
Abstract
Precise and timely nutrition support is essential for good outcomes in a critical care setting. Individuals with body mass index (BMI) in the overweight or obese category are often assumed to be well nourished, and are therefore at risk of being overlooked for nutrition support. This single centre clinical audit evaluated the incidence of malnutrition on admission of patients with BMI > 25. Results suggested that 70%–80% of individuals in this category can be considered either malnourished or at risk of malnutrition. This demonstrates the need for urgent, personalised nutritional care for critically ill patients regardless of body size.
Introduction
It is well established that malnutrition in an intensive care setting leads to muscle wasting, reduced function, impaired wound healing, increased risk of pressure injuries and increased length of stay. 1 Individuals with higher BMI may not be prioritised for nutritional support due to the assumption that their body fat proportions suggest good nutritional status. A previous audit at an ICU with 13 Level 3 beds in a hospital in South East England showed that time until enteral or parenteral feeding was not statistically significantly different between obese and non-obese patients. However, there were individual cases where feeding had been delayed without clear clinical rationale for patients with high BMI. These findings were consistent with another study that demonstrated that malnourished obese hospitalised patients were less likely to receive additional nutrition support than lower weight peers. 2 An audit was therefore undertaken in our local hospital to assess the proportion of individuals with body-mass index >25 kg/m2 who were malnourished on admission to ICU.
Objective
To assess nutritional status and malnutrition risk of non-elective individuals admitted to ICU with BMI > 25 kg/m2.
Methods
All non-elective admissions to ICU between 1st April 2022 and 30th June 2022 underwent a baseline dietetic assessment within 48 h of admission. Dietitians recorded participants’ weight, height, BMI, weight history and diet history from the past 2 weeks.
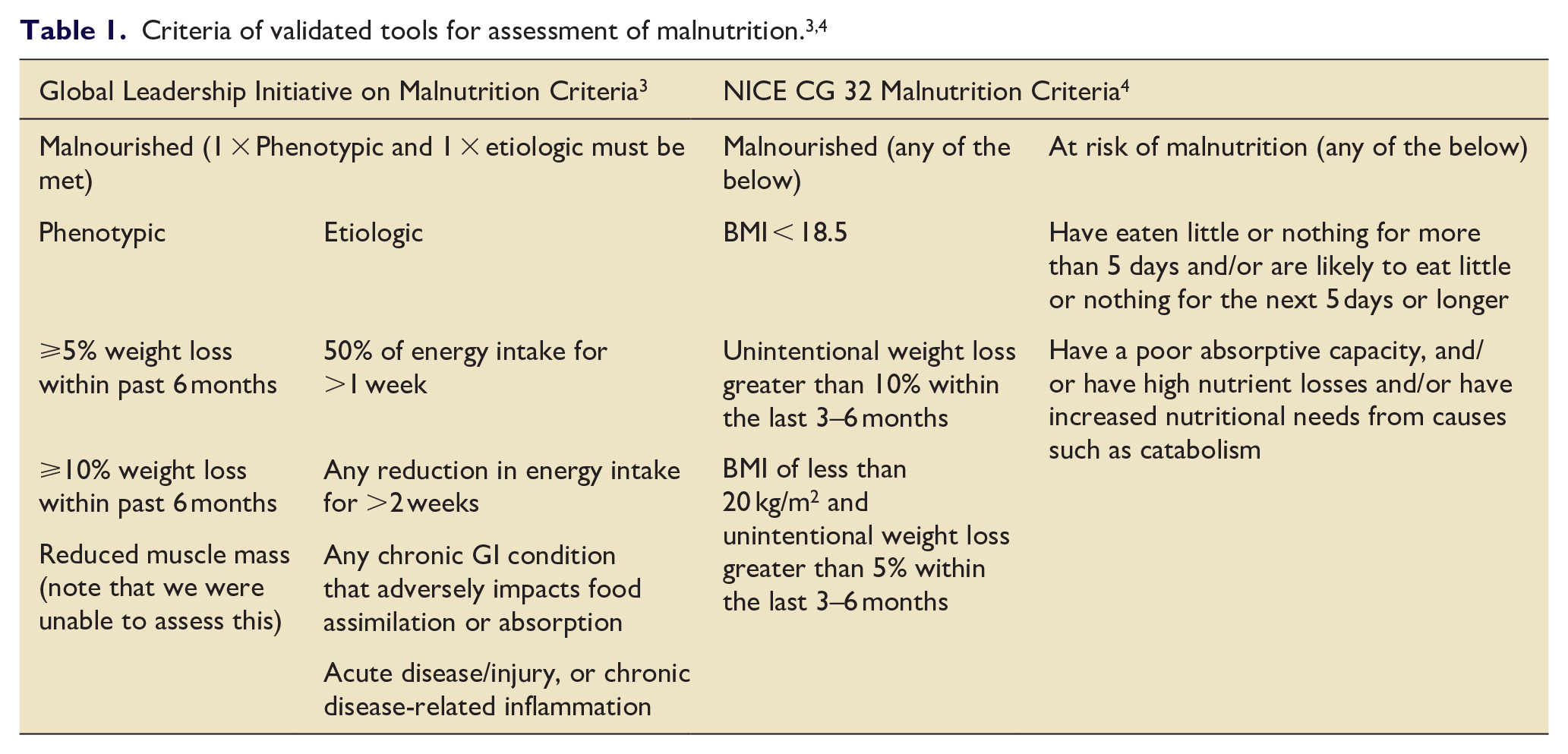
