
Abstract
Objective
Patients undergoing tracheostomy represent a unique cohort, as often they have prolonged hospital stay, require multi-disciplinary, resource-intensive care, and may have poor outcomes. Currently, there is a lack of data around overall healthcare cost for these patients and their outcomes in terms of morbidity and mortality. The objective of the study was to estimate healthcare costs and outcomes associated in tracheostomy patients at a tertiary level hospital in South Australia.
Design
Retrospective review of prospectively collected data in patients who underwent tracheostomy between July 2009 and May 2015.
Methods
Overall healthcare-associated costs, length of mechanical ventilation, length of intensive care unit stay, and mortality rates were assessed.
Results
A total of 454 patients with tracheostomies were examined. Majority of the tracheostomies (n = 386 (85%)) were performed in intensive care unit patients, predominantly using bedside percutaneous approach (85%). The median length of hospital stay was 44 (29–63) days and the in-hospital mortality rate was 20%. Overall total cost of managing a patient with tracheostomy was median $192,184 (inter-quartile range $122560–$295553); mean 225,200 (range $5942–$1046675) Australian dollars. There were no statistically significant differences in any of the measured outcomes, including costs, between patients who underwent percutaneous versus surgical tracheostomy and patients who underwent early versus late tracheostomy in their intensive care unit stay. Factors that predicted (adjusted R2 = 0.53) the cost per patient were intensive care unit length of stay and hospital length of stay.
Conclusion
Hospitalised patients undergoing tracheostomy experience high morbidity and mortality and typically experience highly resource-intensive and costly healthcare.
Keywords
Introduction
Tracheostomy (first depicted on Egyptian artefacts in 3600 BC) 1 is an age-old surgical technique performed both for elective and emergency indications. Advances in medical practice have seen the procedure being performed more frequently, for a plethora of indications both medical and surgical. Also, the procedure is increasingly being performed by clinicians in non-surgical specialities such as intensive care. Consequently, most tertiary hospitals and increasingly primary healthcare services are being exposed to and engaged in the care of these patients.
The cohort of patients who undergo tracheostomy is complex and their care represents a unique challenge as it is prolonged, multi-disciplinary and consequently typically resource-intensive. 2 Some tracheostomy patients undergo laryngectomy (permanent tracheostomy), while some have temporary tracheostomy as a part of their head and neck cancer surgery. Most of these procedures are performed electively and the patient is then admitted to intensive care unit (ICU) in the post-operative period to undergo mechanical ventilation for a short duration. However, in practice the majority of patients who undergo tracheostomy are ICU patients (both medical and surgical patients) who are unable to be weaned off the invasive ventilation and undergo tracheostomy to facilitate this process (achieved by interruption of sedation and intermittent trials of spontaneous unassisted breathing). These patients undergo either a bedside percutaneous tracheostomy or a surgical tracheostomy in the operating theatre. 3 After separation from the mechanical ventilator, they transition to the hospital ward (some of them with a tracheostomy) and undergo prolonged rehabilitation including speech and swallow therapies, besides recovering from the original condition which resulted in ICU admission in the first place. For these reasons, modern management of these patients is multi-disciplinary, involving medical and surgical specialities and other allied teams such as physiotherapy, speech and swallow therapy, and rehabilitation.4–6
Despite these resource-intensive efforts to improve quality and outcome, the morbidity and mortality experienced by this cohort of patients can be significant.7,8 They frequently have a prolonged ICU stay including time on the mechanical ventilator, associated neuromuscular disability, physical and cognitive deconditioning, and sometimes end-of-life issues.9,10 Also, they usually have multiple other comorbidities and undergo multiple other procedures in hospital. Due to prolonged exposure to invasive devices and the hospital environment, being bed bound and with compromised immune system, these patients frequently develop healthcare-associated complications such as nosocomial infections, tracheal strictures and fistula, and pressure injuries. 11
Despite the above concerns around likelihood of poor outcomes and resource-intensive care in this cohort of patients who undergo tracheostomy, there is a lack of clear evidence around overall cost of healthcare for these patients and their outcomes in terms of morbidity and mortality. Particularly so, in the context of the Australian healthcare setting, which maybe different in terms of care, patient demographics, and team structure, as compared to other healthcare delivery settings such as the United States. 12 The existing literature around costs has only focussed on the procedure itself, rather than the total costs associated with the healthcare pathways experienced by this unique group of patients. Procedural costs may be negligible when total costs are considered, and from a health-system perspective, the latter is more relevant. Information relating to the cost of healthcare pathways and hospital episodes assists in many types of policy decisions including allocation of resources to facilities and services, 13 introduction or setting user fees, 14 assessment of the comparative efficiency of healthcare services across settings,15,16 and the determination of health service budgets.
