
Abstract
Background: Unplanned intensive care unit (ICU) admission occurs via activation of medical emergency team (MET) and conventional ICU referral (CIR), i.e., ICU consultation. We aimed to compare the dosage, association with unplanned ICU admissions and hospital mortality between MET and CIR systems.
Methods: We performed a retrospective, single centre observational study on unplanned ICU admissions from hospital wards between July 2017 and June 2018. We evaluated the dosage (expressed per 1000 admissions) and association of CIR and MET system with unplanned ICU admission using Chi-square test. The relationship (unadjusted and adjusted to Australia and New Zealand risk of death (ANZROD) and lead time) between unplanned ICU admission pathway (MET vs CIR) and hospital mortality was tested by binary logistic regression analysis [Odds ratio (OR) with 95% confidence interval (CI)].
Results: Out of 38,628 patients hospitalised, 679 had unplanned ICU admission (2%) with an ICU admission rate of 18 per 1000 ward admissions. There were 2153 MET and 453 CIR activations, producing a dosage of 56 and 12 per 1000 admissions, respectively. Higher unplanned ICU admission was significantly associated with CIR compared to MET activation (324/453 (71.5%) vs 355/2153 (16.5%) p < 0.001). On binary logistic regression, MET system was significantly associated with higher hospital mortality on unadjusted analysis (OR 1.65 (95% CI: 1.09–2.48) p = 0.02) but not after adjustment with ANZROD and lead time (OR 1.15 (95% CI: 0.71–1.86), p = 0.58).
Conclusions: Compared to CIR, MET system had higher dosage but lower frequency of unplanned ICU admissions and lacked independent association with hospital mortality.
Introduction
ICU admissions are either planned, usually after elective high-risk surgeries or unplanned, following activation of medical emergency team (MET) or conventional ICU referral (CIR) systems in hospitalised patients. Unplanned ICU admission, with an incidence between 1.1% and 37.1%, 1 refers to transfer of patients to the ICU from a lower intensity area, usually hospital wards, due to an unanticipated clinical deterioration (e.g., worsening of respiratory failure) or serious adverse events (like procedural mishaps, drug, and diagnostic errors) or surgical issues. They are associated with high morbidity, mortality, and cost to the health care system. 1–3
MET services (also known as rapid response system or emergency medical services) are well-known systems in hospitals to manage an acutely deteriorating hospitalised patient. 4 They are embedded within one of the Australian National safety and Quality Health service standards (NSQHS) called “recognizing and responding to acute deterioration” to provide a nationally consistent standard of care aimed at improving patient outcomes. 5 Although the majority of ICU’s in Australia and New Zealand participate in providing MET services, 6 there is inconsistent evidence on its impact on patient survival. 7–14 MET dose, defined as MET activation rates per 1000 patient admissions, varies across countries. 15 Although MET dose has favorable dose-response effect in reducing in-hospital cardiac arrest, it is inconsistent with outcomes such as hospital mortality. 15,16 International liaison committee on resuscitation (ILCOR) guidelines recommend early recognition and intervention of patients at risk of deterioration by activating rapid response systems. 17 Following activation, 10–20% of MET calls result in unplanned ICU admission. 6
Conventional ICU referral (CIR) system occurs when the home team seek ICU consultation or review of their hospitalised ward patients. An important objective of this referral process is for consideration of “early” ICU admission anticipating clinical deterioration. Although there is evidence on outcomes of patients having unplanned ICU admission, there is minimal data on the dosage, association with unplanned ICU admission and outcome of patients having unplanned ICU admission following a CIR. 6,18
Hence, we undertook a retrospective, observational study to compare the dosage, clinical characteristics, morbidity and hospital mortality between MET and CIR mediated unplanned ICU admissions. We hypothesized that unplanned ICU admissions following MET in comparison to CIR would be associated with higher hospital mortality.
Methods
Design and Setting
This retrospective, single-center, observational study was undertaken at Lyell Mc Ewin Hospital in South Australia, from July 2017 to end of June 2018. Central Adelaide Local Health Network Human Ethics committee approved this study with waiver of consent (HREC/18/NALHN/583). Lyell McEwin is a major metropolitan public hospital in Northern Adelaide Health Network (NALHN) that serves a population of about 3,95,000 within the northern metropolitan area of Adelaide, South Australia and over 50,000 from regional areas are referred.
Our ICU is 20 bedded (2 pods, each with 10 beds), with ability to invasively ventilate 14 patients. It has an average annual admission of approximately 1600 patients with a bed occupancy rate of 80–90%. The case-mix in our ICU is predominantly general medical with lesser surgical and occasional high-risk obstetric cases. Our ICU is staffed with three consultants having clinical roles, one for each pod and the third one for ICU outreach activities (designated as “duty intensivist”). Additionally, the duty intensivist is also responsible for ward-based total parenteral nutrition (TPN) service. 19
Calling criteria for medical emergency team.
