
Abstract
Background: Bandemia, defined as a band count >10%, is indicative of underlying infection and is increasingly being used for early detection of sepsis. While an absolute band level has been linked to worse outcomes, its trend has not been extensively studied as a prognostic marker. In this study, we assessed patients admitted to the ICU with sepsis or septic shock and evaluated the correlation between bandemia trends and clinical trajectory among these patients.
Methods: This study was a retrospective chart review. Band counts, serum lactate levels, and SOFA scores at 0 and 72 h after admission to the ICU were collected. Patients were risk stratified into groups depending on their SOFA trends, and corresponding band trends and serum lactate levels were compared.
Results: 134 patients were included for analysis. There was a statistically significant decrease in bandemia trends for patients with a reduction in SOFA scores [median (IQR)−4.5 (−11, 0); p < 0.0001], and a statistically significant increase in bandemia trends for patients with worsening SOFA scores [median (IQR) 4 (0, 8); p = 0.0007].
Conclusion: Early trends of serum band levels in patients with sepsis or septic shock may help to predict a clinical trajectory and overall prognosis. More investigation is warranted as to whether incorporating bandemia trends, when used in conjunction with other known markers such as lactate levels, may help to guide bedside clinical decisions such as risk stratification, tailored therapies, and ultimately improve outcomes.
Keywords
Introduction
Sepsis is a leading cause of death in the United States despite advancements in early recognition and prompt treatment.1,2 Early identification, subsequent risk stratification and immediate management is known to improve survival in this patient group. 3 Ongoing prognostication however is limited, especially in the intensive care unit (ICU). Logic would therefore dictate that the availability of additional clinical data that promptly and accurately predicts the trajectory of critical illness may influence bedside treatment decisions and ultimately improve outcomes.
Currently, the gold standard biomarker used to guide therapy that correlate
Bandemia occurs as a result of bone marrow stimulation caused by an infection’s ability to induce the production of cytokines, 6 and is defined as newly synthesized and immature leukocytes greater than 10% relative to a pool of leukocytes. 3 The presence of elevated bands has already demonstrated utility in the initial diagnosis of sepsis, as absolute bandemia has been shown to correlate with the presence of serious infection in both the ICU and ED settings.7,8 Furthermore, recent studies have shown that in-hospital mortality rates are significantly elevated in patients presenting with severe bandemia. 9
While the absolute presence of bandemia has been linked to worse outcomes, the trend of bandemia in the ICU setting is yet to be studied. We hypothesized that bandemia trends could be used to track the clinical course of septic shock. That is, bandemia would trend as a clinical correlate: as bandemia resolves, so too do the clinical manifestations of sepsis dissipate. Conversely, failure to clear bandemia should correlate with the persistence of infection, poor prognosis and thus, increased mortality.
Materials and Methods
A retrospective chart review was conducted at the George Washington University Hospital Intensive Care Unit (ICU), a 48-bed unit caring for medical, surgical, trauma, and neurosurgical patients. The hospital’s electronic health record, Cerner (Cerner Corp, Kansas, MO), was used to collect data for the study. The study was approved by the Institutional Review Board of George Washington University.
From January 1, 2016 to May 31, 2019 all ICU patients over 18 years of age who were admitted directly from the Emergency Department (ED) with a diagnosis of sepsis or septic shock were included. Patients without a manual differential on their full blood count, and patients who had another documented diagnosis that could account for an elevated level of bandemia were excluded from the study. Patients who died or were discharged within 72 h of admission were also excluded. Diagnoses with other reasons for bandemia and thus excluded from analysis included myelodysplastic syndromes or disorders, acute inflammatory disorders, blood neoplasms and chronic medication with neutrophilic left-shift side effects such as glucocorticoids.
Bandemia (percentage), sequential organ failure assessment (SOFA) score and lactate level data points were collected at hour 0 on presentation and again at 72 h. Patients were divided into four groups based on their SOFA score trends: • Group 1: initially high SOFA score (≥6) that decreased at 72 h • Group 2: consistently high SOFA score (≥6) • Group 3: initially low SOFA score (<6) that increased at 72 h • Group 4: consistently low SOFA score (<6)
Corresponding bandemia and lactate levels were expressed as fractional change between initial presentation and 72 h.