We hypothesised that this cohort of patients who undergo tracheostomy receive healthcare, which has high resource and cost implications, and experience poor outcomes in terms of mortality and morbidity. In this study, we aimed to review all the patients who underwent tracheostomy in a tertiary level hospital in South Australia over a six-year time period, to estimate the cost associated with their hospital care pathways and their outcomes.
Methods
We performed a retrospective review of prospectively collected data at a tertiary referral hospital – Flinders Medical Centre, South Australia. Our study protocol was approved by the institutional ethics Committee (Southern Adelaide Clinical Human Research Ethics Committee: 514/15). Patients who underwent tracheostomy between July 2009 and May 2015 inclusive were included. The year 2009 was selected for the commencement of the study as this marked the establishment of a high-quality database reflecting hospital care pathways, cost and outcomes.
Care model
Flinders Medical Centre is a tertiary level referral hospital with 32 ICU and 593 hospital beds. The tracheostomy procedure is performed either in ICU by Intensive care physicians or in the operating theatre by the speciality surgical team (ENT). The most common tracheostomy brands utilised for the procedure are Portex® (Smiths medical, USA) or Shiley™ (Coviden, USA). All tracheostomy patients transition through ICU during their stay in the hospital. On ICU discharge, the majority of patients are transferred to a high-dependency stepdown unit, before being transferred to general wards. The nurse-patient ratio for these patients is 1:1 in ICU, whereas it is 1:2 for high-dependency care patients and 1:4 in general wards. A hospital multi-disciplinary team (MDT) was formally established in June 2015 and since this period all patients undergoing tracheotomy are reviewed on weekly basis by a hospital MDT consisting of an ENT specialist, intensive care physician, nurse manager, speech therapist, and physiotherapist.
Data collection
A list of patients with tracheostomy placement during a hospital admission was extracted from the hospital administrative database. Records that contained International Statistical Classification of Diseases and Related Health Problems 10th Revision version 9 – Australian modified version (ICD10AM), procedure codes for percutaneous tracheostomy (4188000), surgical tracheostomy, temporary (4188100) and surgical tracheostomy, and permanent (4188101) were extracted for further analysis. Each recorded procedure was manually checked and the following information fields were extracted – unit record number, age, gender, number of hours on invasive mechanical ventilation, day of admission to ICU, ICD10 diagnoses, ICD10 procedures, length of stay (LOS) in ICU, LOS in hospital, and hospital mortality. Furthermore, data for each patient were manually cross-checked from the surgical database and the date of tracheostomy was recorded. These records were linked by a unique hospital unit record number to a hospital costing database, where the costs of the care pathway for each patient in hospital is collated and recorded. We examined the hospital costing database to identify tracheostomy patients as those having laryngectomy or permanent tracheostomy as a part of primary cancer/ neck surgeries, and those who underwent tracheostomy as a part of their ICU care. ICU patients undergoing tracheostomy were further examined by procedure: percutaneous procedure (at the bedside) versus surgical tracheostomy (in the operation theatre); and timing of procedure: early (≤10 days) and late (>10 days) after ICU admission. We chose a cut-off point of 10 days to define early and late tracheostomy to achieve consistency with the definitions adopted by a recent review article. 17
Costing process
The costing system used for the study allocates costs for hospital overheads, based on Australian Costing Standards. 18 All direct and indirect/overhead costs (including e.g. hospital and ward administration, heating, lighting, cleaning) were collected and assigned to the relevant patient-care areas (such as ICU, ward based on appropriate Australian patient costing standards). These costs were then allocated across all patients in the study based on the time that was spent by each patient in the relevant patient care areas or wards. Similarly, the costs associated with clinician, nursing, and other healthcare professionals were allocated based on the time period for which the patient was admitted under the relevant clinical unit. Patient-level cost data relating to treatments and investigations were calculated by tracing the resources actually used by each patient during their hospital journey and their associated costs, e.g. imaging services, surgical procedures, allied health interventions, medications, pathology tests, prosthetics, and other high-cost consumables. The costings were done for a single hospital separation and in patients with hospital stays extending over one financial year, who had more than one costing record (for each financial year); the total costs associated with the hospital care pathways experienced by each patient are presented in the results.