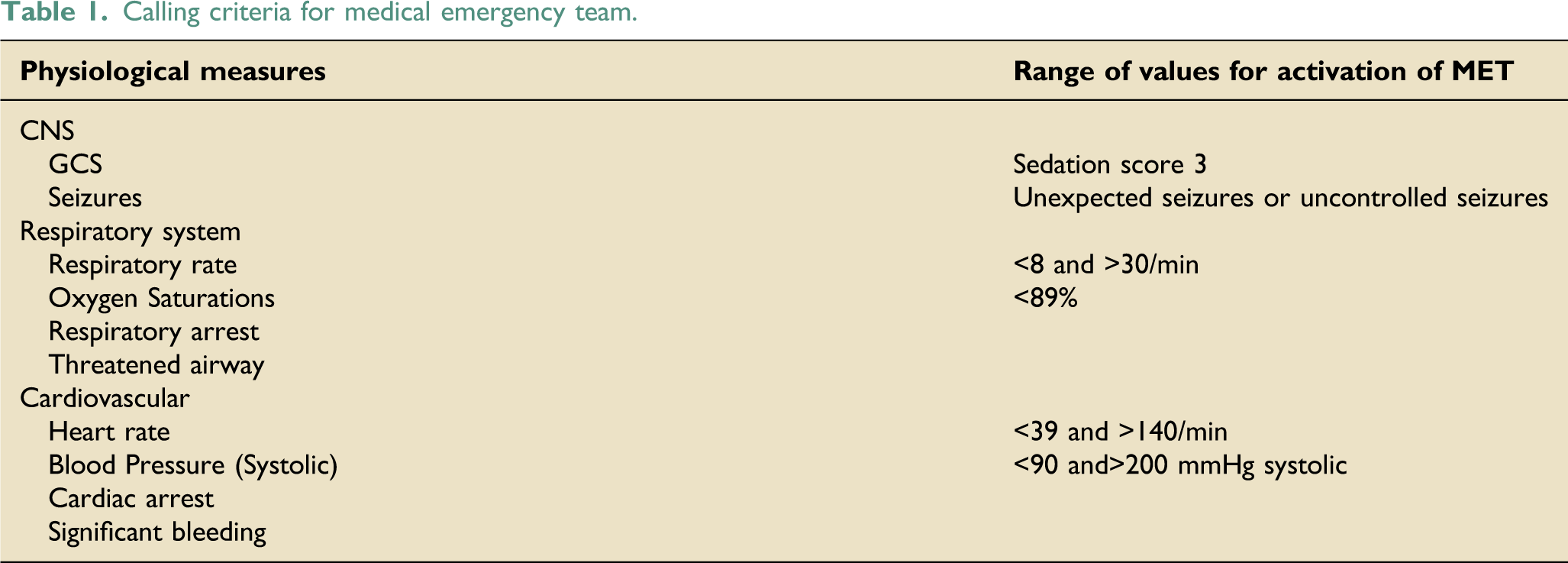
A CIR is initiated as an escalation process by the home team, after their review of a deteriorating patient, as per the RDRA chart recommendation or if the home team is concerned by the presence of worsening trends of patient’s clinical investigations (biochemistry, hematology, or radiology). This occurs before the patients meet the criteria for triggering a MET call. This escalation process is followed in hospitalized ward patients and in those having unanticipated deterioration during surgery.
During business hours (8:00 a.m to 5:00 p.m., Monday to Friday), the MET call’s and CIR’s are overseen by the duty intensivist, who is physically present in the ICU and immediately available for advice. 24 The MET calls and CIR’s are attended, either by the ICU registrar or the duty intensivist or both. During after-hours (5:01 p.m. to 7:59 a.m. throughout the week), the MET calls and CIR’s are reviewed by the ICU registrar, who then remotely (over the phone) discusses about these patients with the on-call ICU consultant. Following a MET call or CIR, the admission of patients to ICU is decided by the duty intensivist during business hours and on-call consultant during after-hours.
Unplanned ICU admission refers to those happening from hospital wards, post-operative recovery area via MET or CIR and patients having unanticipated deterioration during surgery, occurring exclusively via CIR.
Inclusion and Exclusion criteria (Figure 1)
All adult patients (age ≥18 years) having unplanned ICU admission by activation of MET services or by CIR were included. Patients aged <18 years, planned admissions (elective high-risk surgeries and those that could be delayed for 24 h with no adverse effect, as defined by the Australia and New Zealand Intensive care society adult patient data set ANZICS-APD) 19 patients lacking data on hospital outcome, patients admitted from emergency department (ED), another hospital or ICU, and patients sustaining respiratory or cardiac arrest (in and out of hospital) were excluded.
