
Abstract
Purpose
Prolonged bed rest and immobility in the intensive care units (ICU) increase the risk of ICU-acquired weakness (ICUAW) and other complications. Mobilisation has been shown to improve patient outcomes but may be limited by the perceived barriers of healthcare professionals to mobilisation. The Patient Mobilisation Attitudes and Beliefs Survey for the ICU (PMABS-ICU) was adapted to assess perceived barriers to mobility in the Singapore context (PMABS-ICU-SG).
Methods
The 26-item PMABS-ICU-SG was disseminated to doctors, nurses, physiotherapists, and respiratory therapists working in ICU of various hospitals across Singapore. Overall and subscale (knowledge, attitude, and behaviour) scores were obtained and compared with the clinical roles, years of work experience, and type of ICU of the survey respondents.
Results
A total of 86 responses were received. Of these, 37.2% (32/86) were physiotherapists, 27.9% (24/86) were respiratory therapists, 24.4% (21/86) were nurses and 10.5% (9/86) were doctors. Physiotherapists had significantly lower mean barrier scores in overall and all subscales compared to nurses (p < 0.001), respiratory therapists (p < 0.001), and doctors (p = 0.001). A poor correlation (r = 0.079, p < 0.05) was found between years of experience and the overall barrier score. There was no statistically significant difference in the overall barriers score between types of ICU (χ2(2) = 4.720, p = 0.317).
Conclusion
In Singapore, physiotherapists had significantly lower perceived barriers to mobilisation compared to the other three professions. Years of experience and type of ICU had no significance in relation to barriers to mobilisation.
Introduction
The general muscle weakness that develops over the course of an intensive care admission, for which no other causes can be identified besides the acute illness or its treatment, is labelled “intensive care units acquired weakness (ICUAW)”. 1 ICUAW is estimated to be present in 40-46% of intensive care units (ICU) patients,2,3 with clinical features include proximal and/or distal flaccid impairment of the diaphragm and the neuromuscular system. Such impairment may consist of general weakness, reduced deep tendon reflexes, compromised pain, temperature and vibratory senses.4,5 De Jonghe et al. (2007) reported that 75% of patients were presented with diaphragmatic dysfunction after seven days of mechanical ventilation. 6 Other longitudinal studies documented the persisted functional deficits reflected by the six-minute walking distance of ICU survivors for up to twelve months post-ICU discharge.7,8
Early mobilisation, defined as the application of physical activity as early as the second to the fifth day after the onset of critical illness or injury, has been shown to reduce the incidence of ICUAW at the point of ICU or hospital discharge, improve patients' unassisted walking distance, and to decrease the overall length of stay at ICU, hospital and rehabilitation facilities.9–13 Despite the convincing evidence, the practice of early mobilisation among ICU healthcare workers appears to be low.11,13–15 Haemodynamic instabilities with medical contraindications, delirium and deep sedation, pain and fatigue are the most commonly-cited patient-related barriers to mobilisation.9–11,14,15 The lack of mobility culture or staff buy-in within certain ICUs,11,16 poor interprofessional communication and time constraints further compounded the acceptance. 9 Additionally, the level of specialty training and years of clinical/ICU experience, and nurse-to-patient ratios are some of the factors that could influence early mobilisation in the ICU. 17
Factors such as different healthcare professions, years of ICU experience and the ICU settings impact the prevalence of early mobilisation.14,16,18,19 Thus far, no study has explored the barriers to early mobilisation with ICU healthcare professionals in Singapore. This study aimed to identify the perceived barriers to early mobilisation in ICU and to evaluate potential differences in perceived barriers between (1) different acute hospitals with ICU, (2) ICU types, (3) clinical roles, and (4) to evaluate the association between years of experience and perceived barriers.
Methods
Following the CROSS guidelines, 20 this cross-sectional self-administered survey recruited participants via purposive sampling from the ICU teams of all local acute hospitals. The University Review Board granted ethical approval, number: 2020029. Data collection happened between April 2020 to January 2021. Consent was implied when participants returned the completed questionnaires. No financial reimbursement was offered to participants.