Statistical analysis
Statistical analyses were performed using PASW 24.0 software (SPSS Inc, Chicago, IL). Data were tested for normality and normalised by log transformation where necessary. Data is reported as median (inter-quartile range, IQR), range, or as percentage. Data variables were compared using either independent sample t test, Mann–Whitney U test, or chi square test, depending upon the distribution. Factors predicting the cost of tracheostomy were further investigated by multivariate regression analysis where total costs for each patient was included as the dependant variable and age, severity of illness at ICU admission, Charlson co-morbidity index, number of procedures performed during their stay, number of diagnosis made during their stay, length of mechanical ventilation, day of tracheostomy, type of tracheostomy, ICU and hospital LOS were included as independent variables. A conventional two-tailed alpha level of <0.05 was used for all statistical significance testing.
Results
Characteristics of tracheostomy patients in the study (n = 454).
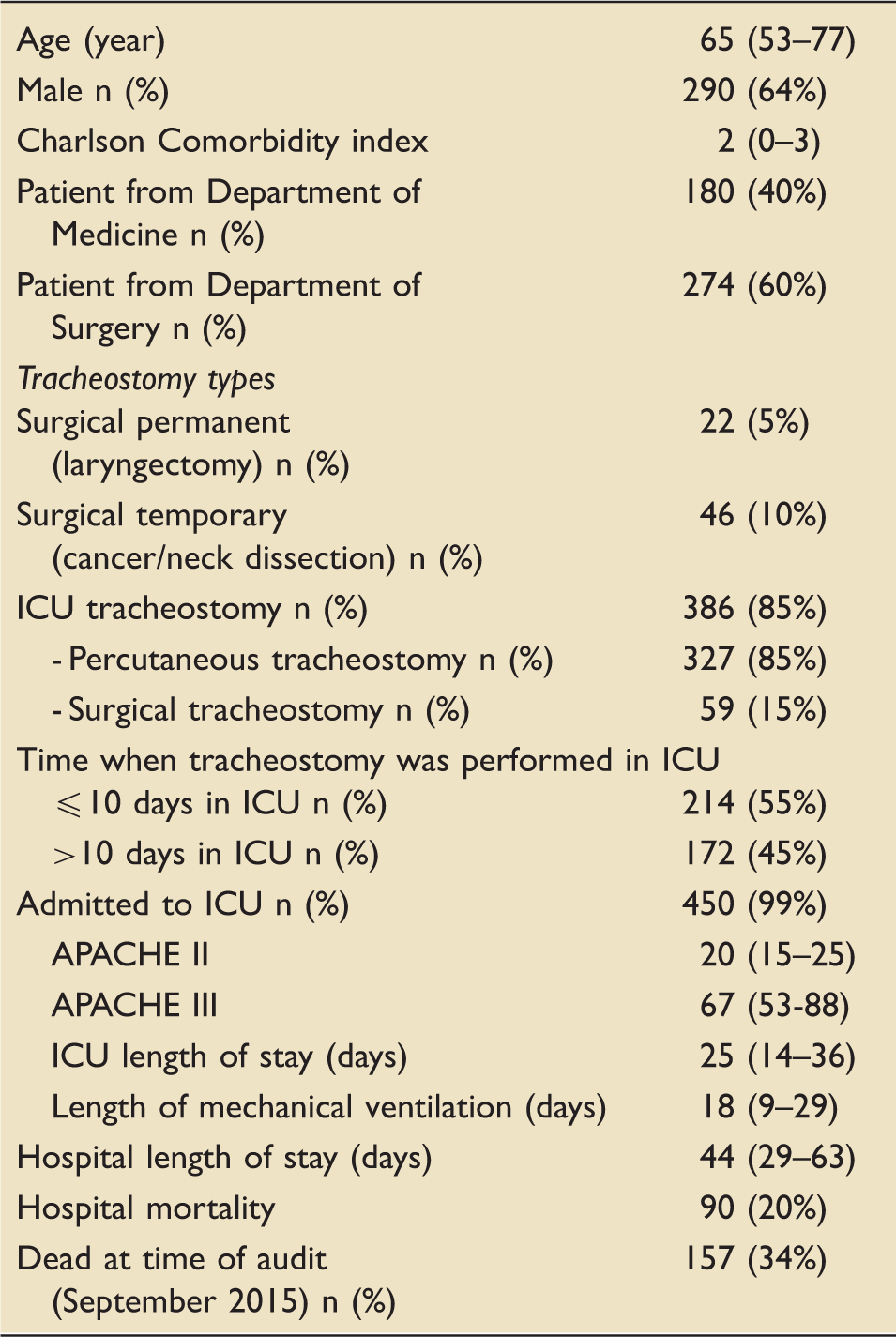
ICU: intensive care unit; APACHE: Acute Physiology and Chronic Health Evaluation.
Data represented as median (inter-quartile range).
The vast majority of the tracheostomies (n = 386 (85%)) were performed on patients in ICU, mostly to facilitate weaning from invasive ventilation. The remainder were either permanent (laryngectomy) or temporary tracheostomies performed in patients as a part of primary cancer management and/or neck surgery (Table 1). Of the tracheostomies in ICU patients, the majority were performed using the percutaneous technique at the bedside (85%).
