
Abstract
In 28 patients supported by an Impella pump (Impella CP, Abiomed Inc.®, Danvers, MA), hemodynamic measurements by PiCCO (PULSION Medical Systems SE®, Feldkirchen, Germany) and pulmonary artery catheter (PAC or Swan-Ganz Catheter; Edwards Lifescience®, Unterschleissheim, Germany) were compared. There was a significant positive correlation of cardiac output (CO; r2 = 0.917, p < 0.001), systemic vascular resistance index (SVRI; r2 = 0.904, p < 0.001), stroke volume index (SI; r2 = 0.909, p < 0.001) and left ventricular work index (LCWI; r2 = 0.689, p < 0.001) in PiCCO and PAC measurements under Impella CP support. We conclude, that in patients with left-ventricular Impella support, hemodynamics may be assessentd by PiCCO or PAC.
Introduction
Immediate revascularization has been shown to improve survival 1 ; however, mortality in patients with acute myocardial infarction complicated by cardiogenic shock (AMICS) remains high. 2 Mechanical support systems like percutaneous left ventricular assist devices and extracorporeal membrane oxygenation (ECMO) are now widely used. 3 The Impella CP, a catheter-based device inserted through the femoral artery into the left ventricle, provides up to 4.3 l/min of support. By unloading the left ventricle, it reduces wall stress and enhances coronary blood flow. The use of a pulmonary artery catheter (PAC or Swan-Ganz Catheter; Edwards Lifescience®) in patients supported by an Impella pump has been associated with improved survival. 3
Advanced hemodynamic monitoring with the PAC and pulse contour cardiac output (PiCCO; PULSION Medical Systems SE®) systems has been extensively compared, showing high agreement. In the PiCCO system, the Impella is positioned between the central venous catheter and the femoral arterial catheter with a thermistor-tip. In contrast, PAC measurements occur in the pulmonary artery, before the indicator passes through the pump.
We aimed to investigate potential differences in hemodynamic parameters measured by PiCCO and PAC in patients treated with an Impella CP due to cardiogenic shock.
Patients and methods
In patients with shock, initial hemodynamic parameters were assessed using the PiCCO system. After Impella pump implantation, a PAC was inserted to monitor pulmonary capillary wedge pressure (PCWP). From January 2014 to July 2016, we analyzed hemodynamic data from PiCCO (PULSION Medical Systems®) and PAC (Edwards Lifesciences®) in 28 patients supported by the Impella CP device (Abiomed®) at the University Hospitals of Würzburg and Brandenburg, Germany. All patients were mechanically ventilated and received norepinephrine; dobutamine was used in 24, and levosimendan or enoximone in 7 and 4, respectively. Seven patients received continuous renal replacement therapy (PrismaFlex, Gambro®).
Cardiogenic shock was defined as systolic blood pressure < 90 mmHg or vasopressor use to maintain systolic blood pressure ⩾ 90 mmHg, with signs of reduced organ perfusion, heart rate > 60, PCWP ⩾ 15 mmHg, or cardiac index ⩽ 2.2 l/min/m².
The study was approved by the local ethics committee (Würzburg University Hospital, 2018090301). Data are presented as mean ± standard error of the mean (SE) or as median and range. Group comparisons were made using t-tests, Mann-Whitney U, or chi-square tests. Intra-class correlation was calculated, and p-values <0.05 were considered significant. Statistical analyses were performed using R version 3.0.2 (The R Foundation).
Results
Over a 24-month period, 28 patients (11 women, 17 men) were studied. Patient characteristics are listed in Table 1. A total of 26 measurements were obtained with the PAC and PiCCO systems. Central venous pressure was 12.67 ± 3 mmHg and pulmonary capillary wedge pressure was 19.7 ± 8.5 mmHg. The Impella pump had supported with 3.0[1.3 – 3.5] l/min. Eleven patients died during their ICU stay.
Patient characteristics.