Survey instrument
The Patient Mobilisation Attitudes and Beliefs Survey (PMABS) was developed to identify critical barriers to mobilising medical inpatients in the acute hospital settings (overall internal consistency Cronbach’s alpha (α) = 0.87, 95% CI 0.83–0.90). 21 The PMABS for the ICU (PMABS-ICU) was subsequently adapted and validated to the ICU context (overall internal consistency α = 0.82, 95% CI 0.76–0.85). 18 With permission from Goodson et al. (2020), this study utilised the PMABS-ICU with minor modifications to the terminologies and included additional demographic questions to the PMABS-ICU for Singapore (PMABS-ICU-SG) to meet the study objectives. The minor modifications were made to increase the survey applicability to the local context, and these include: “physician to doctor”, “physical therapy to physiotherapy”, “physical therapist to physiotherapist”. Additional demographic questions are: “Please specify your training level.”, “Which hospital do you work in?”, “Which ICU do you work in?” and “Please specify the number of years you have spent caring for ICU patients.” There was no modification to the 26-validated statements of the PMABS-ICU to PMABS-ICU-SG. Like the PMABS and PMABS-ICU, the PMABS-ICU-SG consists of three subscales: knowledge, attitudes, and behaviours. The knowledge subscale assesses healthcare professionals’ education and training relevant to mobilising patients and appropriately referring patients for rehabilitation services. The attitudes subscale assesses healthcare professionals’ lack of self-efficacy, outcome expectancy and agreement, and perception of other healthcare providers' attitudes. The behaviour subscale assesses practice pattern limitations that may inhibit the mobilisation of patients. Items were alternated between positively and negatively connotated wordings to avoid response set bias. A 5-point Likert scale (1 = strongly disagree; 2 = disagree; 3 = neutral; 4 = agree; 5 = strongly agree) was used to obtain responses. With Items 1, 3, 4, 7, 10, 12, 13, 15, 17, 19, 21 and 23, the reversed 5-point Likert scale (5 = strongly disagree; 4 = disagree; 3 = neutral; 2 = agree; 1 = strongly agree) was used instead.18,21 The PMABS-ICU-SG scoring system is consistent with the PMABS-ICU. Respondents’ overall perceived barriers and subscale scores ranged from 0 to 100, with higher scores indicating more significant barriers to mobility. Respondents were required to specify their professions, years of ICU experience, hospital of employment, and type of ICU they worked. A free-text response was included to identify other issues related to mobilisation.
Survey population
Invited respondents included healthcare professionals working in the cardiac or coronary care ICU, cardiothoracic ICU, medical ICU, multidisciplinary ICU, neuroscience ICU, and surgical ICU. The eleven hospitals surveyed were Alexandra Hospital, Changi General Hospital, Khoo Teck Puat Hospital, Mount Elizabeth Hospital, Mount Elizabeth Novena Hospital, National Heart Centre, National University Hospital, Ng Teng Fong General Sengkang General Hospital, Singapore General Hospital, and Tan Tock Seng Hospital. Inclusion criteria included: healthcare workers (medical doctors, nurses, physiotherapists and respiratory therapists) who were presently on ICU posting regardless of years of ICU experience, while the study excluded other healthcare professionals that are not involved in the decision making of patients mobilisation in ICU. Respondents indicated their clinical role from one of the four available options. There was no pre-determined sample size, as there is no census on the number of healthcare workers involved in ICU care in Singapore. All responses and databases were kept encrypted, private and confidential with unique anonymised personal identifiers that were only accessible by the researchers.
Data collection procedures
The invitation email to participate was disseminated via the physiotherapy departments of the hospitals for aid in further dissemination to the relevant ICU teams. The PMABS-ICU-SG was administered via Qualtric ®XM with a unique quick response code (QR code) to prevent multiple participation of the respondents. The demographic section of the online survey required non-mandatory completion, while respondents must have completed all the 26 statements from the PMABS-ICU-SG before the submission function was available.
Statistical analysis
An accepted response to PMABS-ICU-SG was defined as having all 26 items answered. A survey with incomplete demographic information was still deemed acceptable with purposive sampling. Statistical analysis performed using IBM SPSS® Statistics ver. 26.0.0.1. The overall, knowledge, behaviour, and attitude subscale scores were tabulated with mean scores and standard deviation (SD). Free-text comments were categorised thematically. The Shapiro-Wilk test (p > 0.05) determined the normality of all data. Independent samples t-test and Mann-Whitney U tests compared the differences between each profession’s overall knowledge, behaviours, and attitudes subscale scores. Pearson correlation coefficient (r) determined the correlation between years of ICU experience and overall barriers score, with correlation coefficient > 0.7 deemed acceptable. One-way ANOVA determined the statistically significant differences in overall barriers score between ICU types. Post hoc Levene’s test did not find equal variance (p = 0.046); hence a Kruskal-Wallis H-test was conducted. Statistical significance was set at p < 0.05.