Data collection
Data on age, gender, time of ICU admission (classified as business hours (8:00 a.m. to 5:00 p.m.), or after hours (5:01 p.m. to 7:59 a.m.)), 19 comorbidities, severity of illness (Acute physiology and chronic health evaluation (APACHE-III) score, Australia and New Zealand risk of death (ANZROD %)), ICU and hospital length of stay (LOS, in hours), ICU interventions, ICU readmissions, and mortality (ICU and hospital) were extracted from locally stored data collected for ANZICS-CPD. Data on number of hospital admissions was obtained from hospital case mix analyst. Data on MET and ICU referrals were obtained from locally maintained MET and patient referral datasets, respectively.
Pre-ICU LOS (Lead time) is the duration of time in hours spent by the patient in hospital prior to ICU admission. ICU interventions include treatments and procedures performed exclusively in ICU such as mechanical ventilation and vasoactive therapy. ICU and post-ICU hospital LOS are the time spent (in hours) in ICU and post-ICU discharge in hospital, respectively. LOS (ICU and post-ICU in hospital) and ICU readmission were represented as morbidity. ICU and hospital mortality included deaths that occurred in ICU and in wards, post-ICU discharge, respectively.
Objectives
The primary objective was to evaluate the dosage of activation of MET and CIR systems. Secondary objectives were to determine the association between unplanned ICU admission from hospital wards with MET and CIR systems, and compare their clinical characteristics, morbidity and hospital mortality.
Statistical analysis
MET activation and CIR dosage was expressed as number of MET activations and CIR requested per 1000 hospital admissions, respectively. 15 We assessed normality of distribution for all data. Continuous data were reported as mean with standard deviation, (SD) or median with inter-quartile range (IQR) and compared between groups by Student’s t-test and Mann–Whitney U test, respectively. Categorical data was reported as frequency (percentage) and compared between groups using Chi-square test or Fisher’s Exact test. The relationship between hospital mortality and the pathway of unplanned ICU admission (MET vs CIR) was tested by binary logistic regression, unadjusted and adjusted to ANZROD and lead time with results depicted as Odds ratio (OR) with 95% confidence intervals (CI). We chose ANZROD (which is derived from APACHE III score components, source of admission to ICU and hospital, lead time, elective surgery, treatment limitation, ventilation status, and APACHE III diagnosis), as it is customized to Australia and New Zealand, and has shown to have better calibration and discrimination over APACHE III for mortality prediction.6,25 We also included lead time in the multivariable model as we considered it to be an important confounder in the context of testing the systems (MET and CIR) effecting unplanned ICU admissions. All significance testing was two tailed with significance (α) level set at 0.05. SPSS statistics version 27 (IBM, Armonk, NY) was used for data analysis.
Results
Derivation of final cohort (patient selection)
During the study period, 55,433 patients were admitted to the hospital of which 38,628 belonged were hospitalised in medical, surgical, and womens health wards. Out of these 38,628 patients, 679 had unplanned ICU admission (2%) with an ICU admission rate of 18 per thousand admissions.1761 patients required ICU admission; of these 679 (39%) were unplanned from medical, surgical and womens health wards and they formed the final cohort for analysis (Figure 1). Out of the 38,628 hospitalised patients, there were 2153 MET activations and 453 CIR, thereby producing MET and CIR dosage of 56 and 12 per 1000 admissions, respectively. Out of 2153 MET calls activated, 355 required ICU admission (16.5%). Out of 453 conventional ICU referrals, 324 (71.5%) required ICU admission (Figure 1). Unplanned ICU admission was very strongly associated with ICU referral compared to MET activation (71.5% vs 16.5%, p < 0.001). Unplanned ICU admissions: derivation of study cohort.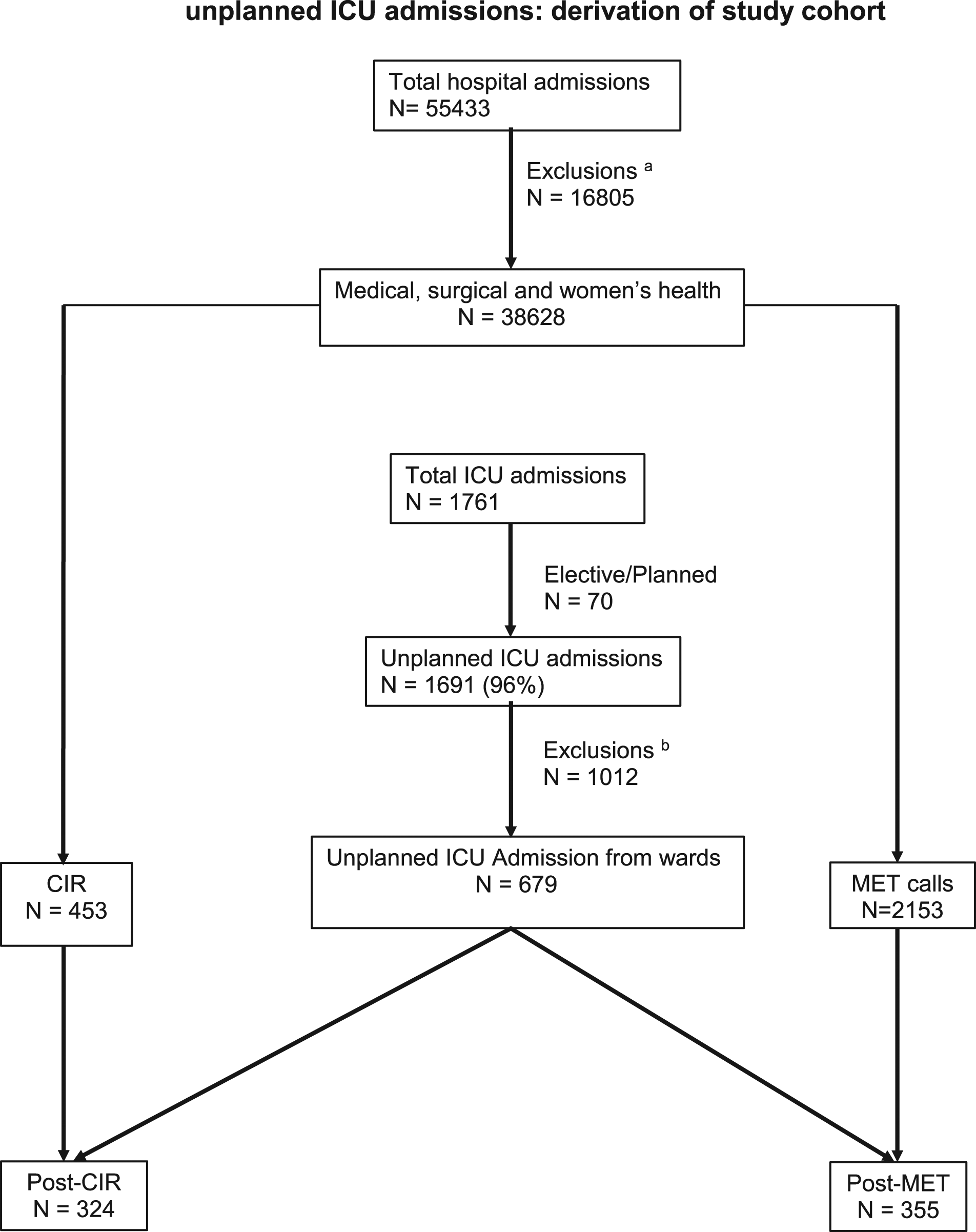
Demographics and Comorbidities
Demographic characteristics.
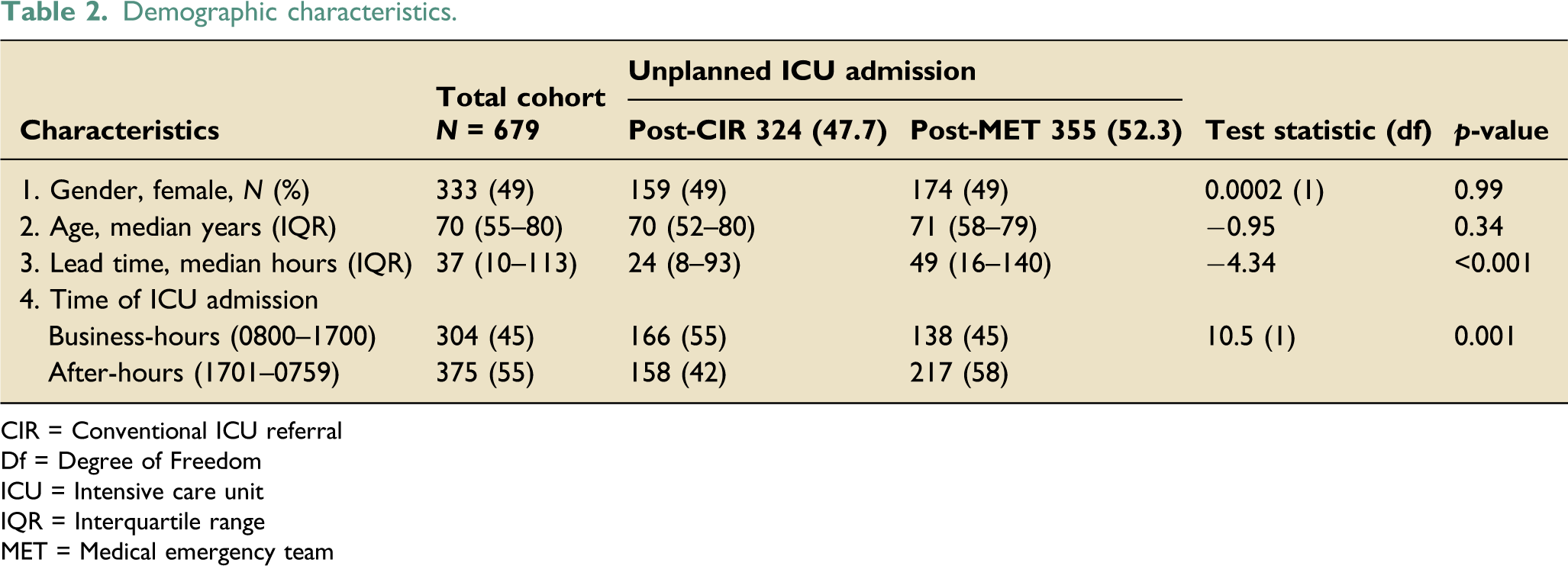
CIR = Conventional ICU referral
Df = Degree of Freedom
ICU = Intensive care unit
IQR = Interquartile range
MET = Medical emergency team
Comorbidities.
