
Abstract
Autism is a lifelong neurodevelopmental condition. Autistic people face challenges as patients in the intensive care unit (ICU) and as providers of healthcare in the ICU. This article describes the experience of autistic people using a neurodiversity-affirming approach. Using the ‘Autistic SPACE’ framework, the needs of autistic people are described in terms of sensory needs, need for predictability, need for autistic acceptance, communication differences and how to approach them, and the benefits of a person-centred empathy-based approach to autistic people. The approach to autistic patients is described in terms of reasonable adjustments within a framework of positive risk taking. For supervisors and managers of autistic healthcare professionals, autism-friendly adjustments to training and working practice, with rationales, are suggested.
Introduction
Autism is a lifelong neurodevelopmental condition. Autistic people face challenges as patients within the ICU (intensive care unit) and as providers of healthcare. This article will discuss the challenges of delivering person-centred care to autistic patients in ICU, and the experiences of autistic healthcare professionals (HCPs) and describe adjustments to usual practice that may benefit these groups using the novel framework ‘Autistic SPACE’.
Diagnostic criteria and recognition of autism
The International Classification of Diseases (ICD10) defines autistic spectrum disorder as characterised by ‘persistent deficits in the ability to initiate or sustain reciprocal social interaction and social communication and by a range of restricted, repetitive and inflexible patterns of behaviour, interests or activities that are clearly atypical or excessive for the individual’s age and sociocultural context.’ 1
Autistic people may exhibit sensory sensitivity to stimuli such as sound, light, touch (especially light touch) texture or taste of food, temperature or the feeling of clothing. These deficits must be considered severe enough to cause impairment in personal, family, social, educational or occupational function. There is considerable heterogeneity in how autistic features present in an individual. Changes in environment or external stressors may lead to fluctuation; for example, an autistic person with usually fluent speech may become non-speaking in the presence of stressful environmental stimuli. 2
The estimated prevalence of autism in the population of the United Kingdom (UK) is 1.1% but this is likely an underestimate. The ratio of male to female people diagnosed as autistic is estimated at 3:1–5:1.1,3 Autism in women and girls is more likely to go unrecognised by parents, teachers and healthcare providers. Women and girls are more likely to be identified as autistic late in life if at all.4,5 People from a minority ethnic background are also more likely to face challenges accessing diagnostic and support services. 6