Results
Respondents
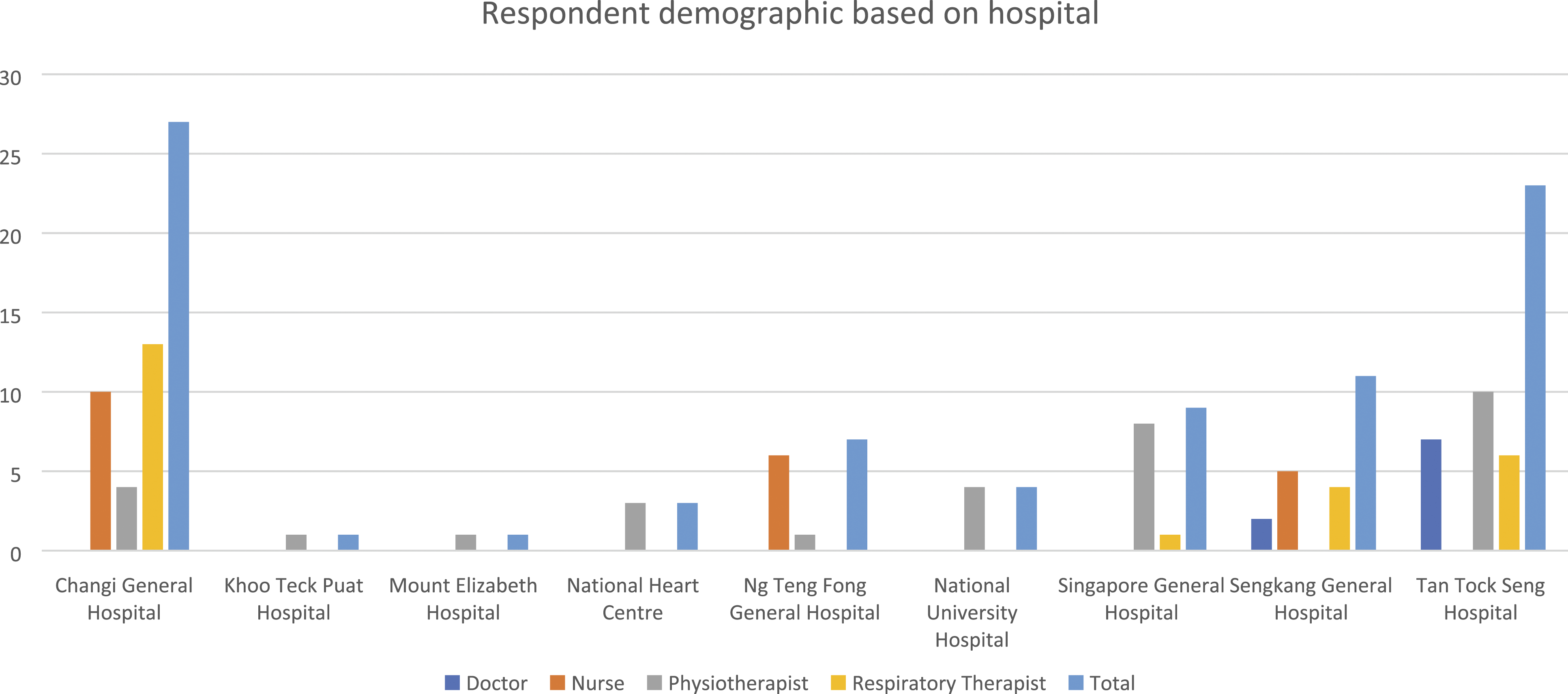
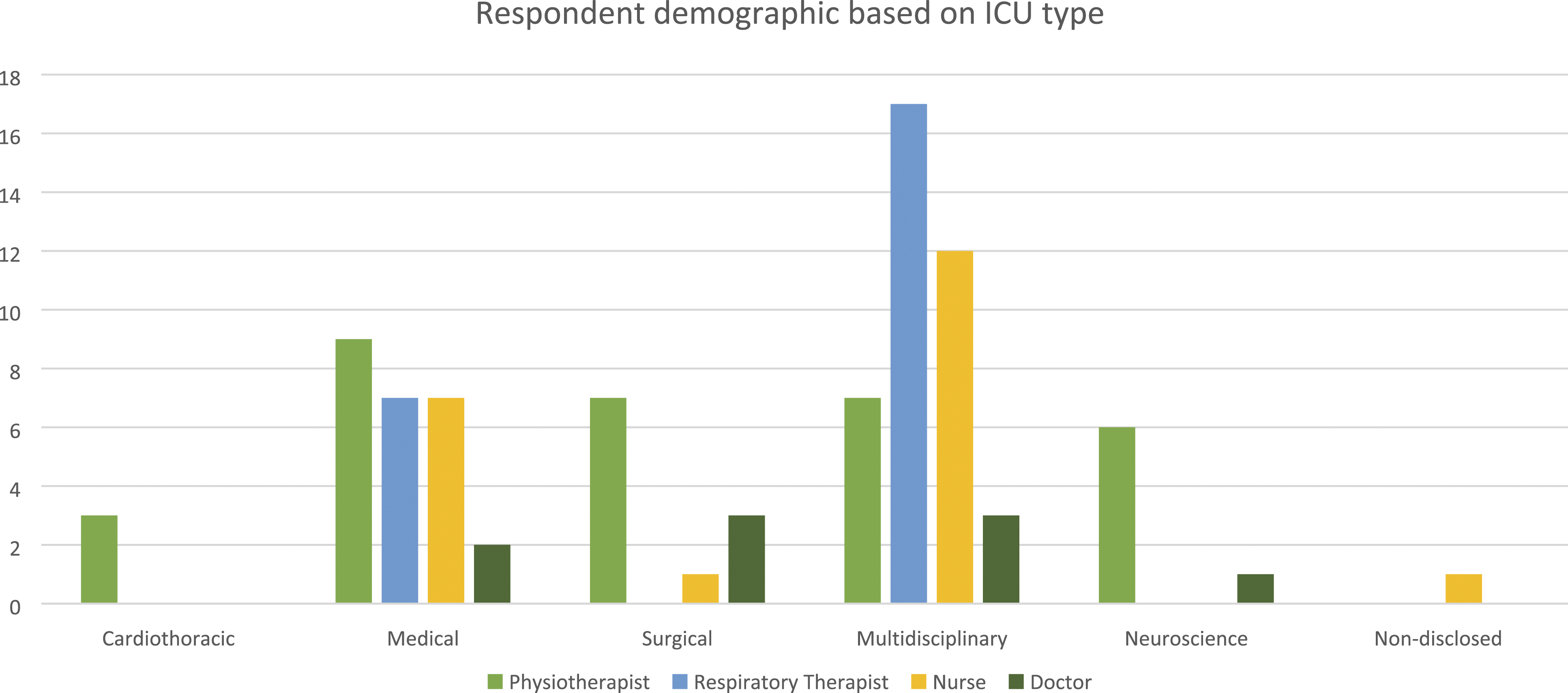
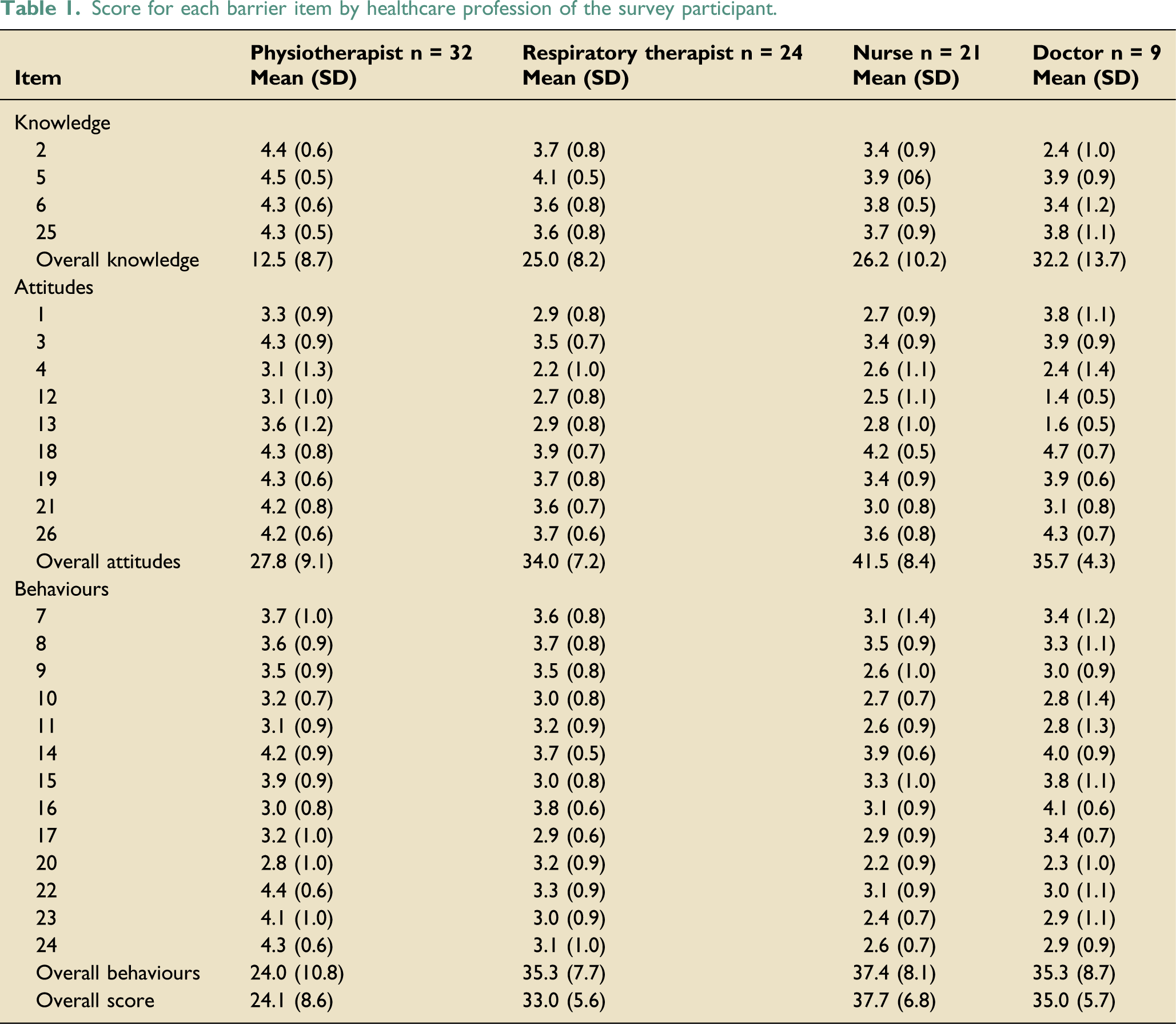
Data were analysed from the 86 completed responses from nine of the eleven hospitals, with no representation from Alexandra Hospital and Mount Elizabeth Novena Hospital. One respondent did not disclose the ICU setting of practice—no other