
Abstract
There are no guidelines for assessing and communicating the expected difficulty of a tracheostomy, leading to difficulties planning a percutaneous approach in intensive care or referring onwards to surgical teams. A Delphi process was used to develop a tool containing metrics which are relevant for either specialty and can be universally assessed by both. Palpable tracheal rings, prior surgery or radiotherapy to the anterior neck, uncorrectable clotting or platelet dysfunction, ability to extend the neck freely, and overlying vessels visible, palpable or on imaging were all found to be relevant. It is hoped this tool will aid communication between specialties.
Introduction
Two thirds of tracheostomy procedures are performed by intensive-care specialists; 90% percutaneously.1,2 The remaining third are discussed with surgical teams. There are no guidelines for what warrants discussion.1 –4 The authors have developed a tool to assess patients to a common standard, communicate the expected difficulty of a tracheostomy, and collectively plan the most appropriate approach, setting and requirements.
Methods
A live Delphi method was used to develop metrics that were relevant to procedural difficulty and universal to assess and communicate.5,6 Expert interviews were conducted by the author to explore the scope and generate ideas for metrics. A working group undertook a round of structured discussions to validate the scope and refine nine possible metrics to the most relevant six. An online iterative process invited six intensivists and anaesthetists and seven ENT surgeons from three hospitals to rate each metric from +++ to −−− on a seven-point Likert scale and engage in free-text discussion using eDelphi (metodix, Helsinki) software. Following their initial rating they were shown anonymised group results and could adjust their own rating. The intensive care and anaesthetics consultants were members of their respective airway specialty groups and the ENT consultants were head and neck or benign airway subspecialists. A metric was taken forward if 70% of surgeons or anaesthetist-intensivists rated it as +++ or ++ relevant. An interquartile range (IQR) of a quarter of +++ (+3) to −−− (−3) (numerically 1.5) was regarded as inter-rater agreement. Likert scales with these thresholds have been recommended by systematic reviews of similar projects.5,7,8 Syntax and content analysis measured engagement levels and therefore degree of quality. 5
Results and discussion
Relevance
