
Abstract
Background:
Venous thromboembolism (VTE) in critically ill patients has been well-studied in Western countries. Many studies have developed risk assessments and established pharmacological protocols to prevent deep venous thrombosis (DVT). However, the DVT rate and need for pharmacologic VTE prophylaxis in critically ill Taiwanese patients are limited. This study aimed to prospectively determine the DVT incidence, risk factors, and outcomes in critically ill Taiwanese patients who do not receive pharmacologic VTE prophylaxis.
Methods:
We conducted a prospective study in a surgical intensive care unit (SICU) of a tertiary academic medical center in Taiwan. Adult patients admitted to SICU from March 2021 to June 2022 received proximal lower extremities DVT surveillance with venous duplex ultrasound. No patient received pharmacologic VTE prophylaxis. The outcomes were the incidence and risk factors of DVT.
Results:
Among 501 enrolled SICU patients, 21 patients (4.2%) were diagnosed with proximal lower extremities DVT. In a multivariate regression analysis, hypoalbuminemia (odd ratio (OR) = 6.061, 95% confidence interval (CI): 1.067–34.421), femoral central venous catheter (OR = 4.515, 95% CI: 1.547–13.174), ICU stays more than 10 days (OR = 4.017, 95% CI: 1.270–12.707), and swollen leg (OR = 3.427, 95% CI: 1.075–10.930) were independent risk factors for DVT. In addition, patients with proximal lower extremities DVT have more extended ventilator days (p = 0.045) and ICU stays (p = 0.044).
Conclusion:
Our findings indicate critically ill Taiwanese patients have a higher incidence of DVT than results from prior retrospective studies in the Asian population. Physicians who care for this population should consider the specific risk factors for DVT and prescribe pharmacologic prophylaxis in high-risk groups.
Keywords
Introduction
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), has been studied worldwide for decades. 1 A DVT is defined as “a blood clot that develops within a deep vein,” 2 and is the most common source of life-threatening PE 3 and is more dominant in the lower limbs than in the upper limbs. 4
Guidelines for pharmacologic prophylaxis are especially robust for trauma patients,5,6 with a recent Consensus Conference providing guidance on current and future dosing strategies.7 –9 The recommended dosing for pharmacologic prophylaxis for critically ill patients who require admission to a surgical intensive care unit (SICU) may be challenging due to varied VTE incidence and bleeding risk of anticoagulants. 10 Risk factors for VTE in critically ill patients have been reported in prior studies.11,12
However, most guidelines were developed according to studies in Western countries. And the incidence of VTE in Asian populations has been reported to be four-times lower than Western populations. 13 Moreover, the Asian VTE studies may not provide an accurate incidence of VTE due to their retrospective nature.14,15 This unclear information on VTE in the Asian population makes it challenging to apply VTE prophylactic strategies in Asian populations such that many patients are not treated with pharmacologic prophylaxis.
Therefore, our study aims to identify prospectively the incidence and predictors of the proximal lower extremity (PLE) DVT in a critically ill Taiwanese population. The primary outcome was the incidence of PLE DVT in patients who require SICU admission. The secondary outcomes were risk factors of DVT, mechanical ventilation duration, ICU stay, hospital stay, as well as in-hospital mortality.
Materials and methods
Ethics
This study was approved by the Institutional Review Board of Kaohsiung Chang Gung Memorial Hospital, Taiwan (201901847B0C501). Procedures were followed in accordance with the standards of this committee and the 1975 Helsinki Declaration. All families or patients who could understand the study provided written informed consent to participate in the trial.
Study design, setting, and participants
From March 2021 to Jun 2022, all consecutive adult Asian patients (⩾20 years old) admitted to the SICU for more than 48 h at Kaohsiung Chang Gung Memorial Hospital, a tertiary academic medical center in Taiwan, were included. The 23-bed multispecialty ICU treats critically ill patients following surgery, trauma, or unstable hemodynamics, including septic shock or respiratory failure.