missing data was found. Figures 1, 2, and 3 present the respondent demographics based on the healthcare profession, hospital, and ICU type. Tables 1 to 5 report the overall and subscale scores by healthcare professions and the score for each healthcare profession’s barrier item, respectively. The knowledge and attitude scores for physiotherapists and the attitude scores for respiratory therapists did not demonstrate a normal distribution, while the rest of the scores were normally distributed. Respondent demographic based on healthcare profession. Respondent demographic based on hospital. Respondent demographic based on ICU type. Score for each barrier item by healthcare profession of the survey participant. Statistical analysis of overall scores between all occupations. *p < 0.05.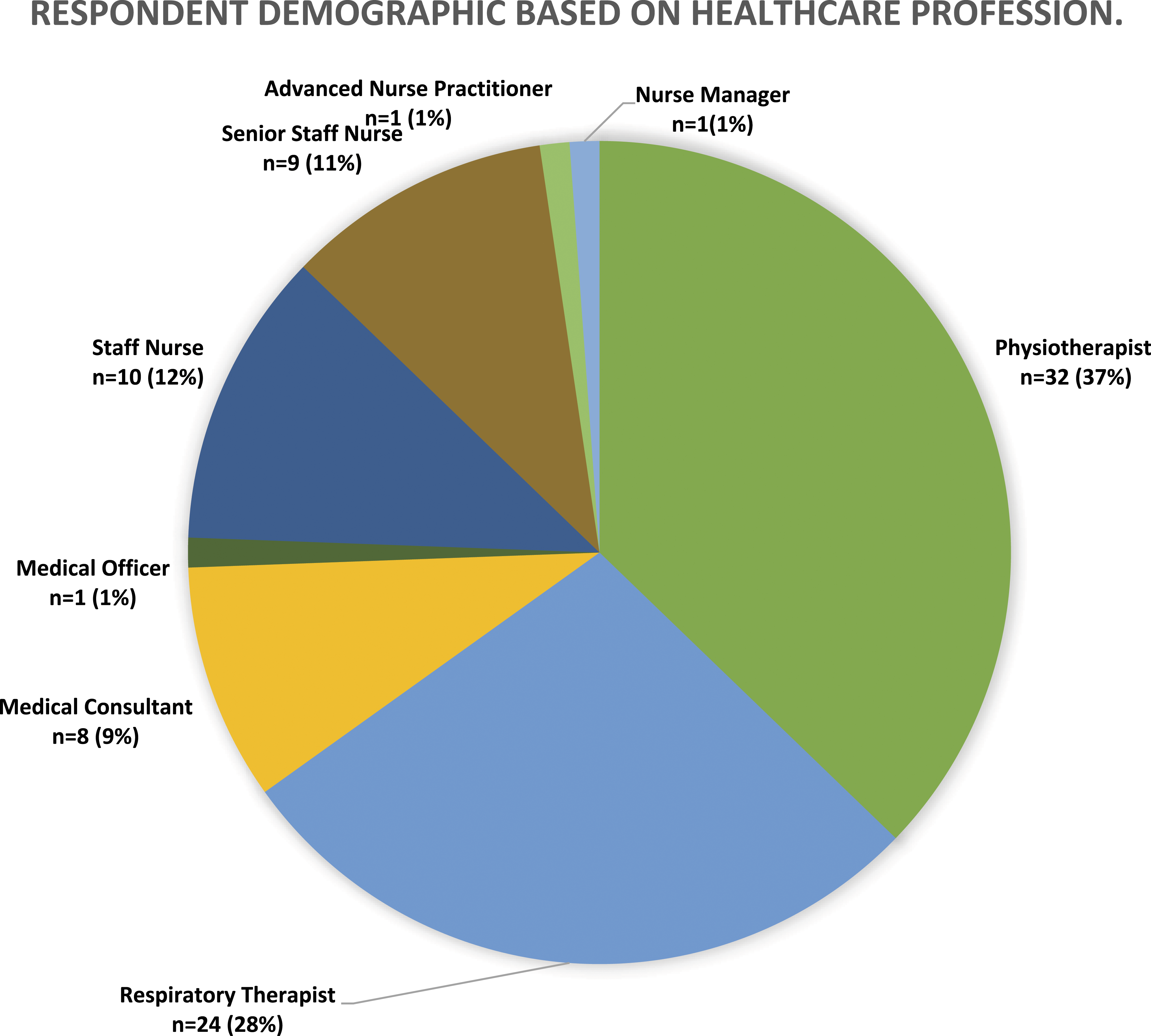

Barriers to mobilisation
Statistical analysis of knowledge scores between all occupations.

*p < 0.05.
Statistical analysis of behaviour scores between all occupations.

*p < 0.05.
Statistical analysis of attitudes scores between all occupations.

*p < 0.05.
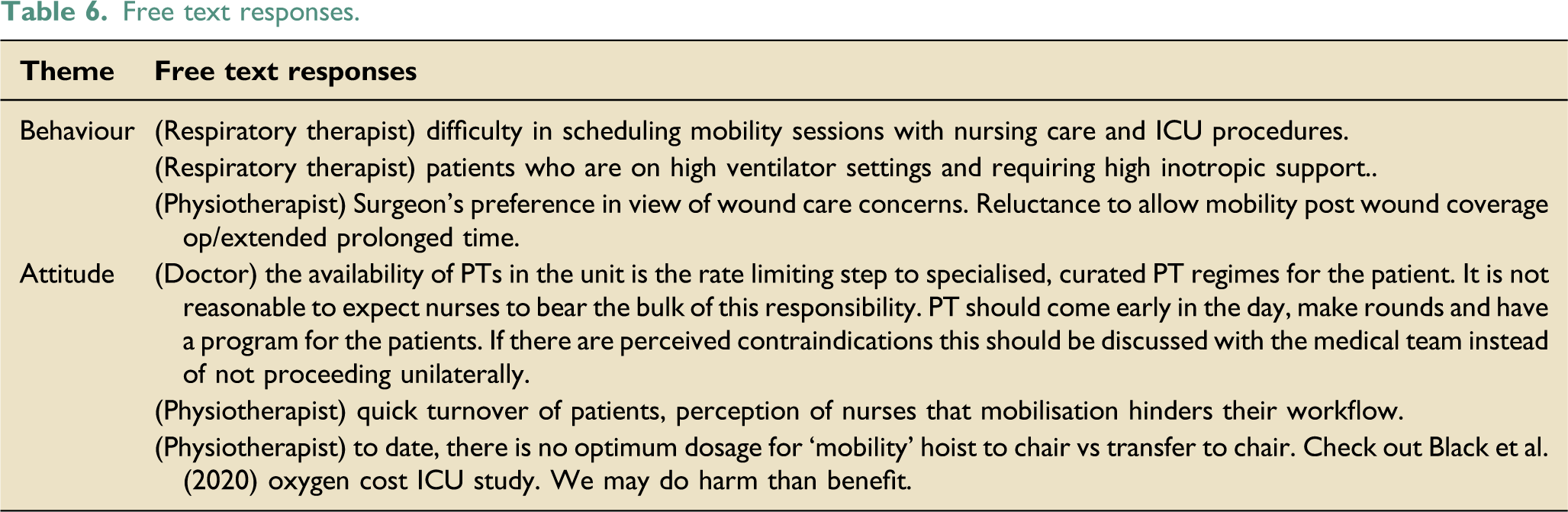
Free text responses.