The five metrics considered relevant to either ENT surgeons or anaesthetist-intensivists and therefore taken forward in this study were: palpable tracheal rings, prior surgery or radiotherapy to the anterior neck, uncorrectable clotting or platelet dysfunction, ability to extend the neck freely, and overlying vessels visible, palpable or on imaging (Figure 1). The Faculty of Intensive Care Medicine guidelines states the first three increase difficulty or warrant discussion with the surgical team. 1 A fourth – overlying vessels – could be inferred from their statement ‘high risk of bleeding’ but is not explicitly stated. 1 Two metrics are considered contraindications to a percutaneous approach in a key head & neck surgery text: prior surgery or radiotherapy to anterior neck, and uncorrectable clotting or platelet dysfunction. 3 A third – palpable tracheal rings – captures two of their suggested difficulty factors: ‘thick neck’ and ‘enlarged thyroid’. 3
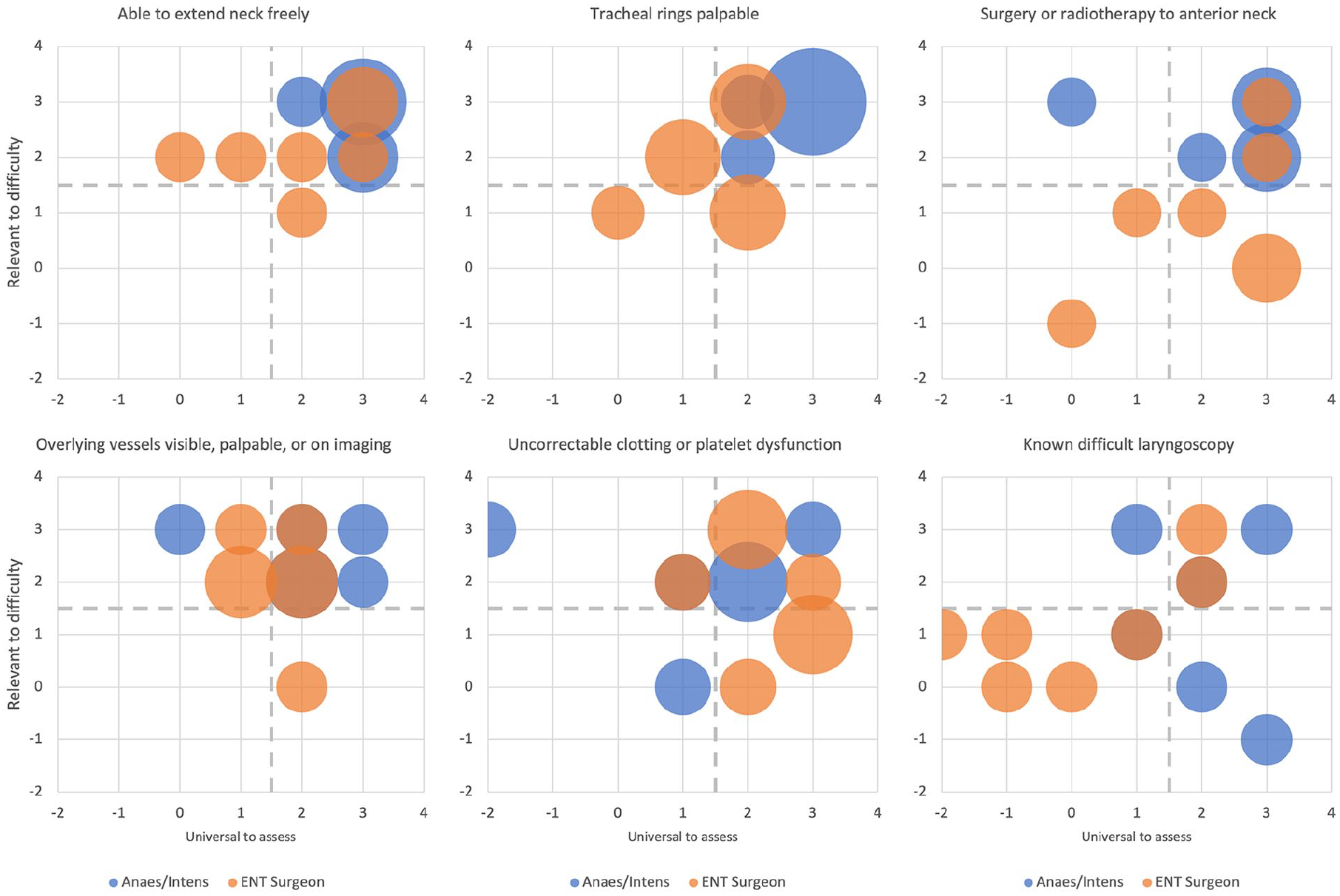
Cluster chart of all responses to metrics plotted by relevance to difficulty versus universal to assess. Bubble size represents number of respondents.
The surgical and intensive care literature both advise placing the neck in extension but neither state this metric would alter the difficulty.1,3 This was the most relevant and universal factor highlighted in this study. The five metrics taken forward in this round of the study therefore capture the four factors in the intensive care and head & neck surgery literature as well as an additional factor deemed the most relevant from clinician expertise. The sixth metric known difficult laryngoscopy was not taken forward.
Universality
The three metrics considered universal to assess by both surgeons and anaesthetist-intensivists were: ability to extend neck freely, palpable tracheal rings, and surgery or radiotherapy to anterior neck (Figure 1). Overlying vessels visible, palpable or on imaging was considered universal by anaesthetist-intensivists, which they commented was due to widespread use of bedside ultrasound. Surgeons did not consider this universal, perhaps because they palpate rather than use ultrasound, or because surgical texts do not teach it.3,4 Uncorrectable clotting or platelet dysfunction was considered universal by surgeons; however not anaesthetist-intensivists. Dissenters commented that without numerical cut-offs it would remain non-universal; however the working group considered a cut-off would create unnecessary disagreement between specialities which would distract from the purpose of the tool.
To further increase universality, the working group agreed to develop an inventory-type assessment tool, rather than a grading of severity. In use therefore, the tool is five metrics where an abnormal finding in any metric should prompt an interdisciplinary discussion, using the finding in each metric to structure the discussion.
Similar tools for predicting difficult intubation have had mixed results due to low predictive value and not affecting clinical choices. 9 By comparison these metrics were selected because they predict a procedural difficulty that would alter the approach, team or setting.