Demographics, clinical characteristics, proportion of SOFA score groupings, bandemia percentages, and lactate measures were reported as descriptive statistics using frequency (percentage), mean ± standard deviation, and/or median (interquartile range). Bandemia percentage and lactate measure differences between start and 72 h were compared by SOFA score groupings with the Wilcoxon signed-rank test. Spearman’s rank correlation coefficient, ρ, was used to show correlations between lactate differences and bandemia percentage differences for each SOFA group, as well as for overall SOFA differences. Corresponding p-values (P) were presented and a two-sided p less than 0.05 was considered statistically significant. All statistical analysis was performed using SAS version 9.4 (SAS Institute Inc., Cary, NC).
Results
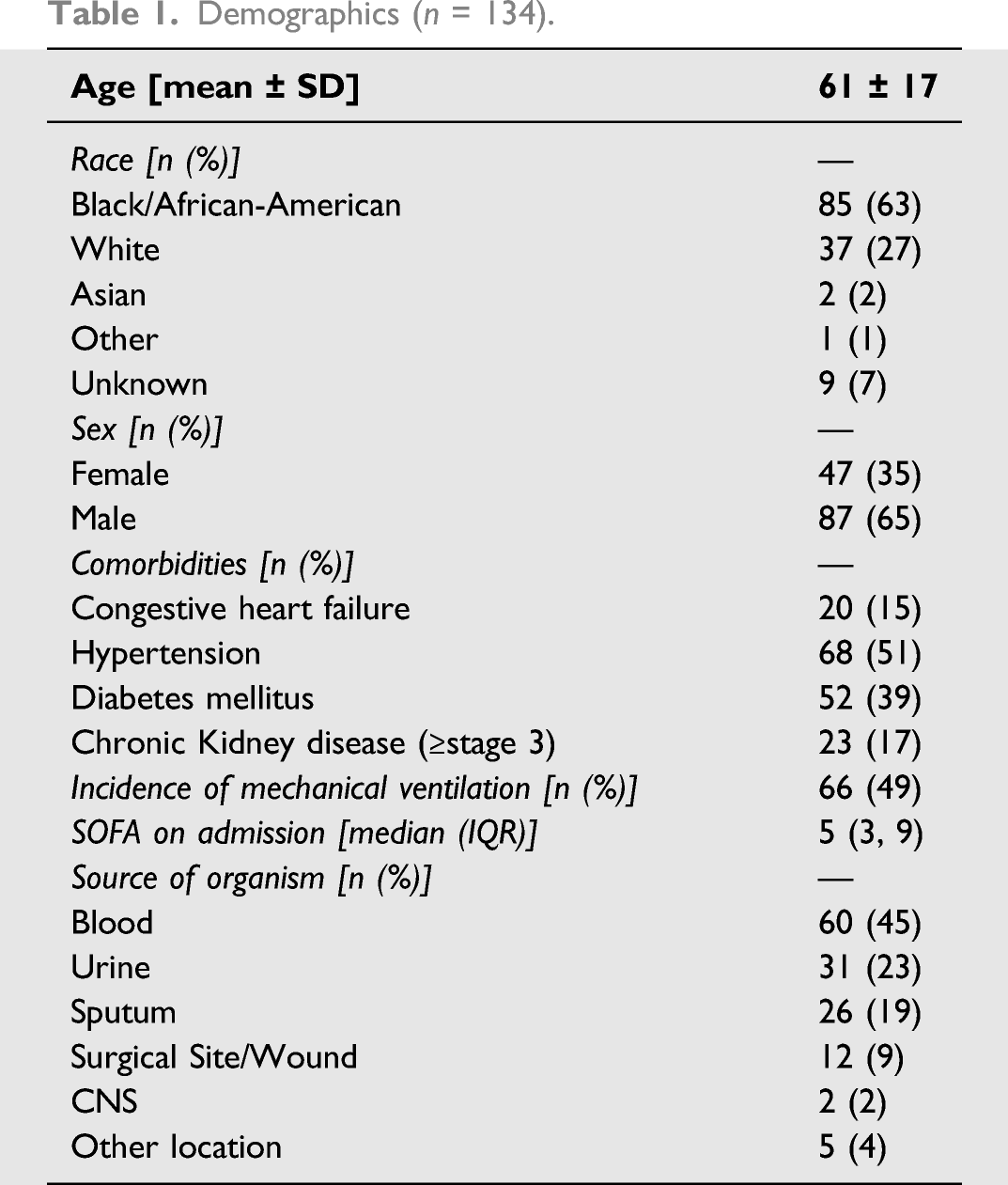
A total of 134 patients were identified for analysis over the study period (Figure 1). The mean age of the patients was 61 (SD 17) years. 63% of the patients identified as black, and 65% were male. The most common source of infection, apart from bacteremia at 45%, was urinary at 21%, followed by respiratory at 19%. Detailed demographic and clinical information are shown in Table 1. Flow chart of the study population. Demographics (n = 134).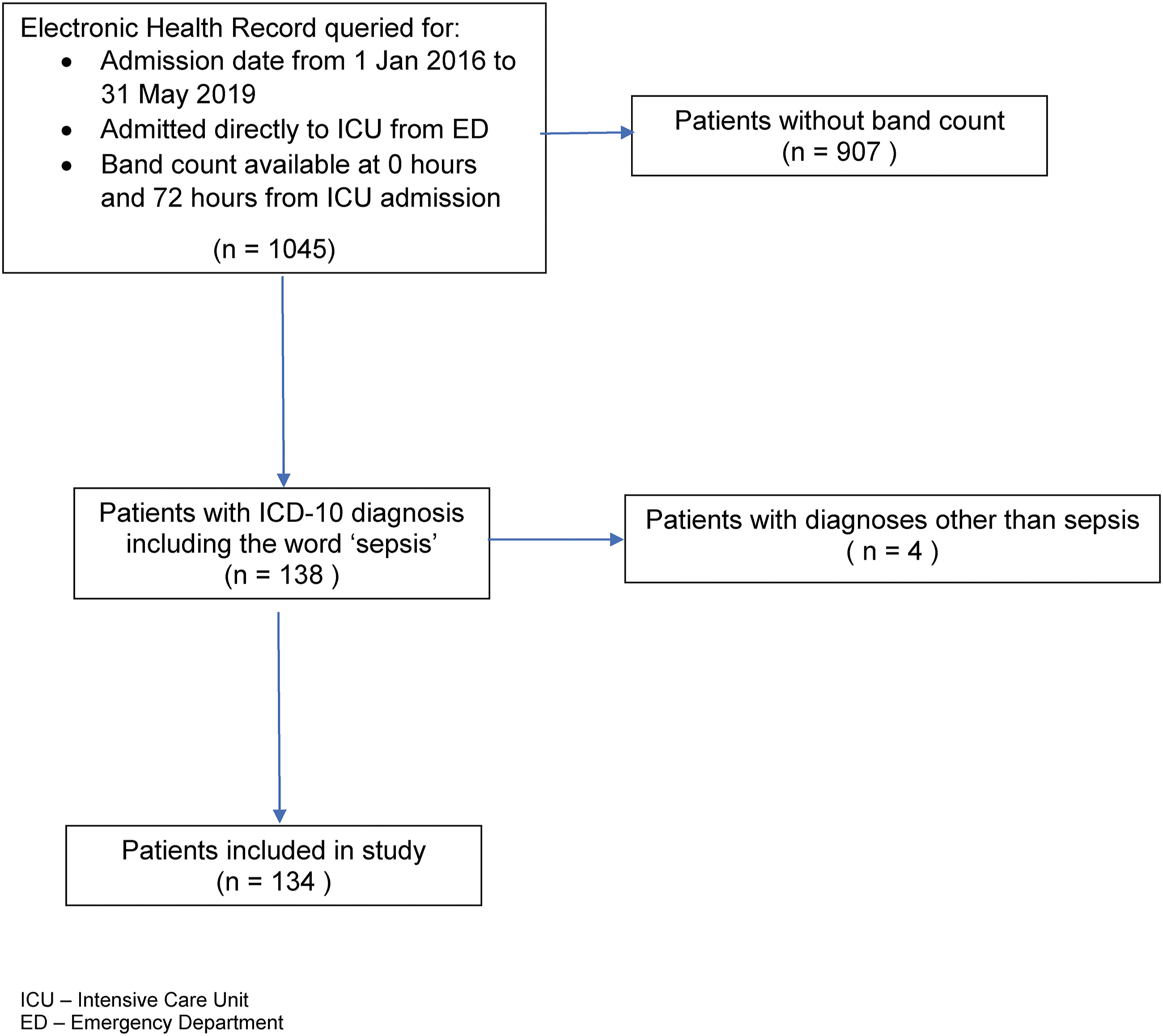
SOFA groups and bandemia percentage change.