The median length of hospital stay was 44 (29–63) days and the in-hospital mortality rate was 20%. The median total cost of managing a patient with tracheostomy was $192,184 (IQR $122560–$295553); mean 225,200 (range $ 5942–$ 1046675) Australian dollars. The median number of ICD10 diagnoses and procedures allocated for this cohort of patients were 16 (10–21) and 14, (11–18), respectively, during their stay in the hospital.
Surgical permanent (laryngectomy) patients (n = 22) and surgical temporary (cancer/neck dissection) patients (n = 46).
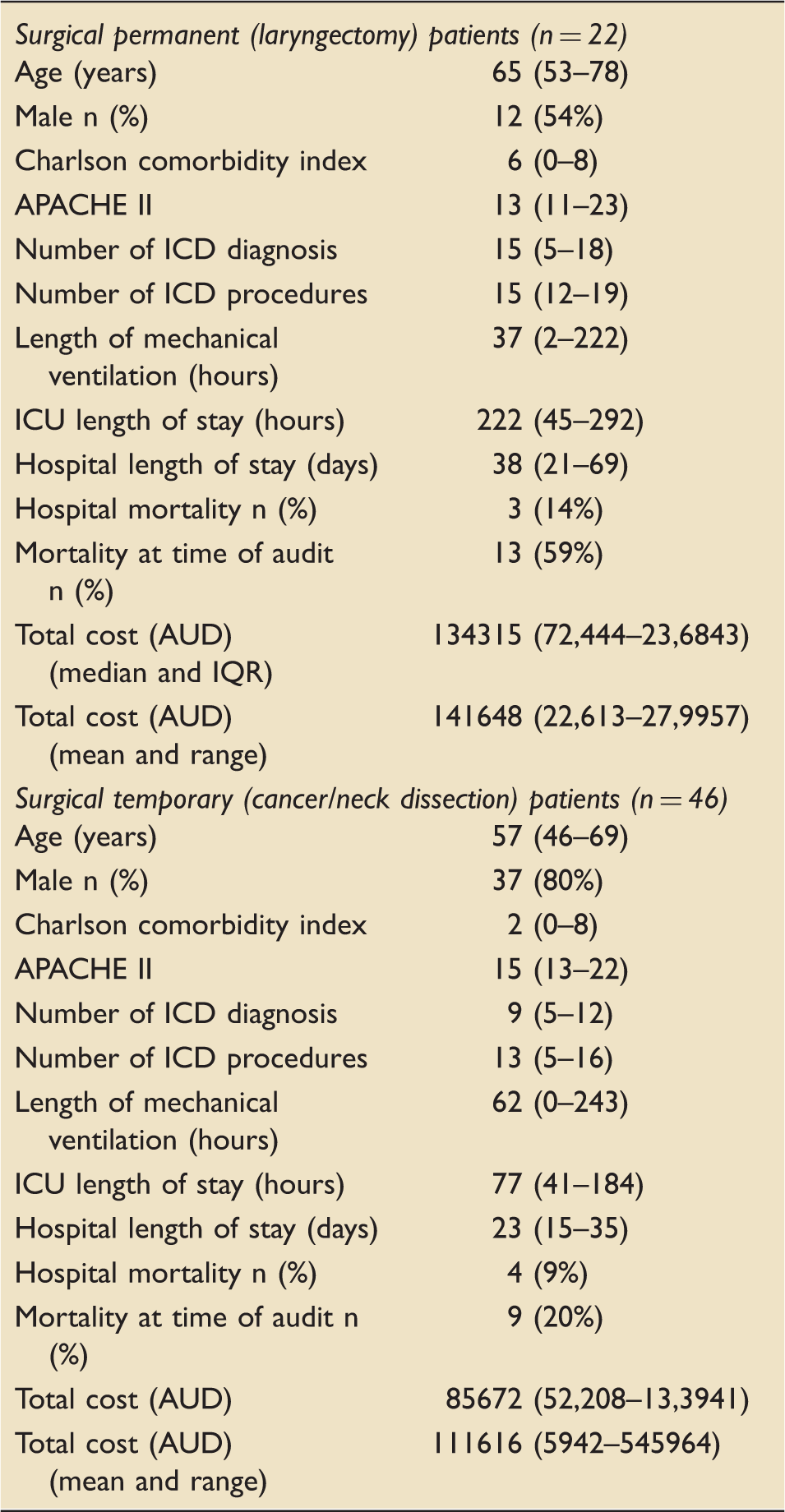
ICU: intensive care unit; APACHE: Acute Physiology and Chronic Health Evaluation.
Data represented as median (inter-quartile range), unless specified.
ICU tracheostomy patients examined: percutaneous and surgical group.