Performing a percutaneous tracheostomy is the highest-risk elective procedure performed by intensivists. The percutaneous technique provides fewer tools for dealing with unexpected difficulties than surgical teams have in theatre. 1 This project identifies areas of shared concern, as well as specifying metrics to enable teams to assess, discuss and plan for these risks in advance (Table 1).
Percentage agreement (+++ or ++) with metrics by stakeholder subgroup.
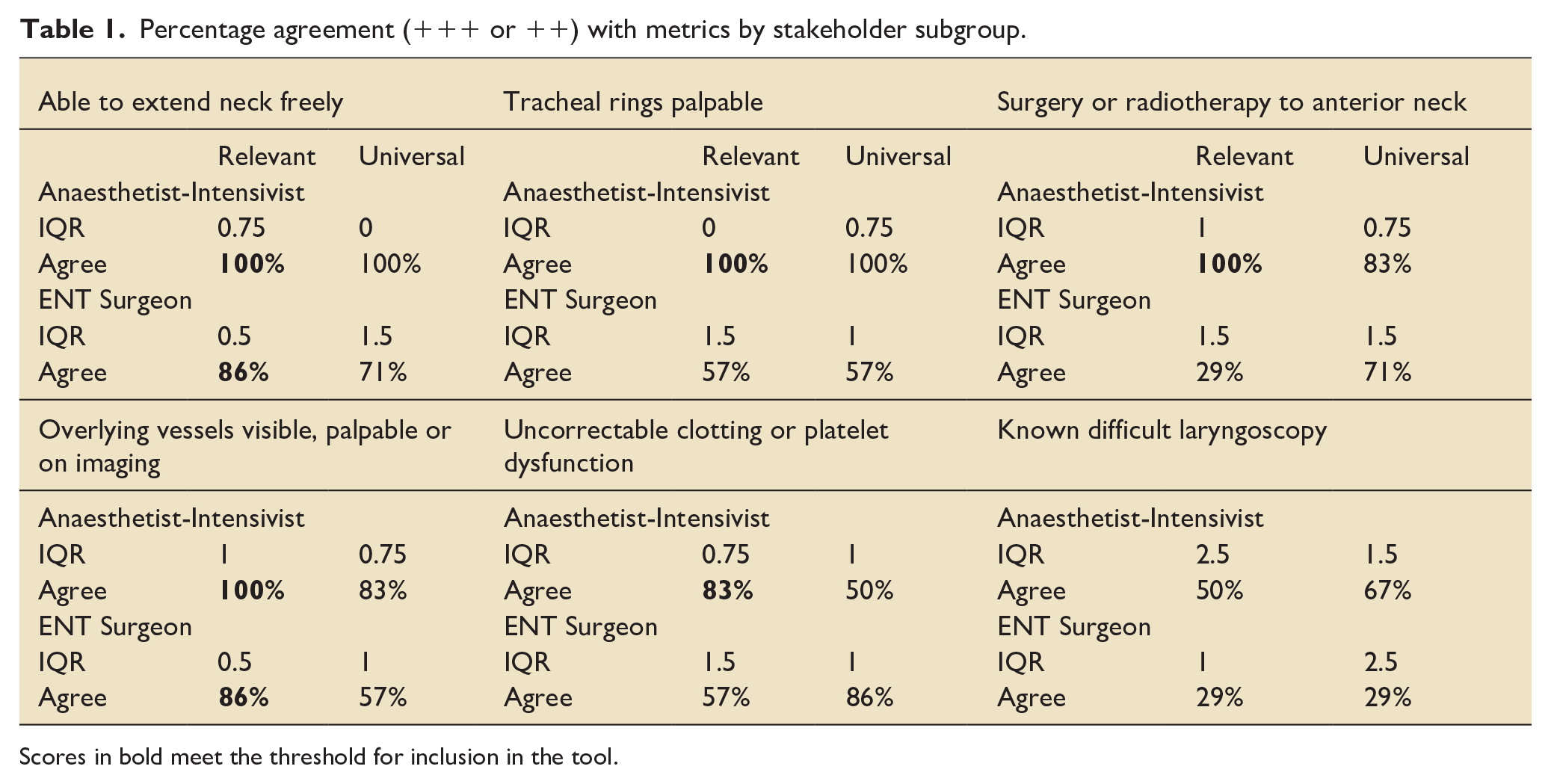
Scores in bold meet the threshold for inclusion in the tool.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.