Recent autism-centred research and advocacy has supported a move towards ‘neurodiversity affirming’ rather than ‘deficit-focused’ approaches to autism and autistic people, framing challenges faces by autistic people as driven by limited understanding and inadequate accommodations made for them, rather than inherent deficits within them. Person-first language (autistic person versus person with autism) and using the term autism spectrum condition rather than disorder, forms part of the autism-affirming approach used by this article. 7 Definitions of terms used in this article can be found in Table 1.
Definitions of key terms.
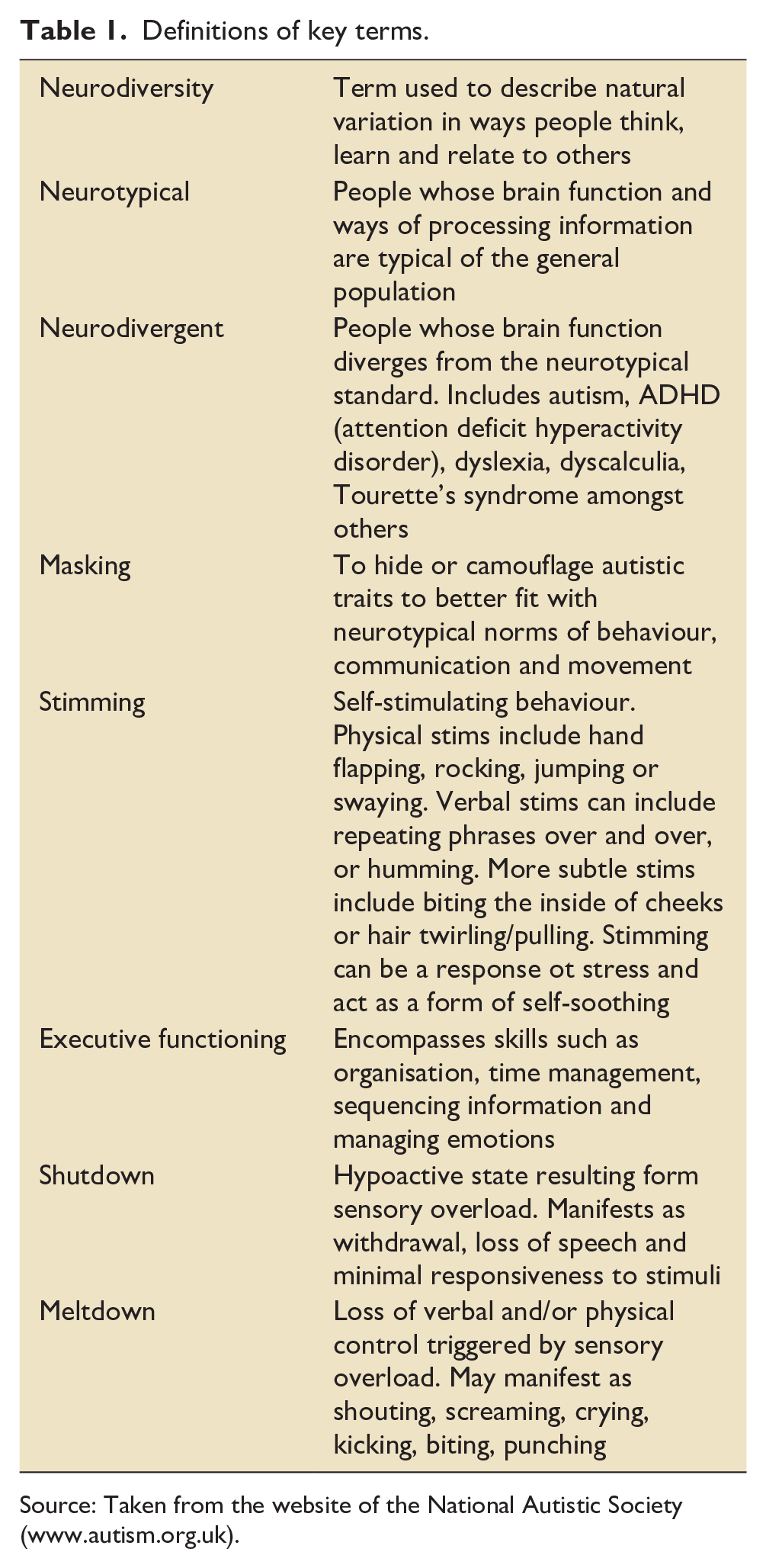
Source: Taken from the website of the National Autistic Society (www.autism.org.uk).
Autism is not a learning disability but approximately 40% of autistic people also have learning disabilities.8,9 This article will focus on the care of autistic patients without learning disabilities, but the principles of autism-affirming care can be extended to this group.
Autism and health outcomes
Autism coexists with other conditions and is associated with chronic poor health and premature mortality compared to the non-autistic population.10,11 Coexisting conditions include physical illness such as epilepsy, functional bowel disorders, chronic pain and hypermobility syndromes. Coexisting mental disorders may include anxiety, depression, sleep disorders, eating disorders and other neurodivergent conditions such as ADHD. 12
Autistic people experience poorer health outcomes compared to non-autistic people. The drivers of these poorer outcomes are multifactorial; autistic people may have impaired interoception (awareness of bodily sensations, such as pain) compared to non-autistic people, communication differences between autistic people and non-autistic healthcare professionals may lead to misunderstanding and misdiagnosis, and previous poor experiences accessing healthcare may result in a fear of seeking help and avoidance of healthcare settings as result. Autistic people may therefore present later, sicker and be more likely to need higher levels of care.13,14
Autistic SPACE
Autistic SPACE is a novel framework to aid healthcare providers and employers meet the needs of autistic patients and healthcare professionals. 15 The acronym ‘SPACE’ encompasses the core needs of autistic people: sensory needs, predictability, acceptance, communication and empathy. Three other wider, underpinning domains are built into the framework: physical space, processing space and emotional space.
The framework considers many of the difficulties faced by autistic people as not as a result of their autism but instead from the need for autistic people to exist in environments that are not designed for them. The Autistic SPACE framework is not prescriptive and accounts for the heterogeneity within the autistic population whilst giving healthcare providers, employers and trainers a means of systematically approaching the needs of autistic people. The following sections will utilise this framework to set out potential reasonable adjustments for patients and healthcare providers in ICU.