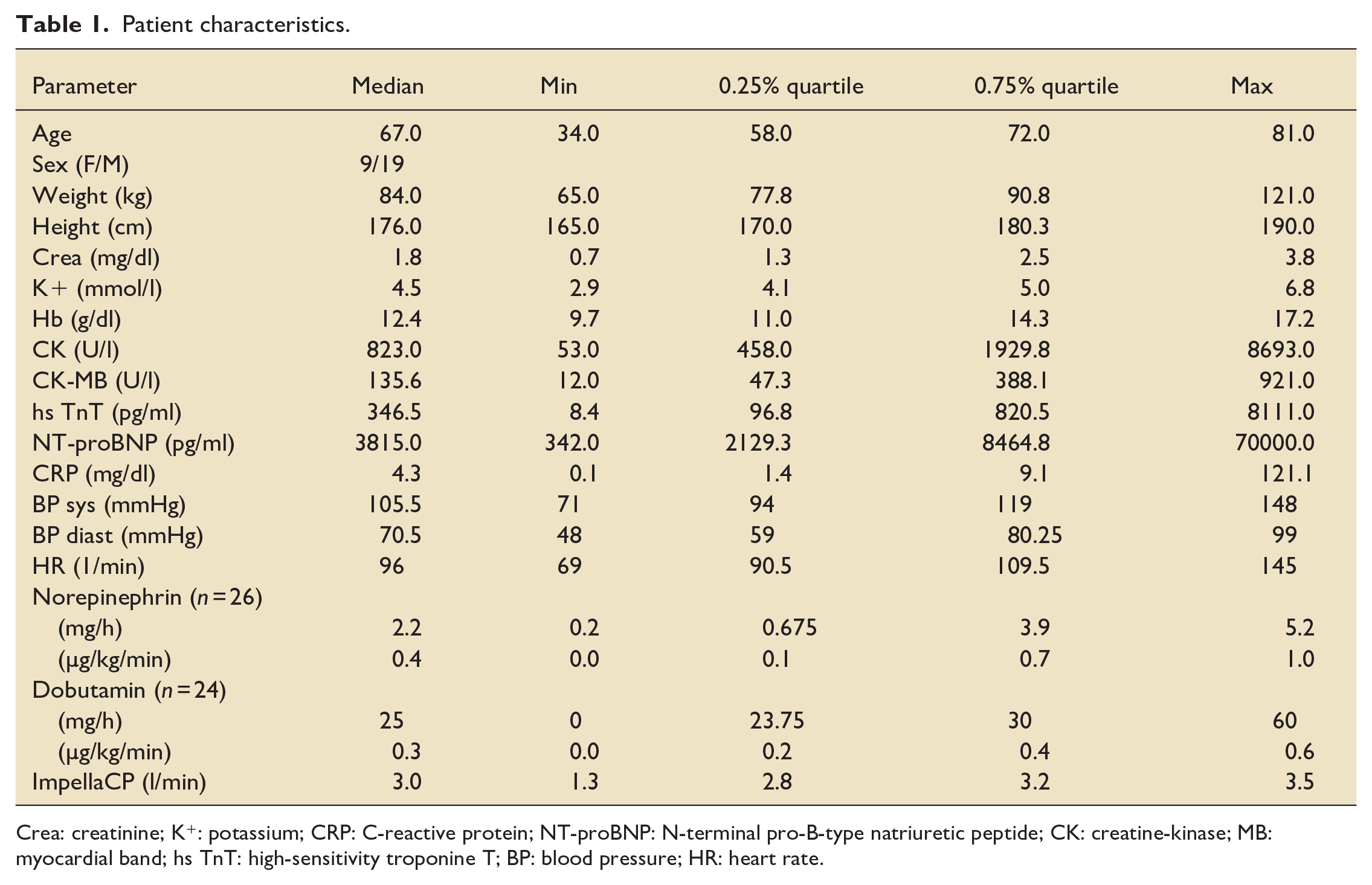
Crea: creatinine; K+: potassium; CRP: C-reactive protein; NT-proBNP: N-terminal pro-B-type natriuretic peptide; CK: creatine-kinase; MB: myocardial band; hs TnT: high-sensitivity troponine T; BP: blood pressure; HR: heart rate.
Parameters assessed by both methods are shown in Figure 1. The intraclass correlation of the pairs are as follows: cardiac output (CO) 0.882 (p-value < 0.001, 95%-CI 0.737–0.949), stroke volume index (SI) 0.929 (p-value < 0.001, 95%-CI 0.833–0.971), systemic vascular resistance index (SVRI) 0.679 (p-value < 0.001, 95%-CI 0.37–0.853), and left ventricular work index (LCWI) 0.684 (p-value < 0.001, 95%-CI 0.377–0.855).