All patients received a venous duplex ultrasound (VDU) for DVT surveillance of the bilateral PLE. The VDU was performed 48–72 h after SICU admission, then every 7 days while the patient remained in the SICU. Patients were excluded when diagnosed with DVT before ICU admission, isolated for resistant bacterial infection, unsuitable to receive a VDU study, or hesitant to join the study. Patients were deemed unsuitable for VDU if there were time limitations, agitation, or anatomic limitations due to wound or dressing. Patients had time limitations because of being transferred to another unit for further procedures or health care. In addition, the patients no longer received VDU once they became isolated for resistant bacterial infection, were diagnosed with DVT in the SICU, or were transferred to another unit. When patients were readmitted to the SICU, a repeat VDU was performed for patients who fit the inclusion criteria. In patients who underwent multiple VDU examinations, the last examination of the same SICU admission was used for additional analysis.
Screening duplex ultrasound
Three VDU operators, including one cardiologist and two surgical intensivists, performed the examinations on each patient using the Philips CX50 system (Philips Healthcare, Andover, MA, USA) with a linear transducer (high frequency, 7–12 MHz). The cardiologist trained and supervised the two surgical intensivists in the VDU examination. Each examination had official images and a report.
Each VDU examined the four items: visible venous thrombosis, venous compressibility, venous color flow, and venous phasicity in the deep vein of the bilateral PLE. In addition, the proximal deep vein included the common femoral vein, superficial femoral vein, and popliteal veins. 16 All VDU examinations were made with the participants lying supine.
Patients were diagnosed with DVT if they had visible thrombosis or were positive for two of another three items (venous compressibility, venous color flow, or venous phasicity in the deep vein of the bilateral PLE). In patients diagnosed with DVT, cardiologists were consulted for anticoagulant treatment.
Data collection
We collected patient information from the health information system, including demographics, patient source, ICU stays on the VDU day, comorbidity, Acute Physiology and Chronic Health Evaluation II score, 17 Sequential Organ Failure Assessment, 18 and recorded the swelling of the lower extremities which were commonly observed in patients with DVT or with critical illnesses.
Serum laboratory parameters were retrieved, including white blood cell count, hemoglobin, international normalized ratio, activated partial thromboplastin time, creatinine, total bilirubin, sodium, C-reactive protein, and albumin level.
In addition, we collected operation-associated factors, including the American Society of Anesthesiologists physical status classification, 19 operation wound classifications, 20 duration of operations, intraoperative blood loss, number of operations, operation regions, and operating divisions.
Intervention information was collected, including blood transfusion in the 24 h before the VDU examination, sedation medications, vasopressors, femoral central venous catheter (CVC), and total parenteral nutrition (TPN) on the VDU day. CVC included a central venous catheter for resuscitation or a double-lumen catheter for hemodialysis. We also collected trauma-associated factors, including Injury Severity Score, 21 Abbreviated Injury Scale, 22 and specific injury regions.
Statistical analysis
Values for continuous variables were expressed as means ± standard deviation (SD) or median (interquartile ranges (IQRs)). The categorical variables are expressed as the number and percentage of the group from which they are derived.
The independent sample t-test was used for continuous variables for the univariate study, and the Mann-Whitney U test was used for nonparametric data. The chi-square or Fisher’s exact test was used for categorical variables, as appropriate. The optimal cut-point value was identified in continuous variables on the receiver operating characteristic curve.
Variables with a p < 0.1 in univariate analysis were included in a multivariable logistic regression analysis. We used time-to-event analysis to compare the in-hospital mortality of patients with and without DVT. A cumulative event curve (censored endpoints) was estimated with the Kaplan-Meier procedure. Continuous variables were changed to category type to overcome the missing data during regression analysis.
A p-value of <0.05 was considered statistically significant. Statistical analyses were conducted using SPSS software (version 22.0 Chicago, IL, USA).
Results
Characteristics
A total of 501 adult SICU patients enrolled in the study (Figure 1). No patients received DVT pharmacological prophylaxis; 21 patients (4.2%) were confirmed to have DVT of the PLE via VDU. A total of eight patients (1.6%) required CT pulmonary angiogram due to clinical suspicion for PE. No patient was diagnosed with PE during the same hospitalization.