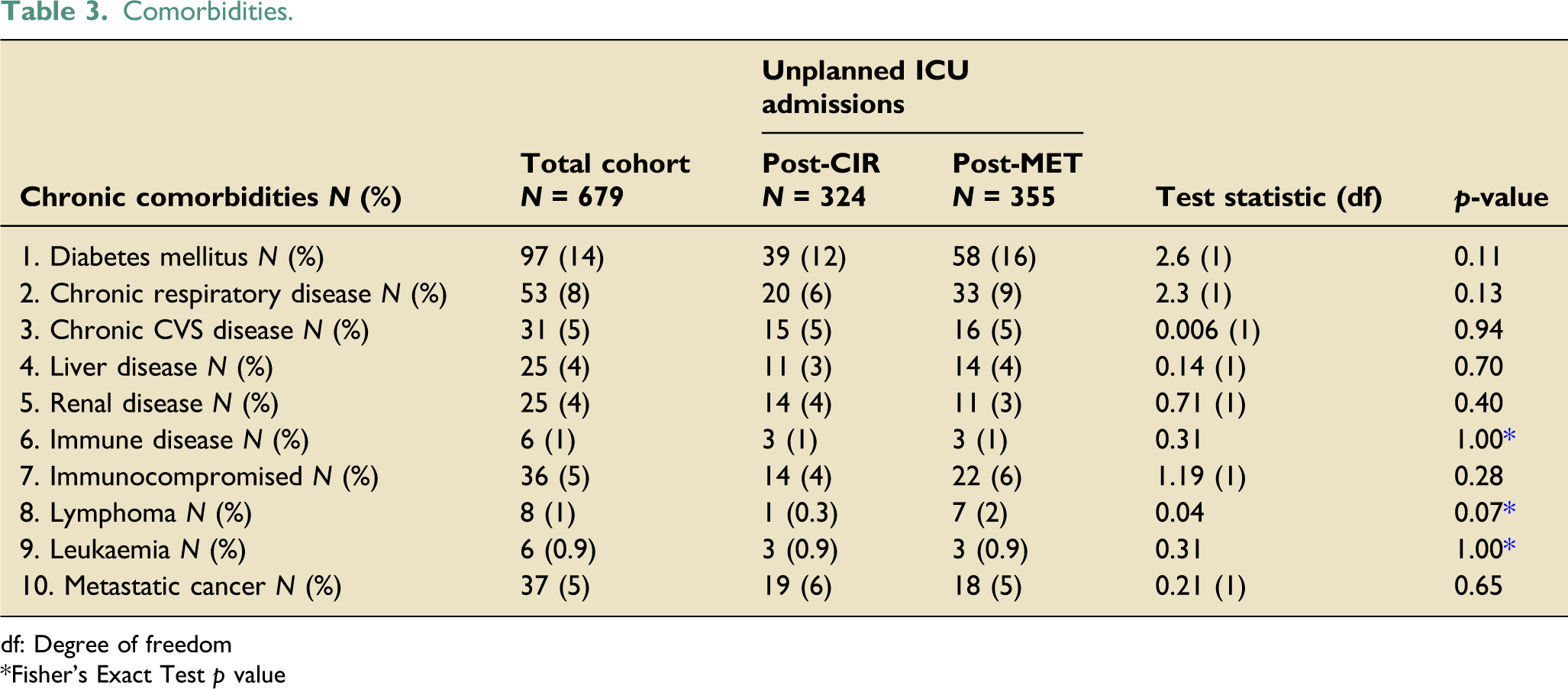
df: Degree of freedom
Fisher’s Exact Test p value
Clinical characteristics at ICU admission
Clinical characteristics.
