.”
Total mortality 1 year after dataset closure was much higher (7.30%) and in line with higher reported long-term mortality rates in other studies.1,34,35 Nonetheless, all patients in our study received psychiatric follow-up started before being discharged from the ICU. An ICU-admission because of auto-intoxication can therefore be interpreted as a warning sign for mortality in the future. Brandenburg et al. 5 therefore advices that an individual plan and follow-up for each patient leaving the ICU and hospital after auto-intoxication could be cost-efficient both for the hospital and health care in general.
We observed no significant difference in mortality between sexes. Although women have a higher risk to commit a suicide-attempt, males are known to have a higher risk of dying after a suicide-attempt.19,36 Higher mortality rates are also reported in older patients committing suicide in Belgium 19 in line with our findings that older age associated with higher mortality. However, the association between higher age and mortality is not confirmed by Rezar et al. 15 in a larger cohort group in the United States. Our results further suggest that severe co-morbidities for example, chronic liver disease, cardiovascular disease and CVA are significantly correlated with higher mortality. This association between severe co-morbidities and mortality is not surprising since those co-morbidities indicate a higher level of frailty, also associated with a higher mortality risk.
In over 50% of the cases, auto-intoxication comprised a combination of substances. The clinical presentation or toxidromes can therefore be mimicked by the co-ingestion of different substances. Hence, one should always stay critical toward a patient’s presentation as well as (hetero)anamnestic information. Abuse of sedatives was noted in almost 50% of cases. Analgesic (like opioids) and antidepressant abuse were noted in 17.8% and 16.7%, respectively. This observation is not surprising, since abuse of opioids and sedatives in Belgium is very high.7 –9 A recent systematic review of self-poisoning suicidal deaths by countries, also found that in Western or industrialized countries, use of illicit drugs (mainly opioids) and medically prescribed psychoactive medications are the leading cause of suicide by self-poisoning. 37 In the United States, data also show that men are more likely than women to use illicit drugs, and to present to the emergency department with overdose as well as death from overdose. 27
The main limitation of this study consist in its retrospective, observational and monocentric set-up. Therefore, the sample size is relatively small and regional variations in the use of different substances, needing different ICU resources cannot be excluded. As a result, the findings of our study may not be representable for other Belgian centers nor are they automatically extrapolable to other countries or regions. Secondly, since we did not perform a cost-analysis of auto-intoxication necessitating ICU admission, the economic impact of this specific patient cohort for the hospital nor for the Belgian healthcare system could be measured. Although, recent studies have shown that the costs of intoxicated ICU patients are significantly higher than non-intoxicated ICU patients,6,38 but whether these findings are applicable to our setting remains unclear.
In conclusion, the prevalence of ICU-admitted auto-intoxicated patients remained stable over the 5-year study period and an impact of the Covid-19 pandemic could not be established. ICU- and in-hospital mortality after auto-intoxication is low, although these patients have a substantial risk for death in years to come after hospital discharge. A cost-analysis of this specific cohort of ICU patients could be useful to identify the economic burden for an individual hospital and for the Belgian healthcare system.
Supplemental Material
sj-docx-1-inc-10.1177_17511437241311102 – Supplemental material for Characteristics and outcomes of auto-intoxicated patients admitted to the ICU: A retrospective cohort study
Supplemental material, sj-docx-1-inc-10.1177_17511437241311102 for Characteristics and outcomes of auto-intoxicated patients admitted to the ICU: A retrospective cohort study by Lotte Van Nylen, Sander Swennen, Ina Callebaut, Laurien Geebelen, Jasperina Dubois, Jeroen Herbots, Marijke Nulens, Jeroen Vandenbrande, Michiel Vantornout and Björn Stessel in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.