
Abstract
The COVID-19 pandemic has brought with it a large number of challenges for healthcare professionals including intubation safety in out-of-theatre environments. An important aspect of this topic is the optimisation of a patient’s head and neck position prior to laryngoscopy which can be challenging when a pillow cannot be located. As a result, the authors compared how well the sniffing position (35o neck flexion and 15o head extension) could be reached using pillows or other novel head supports. The resulting data demonstrated that a 1-litre pressure bag and two 1-litre saline bags achieved the most accurate position.
Introduction
The COVID-19 pandemic has brought with it a large number of challenges for healthcare professionals to address. One aspect of care that anaesthetists and intensivists have tried to deliver safely is the intubation of those who are critically unwell in out-of-theatre locations. The fourth national audit project by the Royal College of Anaesthetists 1 demonstrated that these areas pose a higher risk of anaesthesia-related major airway complications compared to within theatres. As a result, consensus guidelines for emergency intubation in those with COVID-19 2 stress the need to optimise the chance of first-pass success to reduce risks to the patient and staff. These guidelines highlight airway positioning as a key part of the anaesthetic process, with unexpected difficult intubation schemas 3 emphasising the need to effectively manipulate and optimise the head and neck position if initial passes are unsuccessful. A commonly described optimal position for endotracheal intubation in a normal BMI patient is the sniffing position (SP). 4 This has previously been defined as neck flexion of 35o and head extension of 15o with the external auditory meatus aligned with the sternal notch.5,6
Despite a great importance being placed on airway positioning during intubation, the authors found that they had previously had great difficulty finding pillows to help facilitate this position in the emergency department (ED). This had led to suboptimal head support usage (e.g. folded blankets), resulting in failed intubations. This issue was resonated by other authors who found that even when locating a pillow, its quality was unsuitable for positioning. 7 As a result, the authors compared the SP achieved by folded blankets and pillows in one NHS trust with the equivalency of other potential head supports that are commonly available in the ED. The aim of this project was to improve patient safety through the identification of areas for further equipment research to reduce the risk of major airway complications in out-of-theatre environments.
Methods