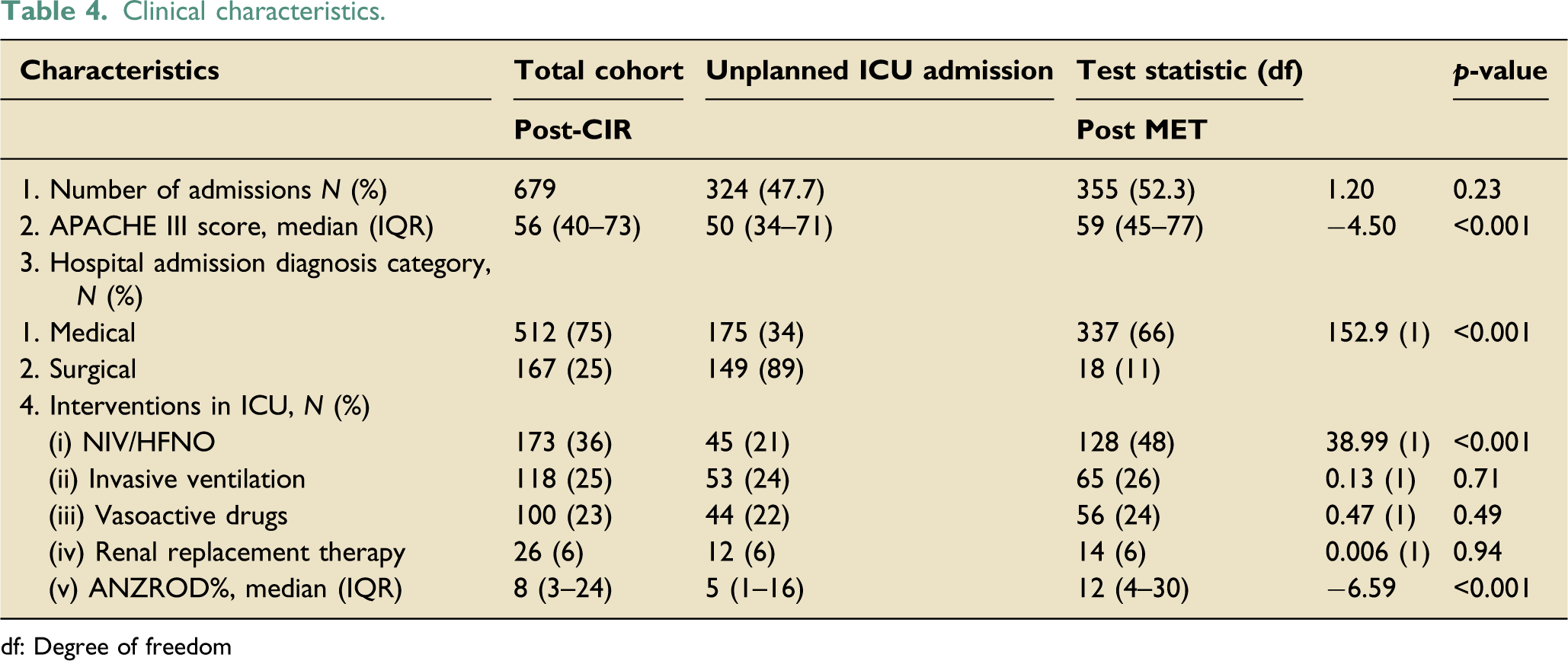
df: Degree of freedom
Morbidity and pathway of unplanned ICU admission (MET vs CIR)
Morbidity and mortality
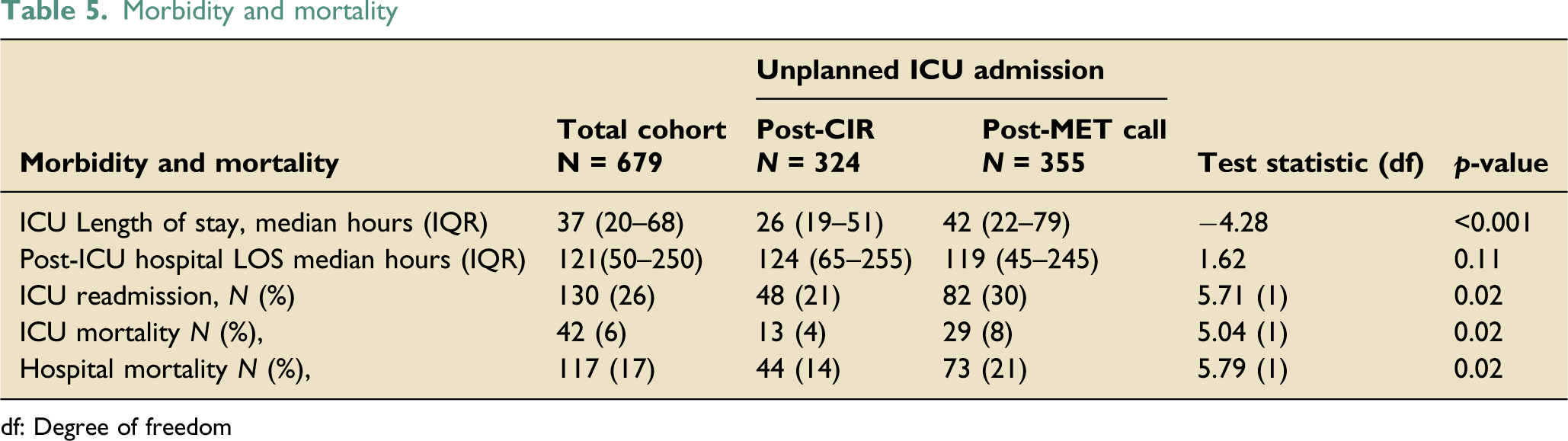
df: Degree of freedom
Hospital mortality and pathway of unplanned ICU admission (MET vs CIR)
Unadjusted and adjusted binary logistic regression of hospital mortality and unplanned ICU admission pathway.