The autistic patient in ICU: Reasonable adjustments and positive risk taking
Autistic patients are highly likely to find ICU extremely challenging as a result of their communication, sensory and processing differences. The ICU environment may overwhelm autistic patients, with the constant presence of visual, auditory, tactile, gustatory and olfactory stimuli. Healthcare providers’ usual communication styles may not be an effective way to communicate with autistic patients, who also must ensure near total loss of usual routine and control over daily activities, surrounded by an ever-changing and unfamiliar staff group. The sensory and communication challenges of ICU may overload an autistic patient’s ability to cope, resulting in severe distress. 16
Strategies for improving the experience of autistic patients in ICU should be formulated with engagement from the patient (if possible), family members or friends and healthcare providers who may work with the patient in the community. Some autistic people carry ‘healthcare passports’ detailing what adjustments should be considered for them in healthcare settings; these should be accessed if available. Liaising with the hospital’s Autism Resource Team is encouraged. These teams are made up of multidisciplinary practitioners trained to support and advise autistic patients and healthcare teams within healthcare settings but may not be available in all hospitals and healthcare networks. In the absence of a specific Autism Resource Team, the Learning Disabilities Team may be able to provide advice and support to ICU staff, families and patients, even for autistic people without learning disabilities.
The UK Equality Act (2010) places an obligation on hospitals to make reasonable adjustments for people with disabilities, including autism. Reasonable adjustments may be defined as modifications to usual practice designed to eliminate or reduce any disadvantage a disabled person may experience as a result of their disability. For autistic patients in ICU, reasonable adjustments may be conceptualised as a form of positive risk taking, deviating from usual practice when necessary, aiming to identify and centre the sensory and communication needs of the patient whilst actively and continually balancing these with potential risks of deviations from usual practice.17,18 Every autistic person is different and the suggestions below should be considered on a person by person basis. The adjustments described below encompass the wider needs of autistic patients in terms of physical space, processing space and emotional space.
Autistic SPACE for patients in ICU
Sensory needs
ICU is an unpleasant sensory experience for all patients. For autistic patients who are likely to have pre-existing sensory sensitivities to light, sound, touch, smell and taste, the sensory challenges of ICU are cumulative, and may quickly become overwhelming. 15 This may result in meltdowns or shutdowns (see Table 1), which may be misdiagnosed as hyper or hypoactive delirium.
Mitigating sensory challenges for autistic patients requires positive risk taking. Modifications to usual care should be decided on a patient-by-patient basis and clearly communicated to all members of the ICU and visiting teams, to avoid variations in care. All reasonable adjustments carry a degree of risk; as part of positive risk taking the rationale behind each adjustment including potential risks as well as benefits should be discussed with the patient, family and multi-disciplinary team. 17 Reasonable adjustments may include:
Alarm limits and volume levels should be set at an appropriate volume to minimise alarm noise without compromising safety.
Offer noise cancelling headphones to the patient. Side room accommodation may minimise noise and visual stimuli. ‘Background’ TV and radio may be an additional source of auditory stress and should be avoided unless agreed with patient or family.
Minimise bright direct overhead light and offer dark glasses if desired.
Aim to keep the bedspace temperature at a level that suits the patient; heat or cold intolerance is common in autistic people.
Review the need for standard monitoring regularly. It may be appropriate to, for example, remove ECG (electrocardiogram) monitoring at an earlier stage than usual. Arterial blood gas monitoring can be discontinued as soon as possible in favour of pulse oximetry monitoring, to facilitate removal of invasive arterial catheters.
Touch, especially light touch, may be unpleasant for autistic people. Restrict touching to examination and procedures – hand holding and other caring touch may increase stress levels by increasing physical proximity. Close physical contact may lead to tactile defensiveness and be mistaken for agitation or aggression. Describe why and how you will touch the patient in advance of touching.
Continuous monitoring should be substituted for intermittent monitoring as early as safely possible.