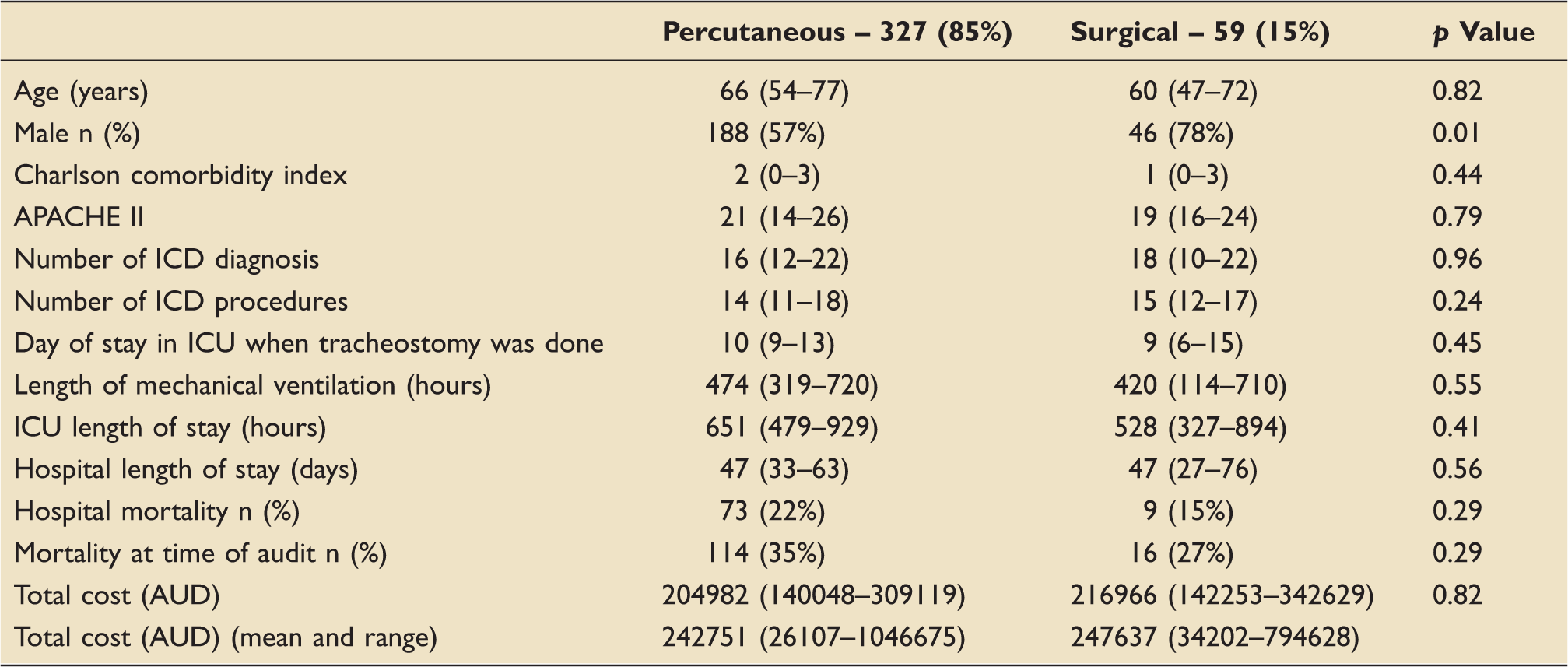
ICU: intensive care unit; APACHE: Acute Physiology and Chronic Health Evaluation.
Data represented as median (inter-quartile range), unless specified.
ICU tracheostomy patients examined as early and late group.
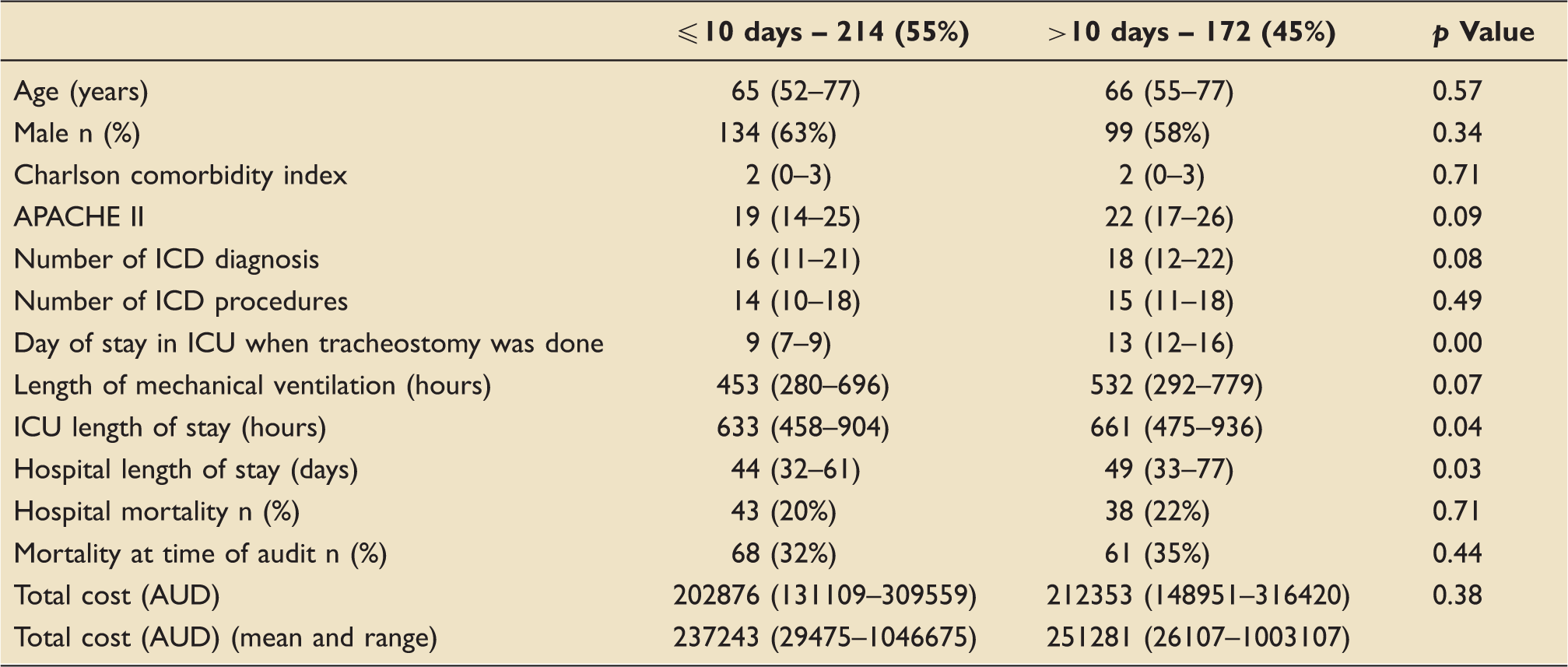
ICU: intensive care unit; APACHE: Acute Physiology and Chronic Health Evaluation.
Data represented as median (inter-quartile range), unless specified.
Factors (unstandardised β coefficient, standard error; p value) that predicted (adjusted R2 = 0.53) the cost per patient were ICU LOS (154, 12; p < 0.01) and hospital LOS (1708, 187; p < 0.01).
Discussion
This study reveals the high healthcare costs involved in the care of patients who undergo tracheostomy in an Australian setting. These patients typically have prolonged duration of invasive mechanical ventilation, ICU and hospital stay, and require multi-disciplinary care for extended time periods. Despite costly and resource-intensive care, this cohort of patients typically experience high morbidity and mortality.
Percutaneous versus surgical tracheostomy
The majority of the ICU patients in our study cohort underwent percutaneous tracheostomy at the bed side (85%). Previously it has been reported that percutaneous tracheostomy is more cost-effective and has fewer overall complications than surgical tracheostomy. 3 What is more relevant from a health system perspective, however, is the total cost of the care episode (or pathway), rather than just the procedure itself. None of the previous costing studies relating to tracheostomy report on the total costs of the care experienced by these patients. This is a major strength of our study. The previous studies have focused purely on the procedural costs associated with tracheostomy, including consumables and the personnel involved in the procedure.19,20 In addition, very few studies included details on the methods utilised to calculate costs.21,22
We did not find any discernible difference in cost or any other major outcomes examined between the groups (percutaneous and surgical group, Table 3; early versus late tracheostomy, Table 4). It is possible that the relatively small number of surgical tracheostomies performed as compared to percutaneous tracheostomies may have caused a selection bias. A previous meta-analysis comparison of open versus percutaneous tracheostomy found that the percutaneous technique was less resource-intensive and less costly than the open surgical technique (by an average of $456.61 USD). 3 However, as demonstrated in this study, such marginal cost benefits may be easily overshadowed by the major costs associated with the resource-intensive care provided to patients undergoing tracheostomy in the long run.