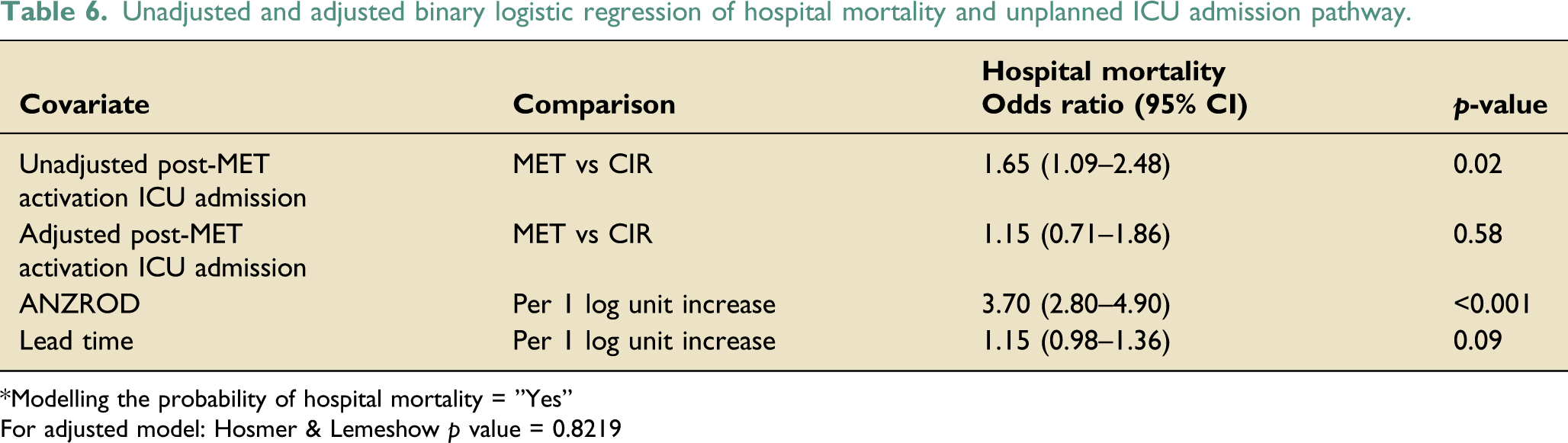
*Modelling the probability of hospital mortality = ”Yes”
For adjusted model: Hosmer & Lemeshow p value = 0.8219
Discussion
In this study, we provide a detailed report on health care outcomes of patients having unplanned ICU admissions from hospital wards via MET and CIR systems.
Key findings
Unplanned ICU admissions
We report a greater number of unplanned ICU admissions from hospital wards compared to previous studies 26–30 (39% in our study vs. 1.1–37.5% in previous studies). This may be due to the variation in inclusion criteria used in the studies and differing thresholds to admit a patient to ICU across hospitals, which depends on the hospital structure, case mix, and resources. 31 ICU care and post-ICU survivors have ongoing complex health care needs that can potentially elevate health care costs. 32
Conventional ICU referral (CIR)
Seventy-two percent of conventional referrals resulted in ICU admission compared to 49% reported in an earlier study. 33 However, this study included only those patients admitted to a medical ICU and having <48 h of lead time to ward admission from emergency department. This higher proportion of ICU admissions following CIR in our study is probably due to inclusion of hospitalized medical and surgical patients, no time limit on lead time prior to seeking CIR and potentially early home team review resulting in early identification of patients who would probably benefit from early ICU admission. This earlier attention and intervention sought by CIR may have decreased the lead time before ICU admission and perhaps decelerated the trajectory of patient deterioration. This may be an important factor accounting for reduced severity of illness (lesser APACHE III scores and ANZROD), ICU LOS and mortality (ICU and hospital) in patients admitted through CIR at our institution, which is similar to other studies. 9,18 Although there is ample evidence on MET systems, 15,34–39 there is no data on the dosage and functioning of CIR system. We believe ours is the first study to report dosage of CIR in hospitalised patients (12 per 1000 hospital admissions). Future research in a larger population from multiple centres is required to confirm our observation.