Participants with BMI > 25 kg/m2 were screened for malnutrition and risk of malnutrition, using the Global Leadership Initiative on Malnutrition (GLIM) criteria and NICE Clinical guideline [CG32] criteria (Table 1).3,4 These screening tools were chosen due to ease of use and inclusion of both etiologic and phenotypic criteria. The Nutrition Assessment in Critically Ill (NUTRIC) score was not used, despite being developed specifically for ICU patients, as this score assesses nutritional risk during stay, rather than pre-existing malnutrition. 5
Results
Forty-five patients were identified for analysis, with 3 excluded due to incomplete data. Average BMI was 30.4 kg/m2 (range 25.0–56.7 kg/m2).
GLIM criteria assessed 71% of participants as ‘malnourished’. NICE Clinical guideline [CG32] assessed 78.5% as ‘at risk of malnutrition’ and 9.5% as ‘malnourished’.
Discussion
This audit identified that a high proportion of individuals with a BMI > 25 were either malnourished or at risk of malnutrition on admission to ICU. Conventional opinion states that overweight and obese individuals should be well nourished, however our findings have not supported this assumption.
Two different validated tools were used to assess malnutrition. The proportion of ‘malnourished’ individuals was very low with the NICE criteria (9.5%) which is unsurprising as this is a very weight-centric measure of nutrition which still relies heavily on BMI. This may reduce its relevance in an ICU setting where BMI and weight changes are often un-reliable due to rapid fluid shifts. However, most individuals audited did meet NICE criteria for ‘risk of malnutrition’ (78.5%). The GLIM criteria is a more varied assessment, including a nutritional assessment and taking in to account clinical condition. This resulted in a much higher proportion of individuals being classified as malnourished (71%).
This audit demonstrated that BMI alone is a poor indicator of nutritional status in ICU patients and therefore challenges the weight biased impression that overweight and obese patients are well nourished and are in less need of nutrition support. It highlights the need to improve the equity of nutritional care for patients across the weight spectrum as previous studies have shown that this patient group is frequently overlooked. 2 Results also support ESPEN guidance stating that every critically ill patient staying for more than 48 h in the ICU should be considered at risk for malnutrition, 6 and be provided with timely and equitable nutrition support regardless of body weight.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Applied Research Collaborative Kent, Surrey, Sussex Individual Development Awards Scheme.