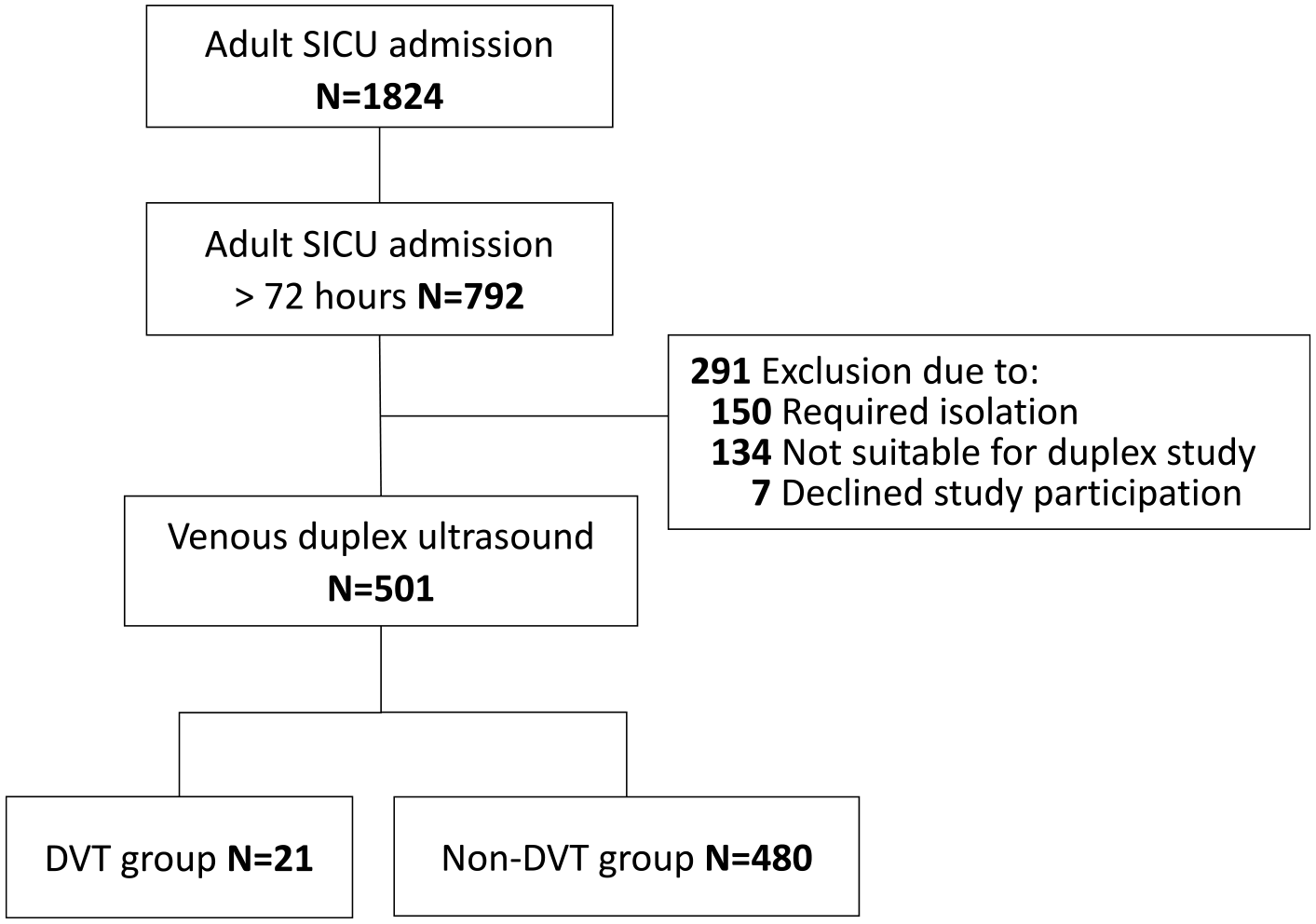
Flow diagram of patient selection.
eTable 1 shows the characteristics of the enrolled patients divided into DVT (N = 21) and Non-DVT (N = 480) cohorts. Among these patients, a total of 701 VDU examinations were performed. Every patient received a mean of 1.39 VDU with a minimum of 1 and a maximum of 6. 76.2% of patients received only one VDU, while 0.2% received six times VDUs (eFigure 1).
