
Abstract
Blood for coagulation analysis can be sampled from the arterial or venous system in intensive care units (ICU). The determination of clot microstructure and strength by fractal analysis (d f ) gives valuable information in a range of vascular haemostatic disease and sepsis. We aimed to determine if d f could be measured equally and comparatively in arterial or venous blood, and 45 critically ill patients in an ICU were recruited. d f was found to be readily measured in arterial blood with results comparable to those in venous blood and that add value of d f as a potential marker of haemostasis in these patients.
Introduction
Coagulopathic conditions occur in the body when the ability of blood to form normal haemostatic blood clots is impaired and is associated with significant morbidity and mortality. 1 Many diseases and their treatment and syndromes such as SIRS and sepsis may have a detrimental effect on the kinetics of coagulation. 2 The measurement and assessment of these coagulation changes may give differing results due to inherent physiological and pathological differences between arterial and venous blood. 3 Furthermore, many of these patients undergo rapid pathophysiological progression or regression which will require an accurate assessment at the bed side to assess and monitor these changes. Blood sampling is often carried out in arterial or venous blood in ICU; however, it is important to ensure there is compatibility in their results due to inherent variation.
Fractal dimension (d f ), a functional biomarker of coagulation/haemostasis, can be used as a point of care test to quantify the quality and arrangement of clot microstructure.4,5 In this study, we measured d f and clot quality in both arterial and venous blood from the same patient simultaneously to determine whether there is any difference in the clot microstructure in the two vascular systems. In previous studies, d f has been shown to assess globally the end point of the coagulation pathway and the secondary effects of disease and its treatment accurately in terms of clot quality. We therefore further assess d f in both arterial and venous blood as a potential global marker for haemostasis. 7
Methods
Study design and patients
This prospective observational study was carried out in a large teaching hospital general ICU and emergency department. This study had full ethical approval from South Wales Research Ethics Committee. An informed 2-stage written consent was obtained from patients with capacity and from those who lacked capacity; an assent was obtained from personal or legal representative. Forty-five adult patients (age ≥ 18) who had both arterial and central venous catheters were included. Patients who were on therapeutic anticoagulation were excluded.
Blood Sampling
Unadulterated whole blood (6.6 mL) was collected by withdrawing from arterial and venous catheters separately and was transferred to double concentric cylinder geometry on AR-G2controlled stress rheometers (TA Instruments, New Castle, DE, USA) at a temperature of 37oC (± 0.1oC). As described in previous studies, the blood sample was then subjected to a shear stress at frequencies of 0.2 Hz, 0.4309 Hz, 0.9283 Hz, and 2 Hz and the phase angle (δ) was measured with respect to time (s). Gel point was obtained graphically from which d f was determined.6-8
Statistical analysis
All statistical analysis was carried out on GraphPad Prism 9 software. A Bland–Altman plot was used to determine the agreement between the measurement of d f on arterial and venous blood. Bias was defined as the mean difference ± 2 SDs of the difference.
Results
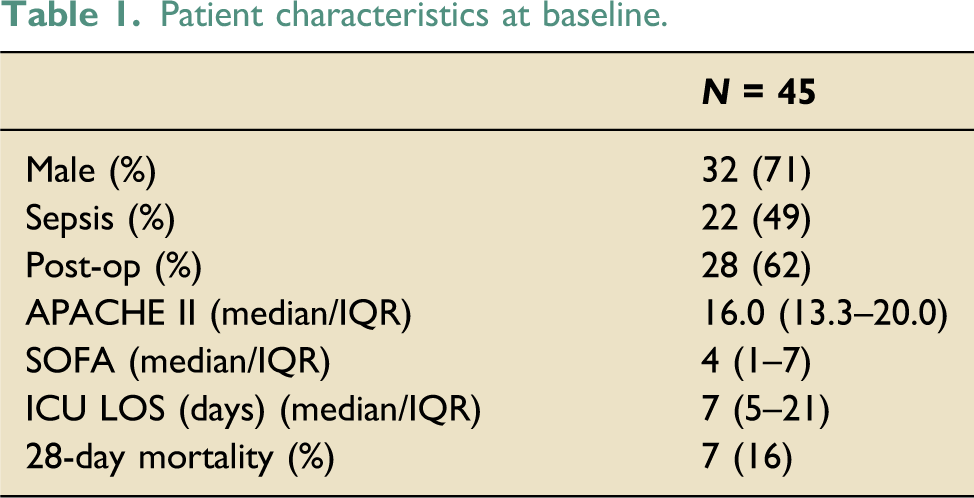
Demographics
Patient characteristics at baseline.