Medical Emergency referral (MET)
The dose of MET activation in our study (56 per 1000 admissions) was similar to previous Australian studies,37,38 and higher than that of an American study. 39 Although, we recorded a higher MET dose, the frequency of ICU admissions following MET calls (16%) was similar to previous studies (10–20%).18,40,41 The higher number of MET calls were likely reflective of having a single tiered rapid response system and broadening our inclusion criteria to patients only from medical, surgical, and women’s health wards. Potentially, the varying experience of nursing and medical staff in managing a deteriorating patient, may have led to a lower threshold to activate MET calls in hospital wards. This group of patients that were admitted to ICU were associated with longer lead time, higher severity of illness scores (APACHE III and ANZROD), longer ICU stays and higher ICU and hospital mortality, which were consistent with other studies,18,40 We certainly acknowledge that the provision of MET service may vary across hospitals and different health care settings, which may influence the dose of MET calls, incidence of post-MET call ICU admission and clinical outcomes. Studies have shown that the optimal dose of MET calls for improved patient outcomes is around 30 and ranges between 25.8 to 56.4 per 1000 hospital admissions and higher MET dosage does not improve hospital mortality.15,38,39
MET and CIR mediated unplanned ICU admissions versus hospital mortality
Unadjusted analysis showed that the risk of hospital mortality after ICU admission following a MET call was significantly higher compared to CIR (Table 6). However, this significance was lost after adjustment for severity of illness (ANZROD) and lead time. We believe, by including ANZROD in the multivariable model, we were able to adjust multiple potential confounders (variables that make up ANZROD) of mortality. These results were consistent with two earlier studies, where the multivariable model included severity of illness. 6,41 However, this binational study included hospitals with single and multi-tiered MET system, 6 whereas patients in our study were admitted to the ICU under a single-tiered MET system.
In summary, data on the proportion of hospitalized patients having unplanned ICU admissions, dosage of MET activation and CIR could provide useful information to health care policy makers towards financial and resource allocation.
The major strengths of our study include providing a detailed evaluation of the processes effecting unplanned ICU admission from hospital wards, that is, the CIR and MET system including their dosage and comparative data of clinical outcomes. Although there is abundant evidence on functioning and dosage of MET services,15,34–39 we believe this is the first study that provides data on detailed evaluation of CIR.
In addition to having a retrospective design, our study had significant limitations. As with any retrospective study, selection bias was a concern and we attempted to minimize this by excluding patients who were referred from ED. and other hospitals and those sustaining in-hospital cardiac arrest. However, the presence of higher heart rate activation criteria compared to other centers and having more patients with medical diagnoses admitted via MET pathway may have given rise to a selection bias, with more sicker patients admitted via MET pathway compared to CIR. Our study lacked data on patients experiencing multiple MET and CIR activations and on treatment limitations initiated or advised during MET calls and CIR’s, which may have impacted the proportion of unplanned ICU admissions and mortality. We acknowledge that the systems and processes in managing a deteriorating patient (MET and CIR) may vary across different centers. This poses significant limitation in interpreting the results of our study as it was conducted in a single center. Additionally, our study lacked data on the following information that may have affected the dosage and proportion of unplanned ICU admissions: number of patients who were exposed to both MET and CIR, those that were physically reviewed by ICU consultant during MET calls and CIR’s, non-availability of on-site ICU consultant during after-hours and absence of ICU follow-up visits.
Conclusions
A large proportion of ICU admissions were unplanned from hospital wards. Compared to MET system, CIR was associated with higher unplanned ICU admissions. In our study, earlier identification and escalation of a deteriorating patient may have been a key factor that was associated with better clinical outcomes. MET system could be made more effective by incorporating more patient-centered triggers thereby enhancing the escalation process in the management of a rapidly deteriorating patient. We need multi-centered, prospective studies on escalation processes of managing a rapidly deteriorating patient to improve patient outcomes.
Footnotes
Acknowledgements
The authors would like to extend their gratitude to all the data entry officers, MET team nurses and research coordinators at Lyell Mc Ewin Hospital, Adelaide SA, involved in collection and maintenance of database, for their eternal support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.