Univariate analysis
In the univariate analysis (eTable 1), the two groups had no significant difference in age, sex, body mass index, and patient source. However, the DVT group was prone to have ICU stays for more than 10 days on the VDU day (52.4%vs 25%, p = 0.005), moderate chronic kidney disease (Serum creatinine > 3 ng/dL) (28.6%vs 12.3%, p = 0.042), lower Glasgow Coma Score (10 (9–11) vs 11 (10–14), p = 0.040), lower serum albumin levels (2.7 ± 0.4vs 3.0 ± 0.5 g/dL, p = 0.046), and leg swelling compared with the non-DVT group (23.8%vs 7.5%, p = 0.022) on the VDU day.
When intervention and operation cohorts were compared (eTable 2), there was no significant difference between the two groups, except the DVT group was more likely to have femoral CVC insertion (38.1%vs 8.8%, p < 0.001) and a nonsignificant trend toward repeat surgery (50%vs 28.5%, p = 0.051).
Multivariate analysis
In the multivariate analysis, the independent risk factors for DVT were hypoalbuminemia before ICU admission (odds ratio (OR) = 6.061, 95% confidence interval (CI): 1.067–34.421, p = 0.042), femoral CVC insertion (OR = 4.515, 95% CI: 1.547–13.174, p = 0.006), ICU stays more than 10 days (OR = 4.017, 95% CI: 1.270–12.707, p = 0.018), and swollen leg (OR = 3.427, 95% CI: 1.075–10.930, p = 0.037) (Table 1).