An examination of the authors’ ED was conducted to identify items that could be used to gently support an individual’s head to achieve the SP during intubation. Each item was used to position one author (normal BMI) as close to the combined angles of the SP as possible. Photographs were taken of each position with anatomical landmarks used to calculate the degree of neck flexion and head extension achieved. The sternal notch–thyroid cartilage angle relative to the author’s horizontal plane was used to define the angle of neck flexion. The mental protuberance-zygoma angle relative to the author’s horizontal plane was used to define the angle of head extension. Each set of angles were compared to the defined SP angles of 35o neck flexion and 15o of head extension.
Results
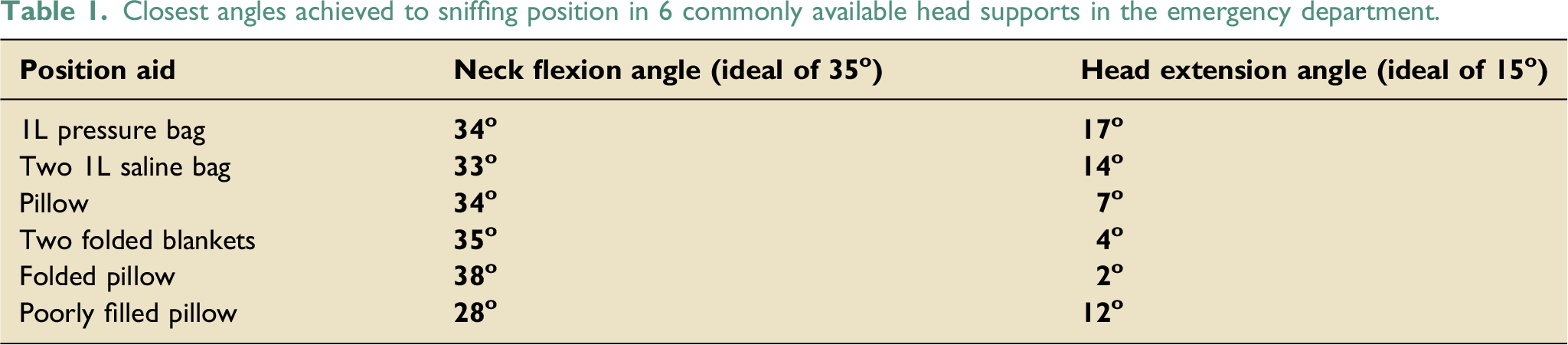
Figure 1 demonstrates the authors’ photographic assessments of pillows, blankets and the two novel pieces of equipment that most accurately achieved the defined angles (a 1-litre pressure bag and two 1-litre saline bags). The results of the individual angle measurements are shown in Table 1. Photos used for head and neck angle analysis. The first photo illustrates the anatomical planes used to calculate these angles. Blue line = Mental protuberance - zygoma plane (Head extension), Red line = Sternal notch - thyroid cartilage plane (Neck flexion), Green line = Horizontal plane. Closest angles achieved to sniffing position in 6 commonly available head supports in the emergency department.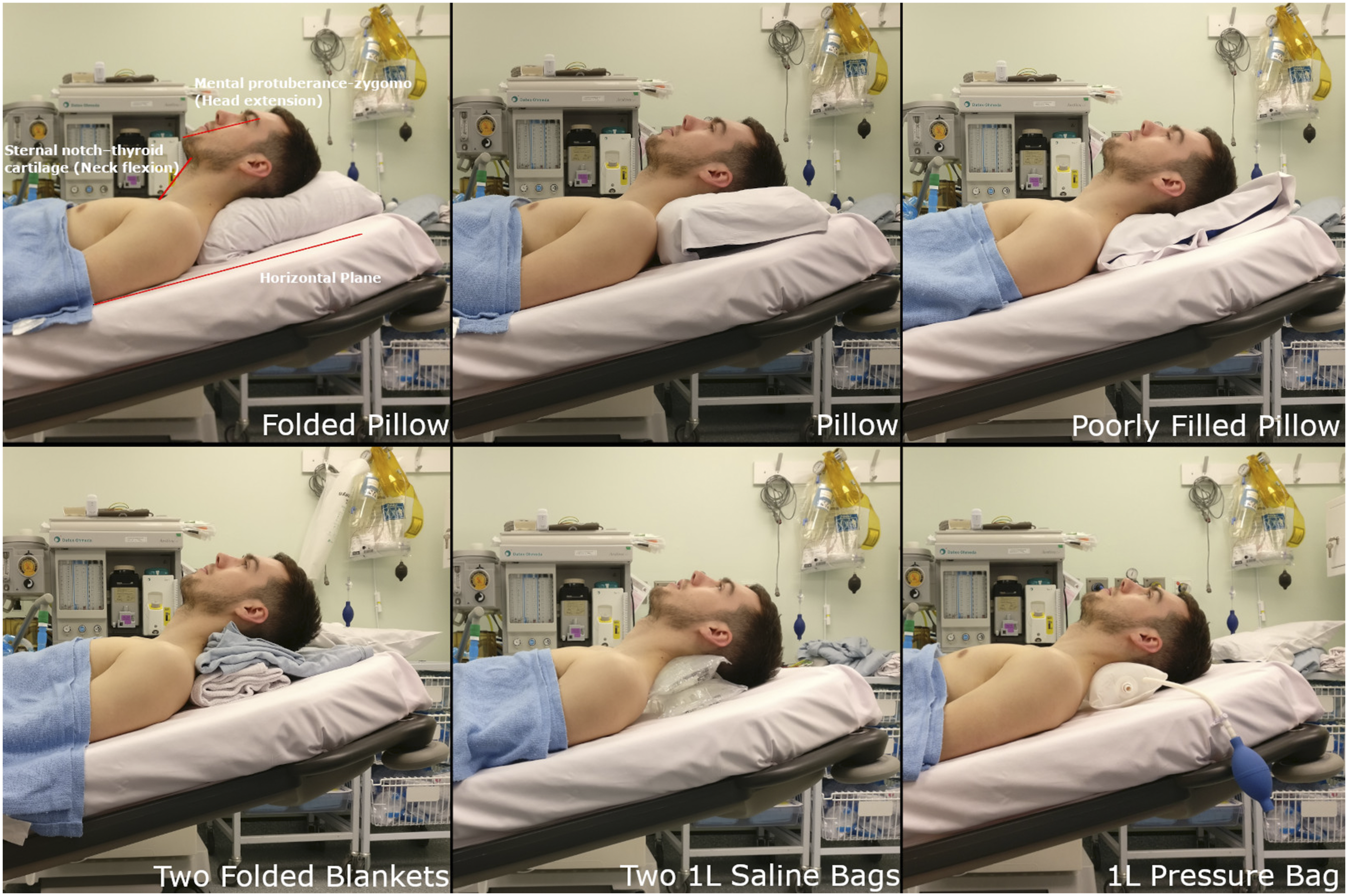
Discussion
Although the pillows and blankets consistently achieved close to 100% of the target neck flexion with the exception of the poorly filled pillow, none facilitated > 47% of the target head extension. In contrast, both novel head supports achieved > 94% of target flexion and > 93% extension. This led to the conclusion that although many of these items were capable of flexing the neck sufficiently, only the pressure bag and saline bags were able to balance this with sufficient extension of the head to align the laryngeal, pharyngeal and mouth axis.8,9 In addition, of all of the supports reviewed, the pressure bag was noted by the authors to be the most versatile as it could be easily positioned behind an unresponsive individual’s neck whilst deflated, with inflation subsequently leading to a highly adaptable variation in position.
In conclusion, this preliminary data suggested that a 1L pressure bag or two 1L saline bags may optimise airway position to reduce the risk of major airway complication during the intubation of a critically unwell COVID-19 patient when no pillow is available. This is currently a topic of great importance as the risk of intubation in patients presenting late in this cohort remains high. 10 It is for this reason that the authors would urge readers to consider the role of novel head supports in the optimisation of airway management in emergency situations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.