Discussion
Overall barriers scale
Our study showed that physiotherapists had significantly lower scores in the overall, knowledge, behaviour, and attitude subscales of the PMABS-ICU-SG, indicating the lowest perceived barriers to mobilisation of patients in the ICU. This is consistent with current literature,9,11,18,21 particularly a survey on Australian ICU practices found that 94% of physiotherapists would routinely prescribe mobilisation exercises for ICU patients. 22 This result is unsurprising, given that mobilising patients is part of a physiotherapist’s daily clinical work.
Behaviour subscale
Nurses had the highest mean behaviour and attitude scores among all professions surveyed, consistent with the previous studies.9,11,18,21 On Item 10 (Table 1), nurses and doctors agreed patients might be perceived with medical contraindications that prevent mobilisation. Similar to Harrold et al. (2015), 23 our results reflect such a possible view. Nurses and doctors who perceive the patients are unstable may choose to enforce bed rest.13,24 Education on the low adverse event rate associated with mobilisation 25 and modification strategies to achieve increased mobilisation may be employed to overcome this barrier.
In items 11 and 24 (Table 1), both nurses and doctors felt that nurses or other healthcare professionals did not mobilise patients suitable for mobilisation. The outcomes affirm the presence of other non-patient-related barriers which hinder mobilisation. The attributions could be the lack of time (Item 23, Table 1), a common concern both profession shared, while the nurse-to-patient ratio was inadequate for mobilisation (Item 9, Table 1). This is unsurprising given the significant workload involved in ICU nursing care 26 ; and doctors have reported feeling overstretched as a frequent and severe stressor of working in the ICU. 27 Conversely, a lower nurse-to-patient ratio has been associated with increased early mobilisation in the ICU. 17 A more cost-effective solution could be a mobilisation protocol, which showed to reduce the proportion (33% to 6%) of staff citing inadequate staffing as a barrier to mobilisation. 13
Attitude subscale
Item 4 (Table 1) revealed that all, except physiotherapists, felt that physiotherapists should be the primary provider of mobilisation, while the physiotherapists were neutral to the statement. This sentiment is somewhat foreseeable, given that physiotherapists are most appropriately trained to fulfil this clinical role. 21 This further reflects the disparity in the expectations of clinical roles between ICU healthcare professionals. Existing literature has shown that unclear expectations and roles regarding mobilisation can pose a barrier to mobilisation, as ICU healthcare professionals may perceive the responsibility of mobilisation to fall on the shoulders of other professions. 24 Item 12 (Table 1), all professions, except physiotherapists, agreed that increased mobilisation equated to a greater workload for nurses due to the nature of the role, such as coordination of medical care, attachment management, and drug administration monitoring. Mobilisation has been viewed as the cause of prolonged working hours by 47% of the nurse respondents. 24 This issue is expected due to the competing priorities, 21 or the lack of assistive mobility devices and inadequate staffing. 13 Future studies can explore the underlying reasons hindering nurses from engaging in more early mobilisation.
ICU types and years of experience
This study reported a negligible correlation between years of experience and barriers to mobilisation, contrary to a similar survey conducted in the USA. 18 One study demonstrated the effectiveness of a mobilisation protocol on increasing mobilisation in Singapore’s ICU, 13 which suggests a preeminence of protocol over years of experience within local ICU. Another reason may be the culture of continuing education, which involves regular interdisciplinary ward rounds and case discussions among ICU professionals, a recommended strategy to overcome barriers to inadequate experience in mobilising patients.28,29 Hence, years of experience was not found to be a significant barrier to mobilisation in Singapore’s ICU.
Free-text responses
Behaviours and attitudes were the themes that emerged in the free-text component. The behaviour theme assesses preferential constraints and external factors affecting patient mobilisation. One respiratory therapist expressed “(the) difficulty in scheduling mobility sessions with nursing care and ICU procedures”. Given the high volume and frequency of ICU procedures, this concern was foreseeable. Undoubtedly, mobilisation can be time-consuming, given the use of many life-supporting devices. However, this is modifiable if coordinated with clear communication and operational planning. 30 Another respiratory therapist cited “patients who are on high ventilator settings and requiring high inotropic support” as an issue that prevents mobilisation. Furthermore, one physiotherapist mentioned that the “surgeon’s preference given wound care concerns'' and “reluctance to allow mobility post-wound coverage operation/extended prolonged time” would prevent mobilisation. These comments demonstrated the rationale of medical contraindications for early mobilisation, consistent with Item 10 from the behaviour subscale. Specifically, such examples illustrated the need for future quality improvement projects.