A multivariate analysis of predictors of DVT in SICU patients.
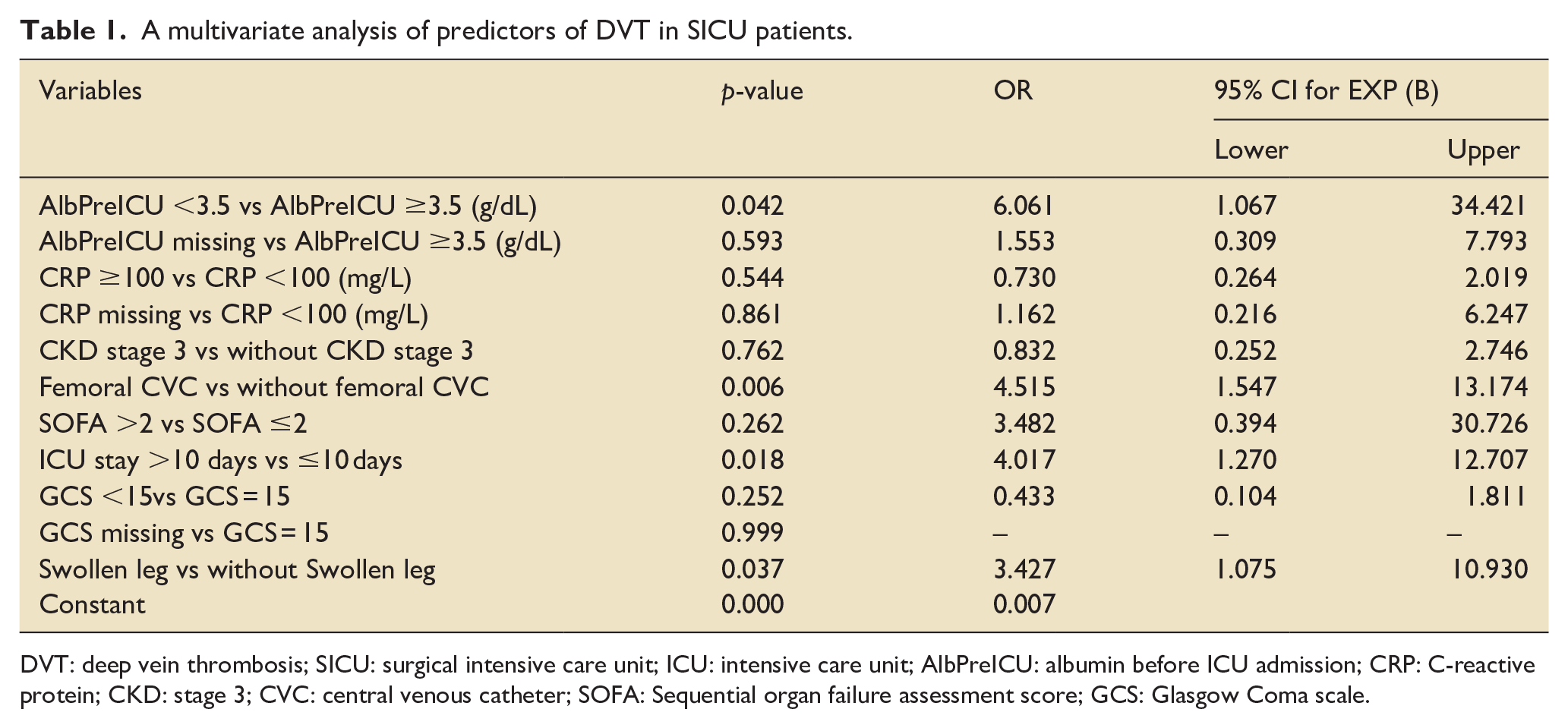
DVT: deep vein thrombosis; SICU: surgical intensive care unit; ICU: intensive care unit; AlbPreICU: albumin before ICU admission; CRP: C-reactive protein; CKD: stage 3; CVC: central venous catheter; SOFA: Sequential organ failure assessment score; GCS: Glasgow Coma scale.
Outcome analysis
Patients were followed until discharge from the hospital. In the outcome analysis (Table 2), the DVT group had a more extended ventilator day (4.0 (1.5–22.5) days vs 3.0 (1.0–7.0) days, p = 0.045) and ICU stays ( 13.0 (5.0–31.0) days vs 7.0 (5.0–12.0) days, p = 0.044). However, there were no significant differences in-hospital stay and in-hospital mortality between the DVT and non-DVT groups. In addition, the Kaplan-Meier survival analysis showed no significant difference in cumulative in-hospital survival (p = 0.894) (eFigure. 2).
The outcomes of patients with and without deep vein thrombosis.
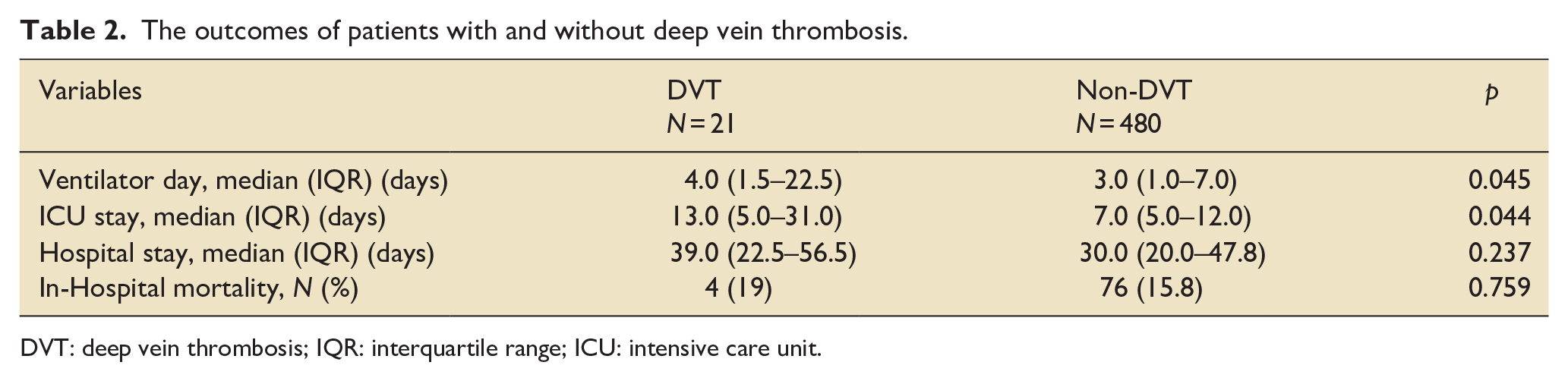
DVT: deep vein thrombosis; IQR: interquartile range; ICU: intensive care unit.