Sedation holds should be kept to a minimum; these may be highly distressing for patients. There is no evidence to guide the optimal sedation regimen for autistic people in ICU but use of drugs such as clonidine and dexmedetomidine may be helpful. 19
Sedation may need to be offered for procedures that may not normally require sedation, for example, tracheostomy changes or urinary catheterisation.
Aim to keep the patient’s care team as small as possible to minimise exposure to new members of staff. During ward rounds, minimise the number of people within the room.
Once oral diet is tolerated, allow family to bring in ‘safe foods’ from home. Autistic people may have strong sensory aversions to certain tastes, textures or colours of foods and allowing familiar foods to be brought in for them may reduce time to full resumption of oral intake.
Predictability
Whiteboards within clear sight of the patient displaying daily routine may reduce anxiety from loss of control over routine and avoid overwhelming the patient as a result of verbally describing the whole day’s activities at the start of the morning shift.
Where possible, allocate a small group of staff to look after the patient to minimise frequent exposure to unfamiliar staff members.
Encourage the patients’ family to bring in blankets, decorations and other familiar objects for comfort. This may require negotiation with infection prevention and control teams.
Acceptance
Minimising variation in care and maintaining regular routine is a central part of delivery of care in the ICU. Deviations from normal routine can be unsettling for staff members. Gaining acceptance from the wider healthcare team of the benefits of specific adjustments in care delivery is crucial. Education and support of staff looking after autistic patients, including acknowledging concerns arising from variations in usual care with potential associated risks, is a crucial part of ensuring autistic patients receive person-centred care. This may include supporting staff who feel they may be neglecting or mistreating patients by avoidance of touch and eye-contact.
Communication adjustments
The ‘double empathy’ problem describes how lack of understanding of the communication differences experienced by autistic people by non-autistic people leads to communication difficulties. 20 This framing of communication between autistic and non-autistic people reframes communication difficulties away from being caused by communication deficits in the autistic person, to a need for both parties in the conversation to understand the differences in the way they communicate to allow for successful communication.
Reasonable adjustments to facilitate effective communication should include modifications to both style and content of written and verbal communication, with the aim of predicting and reducing these difficulties.
Some autistic people may be non-speaking from birth. Non-speaking autistic people should be given access to appropriate aids to allow communication where possible. Autistic people who have access to speech may lose this in periods of intense stress and may communicate more effectively using communication aids or written notes. 18 ICU interventions such as endotracheal intubation may render speaking autistic people non-speaking, and usual practice to enhance communication with this group, modified by the SPACE framework, should be used.
Autistic people may benefit from direct, concise styles of communication, more closed forms of questioning, and avoidance of figurative language, humorous or ironic speech.
Autistic people may have learned to ‘mask’ by adopting more neurotypical forms of facial expression, vocal modulation and body language, but may struggle to mask when unwell or stressed. Healthcare providers should avoid reading into flat affect or vocal tone, particularly when assessing for pain.
Small talk and eye contact may be possible for autistic people to maintain but are energy-depleting at a time of stress; these can be minimised or avoided without fear of appearing rude.
Autistic people may need longer to process verbal or written information and this may be more pronounced in times of stress. Give extra time to autistic patients and/or family members to process information. It may be better to deliver significant information over several meetings. Written material reflecting the key points of significance may be valuable.
Delirium assessment methods such as CAM-ICU (Confusion Assessment Method for the ICU) contain abstract instructions and questions and have not been validated in the autistic population. 19 This may lead to challenges in delirium assessment.
Empathy
Deviations from usual care may be unsettling for healthcare providers. Working through concerns around these practice modifications by aiming to understand the needs of autistic patients on an individualised basis using an empathy based approach has the potential to ameliorate many of the intensely distressing aspects of being a patient in ICU.
Healthcare providers may need to extend specific autism-friendly provisions to the families of autistic people. Autism is a heritable condition and it is likely that some family members will also be autistic and may potentially be undiagnosed. Accommodations for family members may include arranging specific visiting times to minimise time in busy waiting rooms, and utilising communication strategies similar to those described above.
The adjustments described above encompass the wider needs of autistic patients in terms of physical space, processing space and emotional space.
Summary
ICU care involves sensory and communication challenges for all patients. These challenges are magnified for autistic patients. By pre-empting difficulties that autistic patients may encounter and instituting reasonable adjustments by accepting a degree of risk in deviating from usual practice, these challenges may be partially mitigated. Clear communication with the patient, family and wider care team is essential. Seeking early advice and support from the hospital Autistic Support service, if available, is strongly encouraged.