SOFA groups and serum lactate levels change.
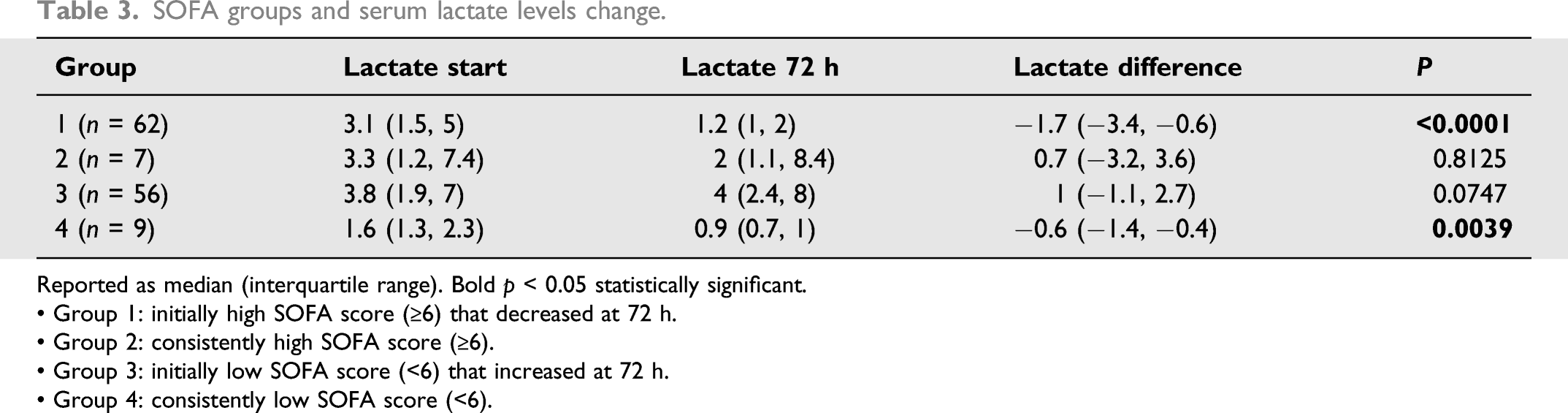
Reported as median (interquartile range). Bold p < 0.05 statistically significant.
• Group 1: initially high SOFA score (≥6) that decreased at 72 h.
• Group 2: consistently high SOFA score (≥6).
• Group 3: initially low SOFA score (<6) that increased at 72 h.
• Group 4: consistently low SOFA score (<6).
Correlation between SOFA changes, band % change and lactate levels.

SOFA changes were statistically significant in relation to band % change and lactate change (ρ > 0.5, p < 0.0001).