Discussion
This prospective, observational study focused on identifying the incidence and risk factors for proximal lower extremities DVT in a critically ill surgical Taiwanese population. The VDU, a point-of-care ultrasound centered on the PLE, found that the DVT incidence was around 4%. The independent risk factors were extended ICU stay, femoral CVC insertion, hypoalbuminemia, and leg swelling. Although there was no difference in hospital stay and in-hospital mortality between the two groups, the DVT group had longer mechanical ventilation days, and ICU stays.
VDU in critically ill patients
Venous duplex ultrasound is one of the diagnostic tools for deep vein thrombosis. 23 This point-of-care duplex, which may be performed by physicians at the patient’s bedside, is a noninvasive, relatively easy technique to learn, free of ionizing radiation risks, and efficient examination because of more rapidly accessible. 24 All these benefit critically ill patients who are not easily transferred to another unit for DVT diagnosis or are prone to contrast-related kidney injury. 25 On the other hand, routine weekly VDU surveillance in high-risk patients has been proven to decrease PE.6,26 In our series, VDU surveillance identified PLE DVT in ICU and prompted early DVT therapy. With this strategy, no SICU patients sustained PE during their hospitalization. To our knowledge, VDU is a feasible, safe, and effective modality to survey DVT in critically ill patients.
Incidence of DVT
The incidence of DVT in trauma patients was as high as 59.9% in Western countries27,28 compared to approximately 28% in Asian populations.29,30 The lower incidence of DVT in Asian populations might be due to a lower prevalence of inherited disorders such as factor V Leiden or the prothrombin 20210A mutation.31,32 In a prospective surveillance of lower extremities DVT in a Western critically ill population, Cook et al. 33 conducted lower extremity compression ultrasounds within 48 h of ICU admission and twice weekly. The DVT incidence in their series ranged from 2.7% to 9.6%. With a similar protocol on patients who did not receive pharmacologic prophylaxis, the PLE DVT incidence in our study was 4.2%. However, some potential bias contributed to the two study’s different results. First, Cook et al. surveyed DVT proximal and distal lower extremities, while our study surveyed only proximal lower extremities. Second, Cook et al. performed VDU twice weekly while we performed VDU every week. Compared with previous retrospective studies on Asian populations that demonstrated a DVT rate of <1%,15,34 this prospective study provides evidence of a higher DVT rate among Taiwanese patients.
ICU stay is a risk factor
Prolonged immobility is an independent predictor of DVT in the ICU due to mechanical ventilation and pharmacological sedation.35,36 In 1991, the risk assessment tool developed by Caprini et al. calculated the VTE risk in surgical patients and added two more points to the DVT score when patients were confined to bed for 72 h. 37 In 2009, a prospective study on critically ill surgical patients in Thailand found that the longer the ICU stay, the higher the DVT rate. 38 Our study is similar to previous publications; ICU stays for more than 10 days are associated with increased PLE DVT risk.
Femoral CVC is a risk factor
In a meta-analysis, Tran et al. enrolled 39 observational cohort studies and 729,499 patients. They discovered that CVC insertion is associated with VTE events in critically ill patients. 39 Moreover, a catheter-related DVT may occur as soon as 1 day after insertion and is mostly asymptomatic. 40 Endothelial damage caused by CVC was thought to be the pathophysiology of thrombus formation. 41 In the risk assessment profiles of Caprini et al. 37 and Greenfield et al., 42 patients who have had a femoral CVC insertion for >24 h received two points for the DVT score. Our multivariate analysis determined that patients with femoral CVC insertion, either for resuscitation or hemodialysis, were more likely to have PLE DVT. Therefore, ICU physicians should be aware of the risk of catheter related thrombosis upon placement and remove the femoral CVCs as soon as the catheter is not required.