Autism in ICU: The healthcare provider perspective
The prevalence of autism in healthcare providers is unknown. Many healthcare professions and medical specialities (including intensive care medicine) select for autistic traits and it is likely that there are many undiagnosed or undisclosed autistic people working within healthcare.21,22
Many autistic healthcare providers and students do not disclose their autistic identity in the workplace. The reasons for this include negative self-image as an autistic person as a result of the prevailing ‘tragedy narrative’ around autism, fear of stigma and exclusion from work or study, and a lack of positive role models of successful autistic healthcare providers.23,24 Autistic HCPs may receive a formal diagnosis in later life; a cross sectional study of autistic doctors demonstrated a mean age at diagnosis of 36 years. 24 These HCPs may have negotiated their education, training and a significant period of their working lives unaware of their autism and unable to avail themselves of appropriate workplace adjustments and accommodations.
Having positive self-identity as an autistic person is associated with improved wellbeing and mental health. 25 There is increasing visibility of autistic people within the medical profession, with networks such as Autistic Doctors International (www.autisticdoctorsinternational.com) providing peer support and advocacy for autistic doctors. Nursing, a traditionally female dominated profession, is characterised by empathy and patient-centred care; this is the opposite of the ‘extreme male brain’ stereotype of autistic people and may contribute to the paucity of visibility of openly autistic people within nursing and other female-dominated allied medical professions.26,27
Autistic SPACE and healthcare providers in ICU
Many traits possessed by autistic people lend themselves to working in ICU; attention to detail, pattern recognition, conscientiousness and a strong work ethic are all essential qualities for a successful career in intensive care medicine. 28 Without adequate understanding of their specific needs however, autistic healthcare providers may struggle and suffer adverse health events. 24
Healthcare providers are likely to have received minimal training in autism and the needs of autistic people. 29 They may be trained to view autism through a lens of pathology, not difference; this may contribute to students and trainees being less willing to disclose their autistic identity and not make use of resources and adjustments available to them. Stigma borne of negative stereotypes of autistic people is a significant barrier against disclosure 22 and may lead to pressure to appear as non-autistic as possible in order to ‘pass’ as neurotypical. Such ‘camouflaging’ or ‘masking’ may be more pronounced in women, who face additional pressure to appear sociable and emotionally attuned to others.5,30,31
Autistic healthcare providers and students will view and experience the ICU differently to their non-autistic colleagues. These differences may need employers and educators to make reasonable adjustments to working conditions to ensure autistic people are treated equitably. In the UK, the General Medical Council, Nursing and Midwifery Council and Health and Care Professions Council have guidance for employers and disabled practitioners setting out rights and responsibilities for HCPs and employers. Occupational Health specialists will be able to advise managers on implementation of adjustments for autistic employees and guide them towards funding sources if needed. For trainers, training bodies (such as NHS Education for Scotland in the UK) provide educational resources to allow trainee healthcare professionals to be appropriately supported in their ICU placements.
The ICU is a demanding working environment and when demands exceed personal resources available to manage demands, burnout may result. 32 Reasonable adjustments, if correctly implemented, monitored and regularly reviewed, may improve the workplace experience of autistic HCPs. 33 Using the Autistic SPACE framework, potential reasonable adjustments are detailed below. The requirements for considering wider needs in terms of physical, processing and emotional space for autistic patients also apply to autistic HCPs.
Sensory needs
Providing areas for ‘downtime’ in a minimally-stimulating environment during the working day – for example a small room where they can have meals away from the loud, smelly and socially active area of the breakroom – may allow autistic HCPs to decompress and reset their energy levels.
Open plan offices are very challenging for those with sensory sensitivities. Allowing working from home for non-clinical activities where possible can reduce sensory overload from shared working space.
Predictability
Do not underestimate how upsetting even minor changes in routine can be for autistic colleagues. For example, changes in uniform colour or fabric can be very unsettling for an autistic person, to the detriment of their performance.
Aim to minimise last minute schedule changes.
Keep in same teams where possible; if it is necessary to make changes, give the HCP as much notice as possible.