The attitudes theme assesses a provider’s lack of self-efficacy, outcome expectancy and agreement, and perception of other healthcare providers' attitudes. One doctor stated that “the availability of physiotherapists in the unit is the rate-limiting step to specialised, curated physiotherapy regimes for the patient. It is not reasonable to expect nurses to bear this responsibility. Physiotherapists should come early in the day, make rounds, and have a program for the patients”. This resonated with the fact that physiotherapists should be the primary healthcare professional who mobilises patients, not nurses, consistent with Item 4.
One physiotherapist stated that the “perception of nurses that mobilisation hinders their workflow” is the reason for the lack of mobilisation in the ICU, corresponding to Item 12. This comment implies that physiotherapists expect nurses to assist in mobilising ICU patients, despite the overwhelming ICU nursing roles, further complicated the perceived insufficient staffing. Additionally, another physiotherapist stated that “to date, there is no optimum dosage for ‘mobility’ hoist to chair vs transfer to chair” and that “we may do (more) harm than benefit”, fitting the sentiment in Item 3. Although the evidence supports early mobilisation, this comment suggests a lack of studies identifying the ideal amount of mobilisation for different patient demographics. Prescription of mobilisation cannot be one-size-fits-all, but it may be beneficial for healthcare professionals to follow guidelines or standard protocols for safe and effective practice.
Limitations
The variety of ICU types surveyed may potentially skew or neutralise the findings. 39 (45.3%), 25 (29.1%), and 7 (8.1%) respondents represented the multidisciplinary, medical and neuroscience ICU perspectives, respectively. The medical stabilities of patients from these ICU could vastly differ from those at the cardiothoracic (3.5%) or surgical ICU (12.8%). Given the relatively small sample size, this study could not provide further insight into the specific nature of different barriers to early mobilisation in different ICU types. Result comparisons with other studies are limited due to the heterogeneity of the reported study designs. Current evidence largely comprises cohort studies that surveyed either the point-prevalence of perceived barriers,14,17,23,24 or the qualitative responses of healthcare professionals. 16 In addition, the survey distribution (via physiotherapy departments) may have caused a positive selection bias towards physiotherapists and a lower response rate from other professions. Also, the online survey form without the “save” functions could dissuade keen participants from contributing to the study as it would have been tedious to restart the survey if the previous attempt was incomplete. More importantly, the survey period coincided with a peak in the local COVID-19 pandemic, when many healthcare professionals in the ICU were occupied with managing critically-ill patients, which may have detracted from their availability and willingness to complete the survey. The infection-control restrictions and newly-laid protocols greatly impacted patient management guidelines. Responses could have been affected or even compromised by changes in workflow and practices during the pandemic, potentially proving a deterrent to mobilisation, which requires physical space. The readiness and timeliness to initiate early mobilisation could also have been impeded by the deployment constraints of staffing and transfer aids, such as the hoist. This time-factor and recency effect may have influenced the perception and willingness for early mobilisation and potentially biased these survey findings. The PMABS-ICU-SG also has potential limitations in comprehensively measuring all perceived barriers. This was evident from the literature review and free-text question, which raised multiple patient-related perceived barriers that were not addressed in the survey. A follow-up qualitative study that further identifies other barriers and their contributing factors in our healthcare settings may be considered to elucidate these issues.
Conclusion
Two major barriers to patient mobilisation in ICU have been identified through this study. Firstly, concerns about the safety of early mobilisation in contraindications and medical instability contribute significantly to the unwillingness to mobilise patients in the ICU. Secondly, there is some discrepancy in the expectations of healthcare professionals responsible for mobilising patients. This study sheds light on key differences in the perceptions of different healthcare professionals. As the literature moves from merely identifying perceived barriers to investigating suitable interventions, future local quality improvement projects should extrapolate this study’s results to formulate evidence-based solutions.
Supplemental Material
Supplemental Material - Perceived barriers to mobility in the intensive care units of Singapore: The Patient Mobilisation Attitudes and Beliefs Survey for the intensive care units
Supplemental Material - Perceived barriers to mobility in the intensive care units of Singapore: The Patient Mobilisation Attitudes and Beliefs Survey for the intensive care units by Meredith T Yeung, Nicholas K Tan, Gideon Z Lee, Yuemian Gao, Chun Ju Tan and Clement C Yan in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.