Lower serum albumin is a risk factor
The serum albumin produced by the liver is vital for maintaining the oncotic pressure and properly distributing body fluids between blood vessels and soft tissues. 43 Critically ill patients with hypoalbuminemia may have tissue edema and delayed postoperative recovery. 44 In 2016, Truong et al., 45 using data from the extensive national NSQIP database, established that lower serum albumin significantly increased the risk of developing a postoperative DVT in a colorectal cohort. In another study of 1500 geriatric intertrochanteric fracture patients, hypoalbuminemia was an independent DVT risk factor. 46 The pathophysiology was explained as decreased venous flow secondary to intravascular volume depression. Our study on critically ill surgical patients also identifies hypoalbuminemia as an independent PLE DVT risk factor. Therefore, care providers in ICU should be aware of DVT risk in patients with lower serum albumin.
Leg swelling is a risk factor
Critically ill patients in ICU usually have limb edema because of immobility, low serum albumin levels, cellulitis, and fluid overload.47,48 Limb edema, as detected on physical examination, is a poor prognostic indicator in critically ill patients. 49 In addition, leg swelling can also be due to a DVT. In Caprini et al.’s risk assessment tool, 37 patients with swollen legs received one point added to the DVT score. Marik et al. conducted prospective venous duplex scans on 102 ICU patients and suggested that limb edema in ICU is associated with DVT. 50 Despite many etiologies of leg swelling in ICU patients, and it is hard to clarify the leg swelling as an effect or cause of DVT, our study concurs that leg swelling is associated with a higher rate of PLE DVT.
This study carries limited information for the Western population because there have been well-established recommendations for pharmacologic prophylaxis in Western countries. This study focuses only on the Taiwanese population and should not be directly applied to all Asians. Other Asian or Asian populations living in Western countries may have different presentations due to different generic risk profiles and lifestyles, requiring further prospective studies to know their true incidence of DVT.
Limitation
This study had several limitations. First, it was a single tertiary center study and required external validation. Second, this prospective cohort may lose some confounders. Third, the small number in the DVT group may interfere with the statistics results. Fourth, this study did not analyze the factors associated with inherited thrombophilic syndromes, which are rarely seen in the Asian population. Fifth, patients who needed contact isolation were excluded from the VDU examination. However, this group usually has higher disease severity, longer ICU stays, and may have a greater chance of developing DVT. Lastly, the patients studied were only followed in the SICU. Those patients who developed DVT after transfer from the SICU might not be identified leading to a DVT rate that is lower than the actual rate.
Conclusion
This prospective study identified a higher incidence of proximal lower extremities DVT in critically ill Taiwanese patients who were not treated with pharmacologic prophylaxis compared to prior studies on Asian patients. In addition, VDU is a feasible and effective modality to survey PLE DVT in the critical care field. Physicians should monitor for the risk factors for DVT and consider pharmacologic prophylaxis to reduce VTE events in high-risk groups. Further studies are needed to validate our results and optimize the strategies for managing DVT in critically ill surgical Asian patients.
Supplemental Material
sj-docx-1-inc-10.1177_17511437231214906 – Supplemental material for The incidence and risk factors of proximal lower extremity deep vein thrombosis without pharmacologic prophylaxis in critically ill surgical Taiwanese patients: A prospective study
Supplemental material, sj-docx-1-inc-10.1177_17511437231214906 for The incidence and risk factors of proximal lower extremity deep vein thrombosis without pharmacologic prophylaxis in critically ill surgical Taiwanese patients: A prospective study by Ting-Lung Lin, Wen-Hao Liu, Wei-Hung Lai, Ying-Ju Chen, Po-Hsun Chang, I-Ling Chen, Wei-Feng Li, Yueh-Wei Liu, Eric J Ley and Chih-Chi Wang in Journal of the Intensive Care Society
Footnotes
Abbreviations
VTE venous thromboembolism, DVT deep vein thrombosis, PE pulmonary embolism, ICU intensive care unit, CVC central venous catheter, PLE proximal lower extremities, SICU surgical intensive care unit, VDU venous duplex ultrasound, TPN total parenteral nutrition.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We appreciate the staff members of the SICU at Kaohsiung Chang Gung Memorial Hospital (grant number: CMRPG8L0431) for patient management and the Biostatistics Center at Kaohsiung Chang Gung Memorial Hospital for statistics work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.