Early versus late tracheostomy
There is some evidence that early tracheostomy decreases the LOS and critical care resource utilisation,23–25 thereby reducing costs overall. 26 However, by delaying the decision on tracheostomy, about half of the patients may get the opportunity to recover enough to not need the tracheostomy, thereby indirectly saving costs. 7 Overall there was no difference in mortality and duration of mechanical ventilation.17,27 Although we found small differences in length of ICU and hospital stay, we did not find any difference in the mortality or costs associated with the care of these patients. It is also plausible that patients undergoing early tracheostomy were experiencing milder morbidity. However, the lower APACHE score (severity of illness score) did not reach statistical significance in our study. Also, calculating the cost of tracheostomy is not only about the cost of tracheostomy tubes, LOS, and mechanical ventilation.28,29 Obviously these are important, but what may be more important and relevant is the composite summation of the different services that are required in the short- and long-term management of these patients. The composite cost of these patients was not different between the early and late groups (Table 4). The majority of these patients have a prolonged stay in ICU and hospital as seen in our study. Finally, the mortality rates in ICU patients requiring tracheostomy is high (overall 33%), indicating the need for end-of-life care issues to be considered for a significant proportion of patients. Similar rates have been reported in previous studies,7,30 suggesting generally poor outcomes in this cohort of patients.
MDT approach in management of these patients
Previous studies have noted that the introduction of a multi-disciplinary approach in the management of tracheostomy patients (comprising a specialist physician, nurse consultant, physiotherapist, and speech pathologist) has been associated with reductions in LOS, duration of cannulation, and possible cost savings.4–6 However, the total costs associated with the introduction of an MDT approach in this context have not been examined in detail to date. A multi-disciplinary tracheostomy working party which brings ICU, ENT, physiotherapy, and speech therapy together may facilitate the fast tracking of the management of this often-complicated group of patients.4–6 Participation in a larger multi-institutional, multi-disciplinary collaborative 31 that collects data on patients undergoing tracheostomy, where experiences and data can be shared and built upon, would also be valuable in the management of these patients. We have recently initiated an MDT approach for the care of patients undergoing tracheostomy in our healthcare setting and we intend to comprehensively examine the costs and outcomes associated with this approach as the next stage of the research outlined here.
Strength and limitations
We have examined morbidity and mortality of patients undergoing tracheostomy in a tertiary level hospital in an Australian context. We have also examined the total cost of managing these patients in this context. To our knowledge this is the first study to examine the total cost of the care pathways experienced by this complex cohort of patients. Our study has some limitations. Firstly, it was retrospective in design and there may be a possibility of incorrect data entry. However, the possibility of recording errors was reduced as each patient record was manually cross-checked from other databases including their hospital and ICU record number, name, and date of birth. As indicated previously, surgical tracheostomy patients were relatively under-represented in our study, which means that any comparisons in costs and outcomes for surgical versus percutaneous tracheostomy patients should be treated with caution. To our knowledge this study represents the most comprehensive detailed analysis undertaken to date of the total costs associated with the care pathways for patients undergoing tracheostomy. However, the costs need to be continually updated and the findings presented here need to be confirmed in other clinical settings and for larger group of patients.
Conclusion
Hospitalised patients undergoing tracheostomy experience high morbidity and mortality and typically experience highly resource-intensive and costly healthcare. Interventions such as an MDT approach should be considered in order to improve the quality and the cost-effectiveness of the care provided for this unique cohort of patients.
Quick look
Footnotes
Authors’ contribution
Substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data for the work: Shailesh Bihari, Shivesh Prakash, Paul Hakendorf, Christopher MacBryde Horwood and Steve Tarasenko. Drafting the work or revising it critically for important intellectual content: Shailesh Bihari, Shivesh Prakash, Andrew W Holt, Julie Ratcliffe and Andrew D Bersten. Final approval of the version to be published: Shailesh Bihari, Shivesh Prakash, Paul Hakendorf, Christopher MacBryde Horwood, Steve Tarasenko, Andrew W Holt, Julie Ratcliffe and Andrew D Bersten. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: Shailesh Bihari, Paul Hakendorf, Julie Ratcliffe and Andrew D Bersten.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.