Rheological markers (d f )
From Figure 1, the Bland–Altman plot shows that the majority of the samples lies in between the defined values of the mean difference ± 2 SDs. Fractal dimension (d
f
) measurements in both arterial and venous samples. The Bland–Altman plot shows that the majority of the samples lies in between the defined values of the mean difference ± 2 SDs (standard deviation).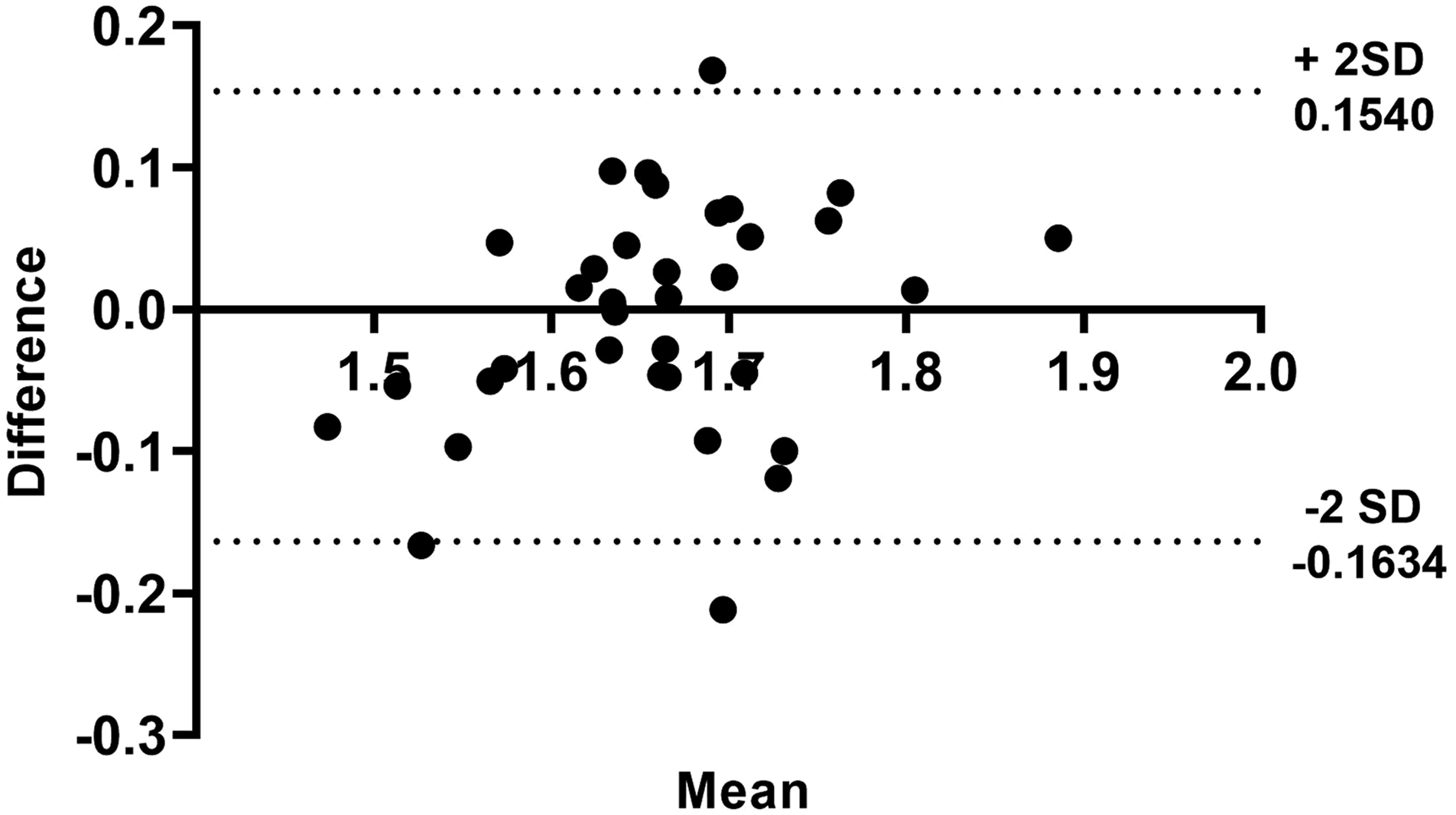
Discussion
In this study, we show for the first time that d f conclusively demonstrates that blood can be taken from either arterial or venous blood and reliably give a comparative and accurate result, irrespective of the underlying pathological condition. Previous studies have shown that the test values can give different results when blood is sampled from either the venous or arterial systems. 7 In our study, we show that the biomarker of clot microstructure gives consistent and equivalent values from arterial and venous sampling points, irrespective of the underlying condition or its treatment. This also gives further evidence that scientific measurements of clot microstructure, such as df which is a structural marker of the end point of the coagulation system, may give a more meaningful and accurate marker of haemostasis in either arterial or venous blood.8-10 The limitations of the study were it being a single-centre observational study and further studies are required to assess its potential.
Footnotes
Acknowledgements
Our thanks go to the staff in the Ed Major Intensive Care Unit and Welsh Centre for Emergency Medicine Research of Morriston Hospital for their invaluable support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Institute for Social Care and Health Research (NISCHR) and was part-funded by the European Social Fund (ESF) through the European Union’s Convergence programme administrated by the Welsh Government.