Discussion
This study evaluated bandemia trends in relation to the existing clinical data more commonly used for prognostication: serial SOFA scores and serum lactate levels. Our results showed that clearance of an elevated band count over the course of the first 72 h after admission directly correlated with improving SOFA scores. We also found that in patients with an improving SOFA score (group 1), bandemia clearance provided positive prognostic information, similar to that of lactate clearance. It was noted that in patients who had an initial SOFA score <6 and subsequently developed an elevated SOFA, there was a significant relation in the concomitant development of bandemia. It is also worth noting that in patients with a persistently high SOFA score (group 2) and a worsening SOFA score (group 3), there were no significant changes noted in serum lactate level.
Although patients presenting with sepsis or septic shock often exhibit leukocytosis (and occasionally leukopenia), it is important to consider that the time from marrow stimulation to subsequent laboratory-supported bandemia is currently unknown. This study does not address this specific question and further investigation is warranted.
Lactate is the gold standard biomarker for predicting patient outcomes in sepsis. 10 A significantly elevated serum lactate is associated with worse outcomes, 11 and its normalization in sepsis correlates with improved survival.12,13 In addition to its prognostic use, lactate has been demonstrated to be a valid tool in guiding resuscitation. Evidence has shown that a 10% reduction in serum lactate after 2 hours of initial fluid administration corresponds to adequate resuscitation of sepsis. 14
\However, as a non-specific biomarker and natural byproduct of cellular respiration, lactate trends must be interpreted with caution. Potential confounding variables include Type B (non-hypoxic) causes of hyperlactatemia observed in chronic kidney disease and cirrhosis due to reduced lactate clearance.15,16 Other noninfectious etiologies of hyperlactemia include medication induced hyperlactatemia via beta-adrenergic agonism (e.g., albuterol or epinephrine), due to increased glycogenolysis and lipolysis and subsequent increase in anaerobic metabolism. 17 Hypermetabolic states seen in malignancy and generalized tonic-clonic seizure disorder can also produce elevated lactate levels. 18 Lastly, drug-induced mitochondrial dysfunction is often overlooked as a contributor to hyperlactatemia, especially in the ICU setting where medications such as Propofol, 19 Linezolid (in inherited mitochondrial disorders), 20 and Nucleoside Reverse Transcriptase Inhibitors are often administered. 21 Therefore, the addition of another objective marker, such as bandemia trends, could be considered as an adjunct to lactate levels, thus, increasing the accuracy of diagnostics and prognosis in the management of sepsis and septic shock.
There are several limitations to this study. As this study tracked trends in bandemia and lactate levels over 72 h, it excluded patients who died before that period elapsed, and therefore its findings might not adequately represent those with the highest severity of disease at baseline that do not survive the initial hours of septic shock. Our study did not directly measure the association between bandemia and other patient-centered outcomes including mortality. Identifying bands in the lab can prove to be challenging for a variety of reasons including machine error and human error when manual differentiation is performed. As a single-centered study with a small cohort, we recognize the limited impact of this study, and our data needs to be externally validated and correlated with further clinical outcomes. Because our exclusion criteria may have eliminated patients with multiple comorbidities, the generalizability of these findings is limited. Additionally, patient demographics were unevenly represented, as the majority of those cared for were male and African American, limiting the generalizability of our results. Further, the small sample sizes in groups 2 and 4 may have skewed the data. Lastly, we present results that apply solely to those admitted directly to the ICU from the ED. Future studies examining a larger and more diverse pool of patients, across multiple tertiary centers, and those that are identified as critically septic either upon initial presentation or while hospitalized, could further support the use of bandemia trend as a prognostic factor.
Conclusion
Our preliminary study examining the prognostic value of bandemia trends in critically ill, septic patients suggests that bandemia clearance and trending, in conjunction with other existing clinical tools, may be of use as a marker of improvement in sepsis. Conversely, worsening bandemia may be predictive of a deteriorating clinical status and possibly a higher mortality as extrapolated from worsening SOFA scores. The trend of bandemia in the ICU should be further studied to evaluate its role in further resuscitation, need for additional source control and appropriate antibiotic stewardship Furthermore, incorporating bandemia could be helpful in developing a risk stratifying calculator, and may be beneficial when used in conjunction other markers, such as lactate levels, for tailoring therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.