Autistic HCPs may benefit from pre-training sessions in new equipment or computer systems to allow maximum time to familiarise themselves and prepare mentally for the change.
Consider giving autistic new employees and students an individual induction to allow them to familiarise themselves with the layout and routine of the ICU.
Differences in executive functioning may lead to issues with timekeeping and organisation skills. Make instructions and expectations explicit and unambiguous, for example how long is reasonable to spend on a break period.
Acceptance
Autistic colleagues may be able to engage in ‘normal’ social contact one day but need solitude to allow themselves to maintain their energy levels on another day. Try to accept this and not label them as antisocial or unfriendly.
If a colleague discloses their autistic identity to you, believe them. They may appear neurotypical as a result of ‘masking.’ Autistic women in particular may be highly motivated to develop social connections through interactions in the workplace These interaction occurs at a cognitive rather than intuitive level and are highly energy-depleting. 5
Autistic people, particularly women, may fear coming across as cold or blunt, and may struggle with the social aspect of working relationships particularly with other women. 34 Be mindful of the differing communication styles and needs of autistic people, particularly women, if asked to provide feedback to supervisors or trainers. This may include facial expressions (including lack of eye contact) and tones of voice which may differ from neurotypical norms.
Accept that some autistic colleagues may not be able to attend social events outside of work. These are often noisy, require conversation that occur outside of the ‘scripts’ autistic people use for communication in the workplace, and may involve consumption of food which may not be possible for an autistic person with food-related sensory sensitivities. Not attending such events does not mean that an autistic colleague is not a ‘team player’.
Some teaching methods such as simulation may be challenging for autistic people. Incongruence between scenario set up and real life may act as a significant barrier for effective cognitive processing, leading to impaired simulated practice which may not reflect the ability of the HCP. 33
Communication
Many of the principles for communication that may be used with autistic patients can also be used with autistic colleagues. When communicating in clinical situations, it is helpful to use unambiguous, clear commands, and to check understanding after giving instructions. Avoidance of vague instructions (‘why don’t you go for a wander and see if anyone needs a hand with anything’) and figurative language may be helpful. Autistic people may struggle to know when to speak up in meetings, or when they should hold back and let others speak in group conversations; a sympathetic and autism-informed chair may be helpful to guide them in formal meetings.
Empathy
Working in ICU can be immensely rewarding. It can also be immensely challenging. These challenges may be amplified many times over for autistic colleagues, who have to deal with the cumulative impacts of sensory and communication differences whilst using additional cognitive and emotional energy to mask their autistic traits in an attempt to be better accepted by colleagues, families and patients.
Having the empathy to understand that autistic colleagues are not being difficult or over-sensitive but are people who experience the world differently is a crucial first step towards autism acceptance in the workplace. Although everyone may experience some of the challenges that autistic people do, it is the energy-depleting intensity of these challenges that render them problematic for autistic people. Being autistic is not an excuse for poor practice or behaviour but lack of empathy and understanding of the challenges faced by autistic HCPs can lead to impaired practice and burnout. 33
Having an autism mentor within each ICU, and autism-informed educational and clinical supervisors for trainees and students may help in supporting autistic healthcare professionals throughout their ICU careers, as well as promoting awareness and acceptance of autism in their units.
Summary
Autistic healthcare professionals have the potential to thrive in ICU, a clinical environment which contains as much routine as it does variety. 35 As a result of sensory and communication differences and need for predictability, autistic HCPs should be supported in the workplace by autism-informed supportive managers and supervisors to allow them to work to their full potential. Autism remains a stigmatised condition which inhibits individuals revealing their autistic identity at work; positive role-modelling by established autistic healthcare professionals may help deconstruct negative stereotypes of autistic people and allow autistic healthcare professionals to develop a positive professional identity.
Conclusion
Autism and the challenges faced by autistic people are often poorly understood. Many of the adjustments to usual practice described in this article cost little or nothing to implement but do require an awareness of the sensory and communication differences of autistic people, who have a need for predictability in their daily routines. Such awareness and acceptance coupled with an empathetic approach and, in caring for autistic patients, a positive attitude to risk taking, has the potential to greatly improve the experience of ICU for autistic people.
Footnotes
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author is autistic and is the ICU lead of Autistic Doctors International, a not-for-profit peer support and advocacy network.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.