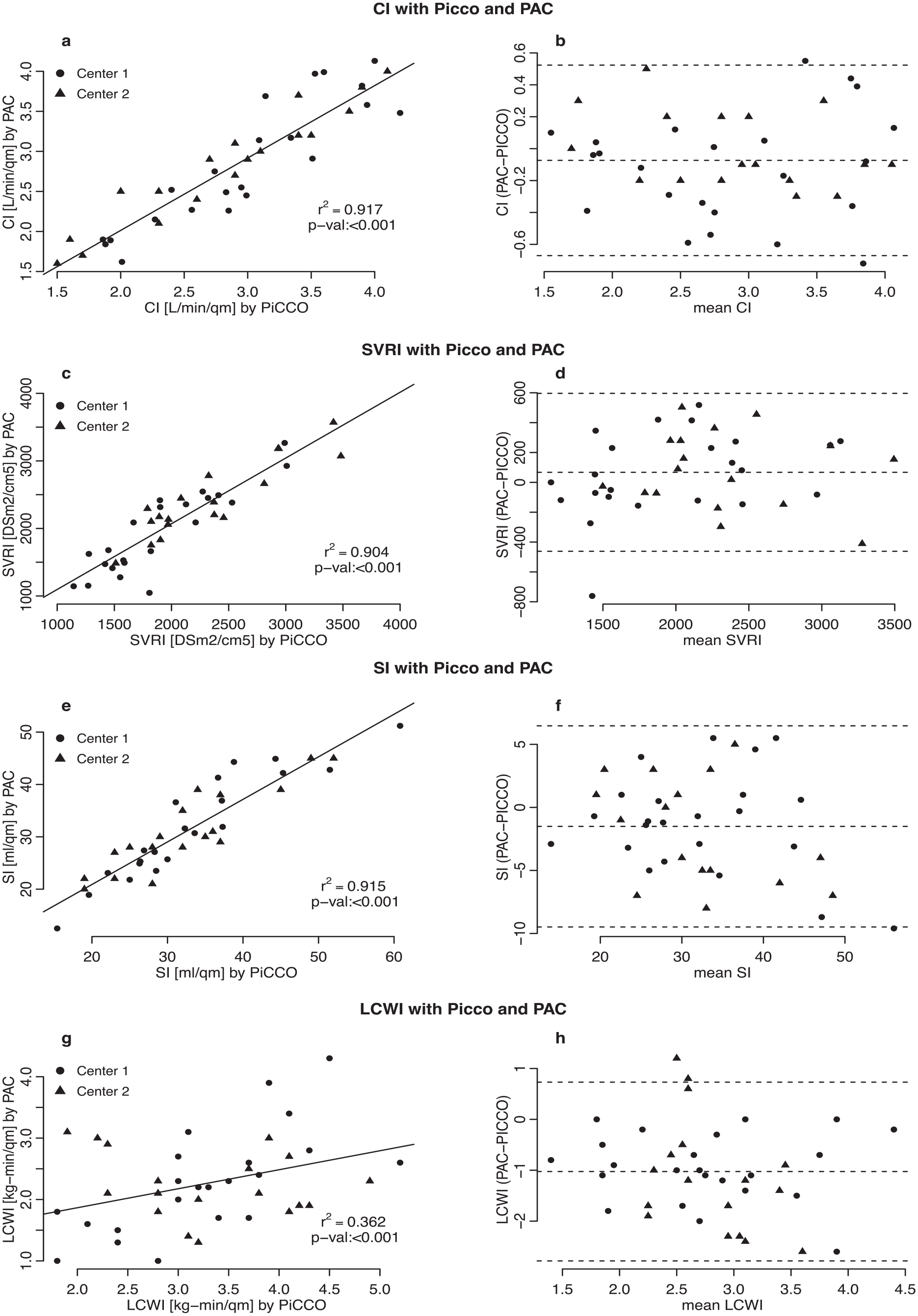
Comparison of cardiac index (CI), systemic vascular resistance index (SVRI), stroke volume index (SI), and left ventricular work index (LCWI) measured by PiCCO and PAC. Method comparison for cardiac index (a, b), systemic vascular resistance index (c, d), stroke volume index (e, f), and left ventricular work index (g, h) measured by thermodilution assessed by PiCCO and PAC. (a), (c), (e), and (g) show the regression analysis between both methods, (b), (d), (f), and (h) show Bland-Altman difference plots using the % difference between the two methods.
Discussion
In this study, we compared hemodynamic monitoring using PiCCO and PAC measurements in patients with cardiogenic shock supported by Impella CP. We found a significant positive correlation between the two methods.
In PAC, cooled saline is injected into the right atrium or superior vena cava, with the temperature drop measured in the pulmonary artery. In the PiCCO system, saline is injected via central venous catheters and measured at a distal arterial line after transpulmonary passage. Both methods rely on thermodilution, assuming constant volume and temperature, immediate injection, complete mixing, and representative sampling. 4
Neither PAC nor PiCCO has been proven superior,5,6 and advanced hemodynamic assessment has not shown reduced mortality. 7 However, we demonstrated that PiCCO measurements are comparable to PAC values in patients with compromised hemodynamics under Impella.
This study’s limitations include its observational design, lack of impact analysis on clinical outcomes, and no comparison with echocardiography.
In conclusion, PiCCO-derived parameters closely align with PAC in Impella-supported patients, offering a promising alternative for hemodynamic management.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.