
Abstract
Objective
COVID-19 has created unique challenges for families of patients admitted to intensive care units. Restricted visiting, language barriers and time constraints have limited communication, resulting in a lack of understanding and anxiety. We introduced digital animations to support communication and assessed the impact on families of patients admitted to intensive care.
Methods
Multi-language animations explaining mechanical ventilation, (www.explainmyprocedure.com/icu) were introduced at two London intensive care units during the COVID-19 pandemic. Web-links were sent by email. Reported understanding of the treatment, its benefits, risks and alternatives was assessed among family contacts of 71 consecutive patients admitted to intensive care; 39 before the animations were introduced (no animation group) and 32 afterwards (animation group). Reported understanding in the two groups was assessed by telephone questionnaire and compared.
Results
Following introduction, all relatives reported they had watched the animation. The proportions who reported complete understanding of mechanical ventilation, its benefits, risks and alternatives, in the no animation group (n = 39) were, respectively, 15%, 28%, 0% and 3% and in the animation group (n = 32), 94%, 97%, 84% and 66% (p < 0.0001 for all comparisons).
Conclusion
Family use of online multi-language animations explaining mechanical ventilation is feasible, acceptable and associated with substantial improvement in understanding. The approach is not limited to mechanical ventilation, or to use in a pandemic, and has the potential to be applied to a wide range of treatment and recovery pathways on intensive care.
Introduction
Understanding of Intensive Care Unit (ICU) treatment is often incomplete among families of patients admitted there. 1 , 2 Language barriers, treatment complexity and time constraints are long-standing challenges, but more recently, COVID-19 has led to restricted ICU access, preventing families from visiting. Effective communication has been further complicated by increased demands on staff who need to look after three or four patients simultaneously instead of one or two. 3
Family satisfaction with information is the first UK standard used to assess high quality care in ICUs and an important outcome for evaluating quality improvement strategies in the ICU. 4 It is also one of the most challenging standards to meet when direct access to ICU is prohibited and time for explanation of treatment is limited. New approaches are therefore needed to save time, support communication and understanding. 5
Multi-language animations describing the benefits, risks and alternatives of commonly performed medical and surgical procedures have been shown to substantially improve patient understanding before consent, both in the elective and urgent patient pathway.6,7 Animations describing ICU and the treatments offered were developed and translated into 5 different languages (Explain my Procedure Ltd) as part of a UK Government Scheme to support the COVID-19 response and were endorsed by the Intensive Care Society.
Here, we describe the introduction of the first of these animations, covering mechanical ventilation, to support staff and families in a large London NHS Trust during the second wave of the COVID-19 pandemic. We report the results of a consecutive survey of reported understanding among relatives of patients admitted to ICU before and after introduction of the initiative.
Methods
This project was conducted, between November 1st 2020 and January 31st 2021, at two hospitals receiving patients with COVID-19 and other acute conditions requiring intensive care treatment and level 3 mechanical ventilation (St Bartholomew’s Hospital and the Royal London Hospital, both part of Barts Health NHS Trust). Family understanding of mechanical ventilation was the primary audit measure assessed in two surveys, before and after introduction of multi-language animations explaining this procedure. Figure 1 shows a flow diagram of the pathway for introducing the animations into practice. We followed the SQUIRE guidance for conducting and reporting quality improvement projects. 8
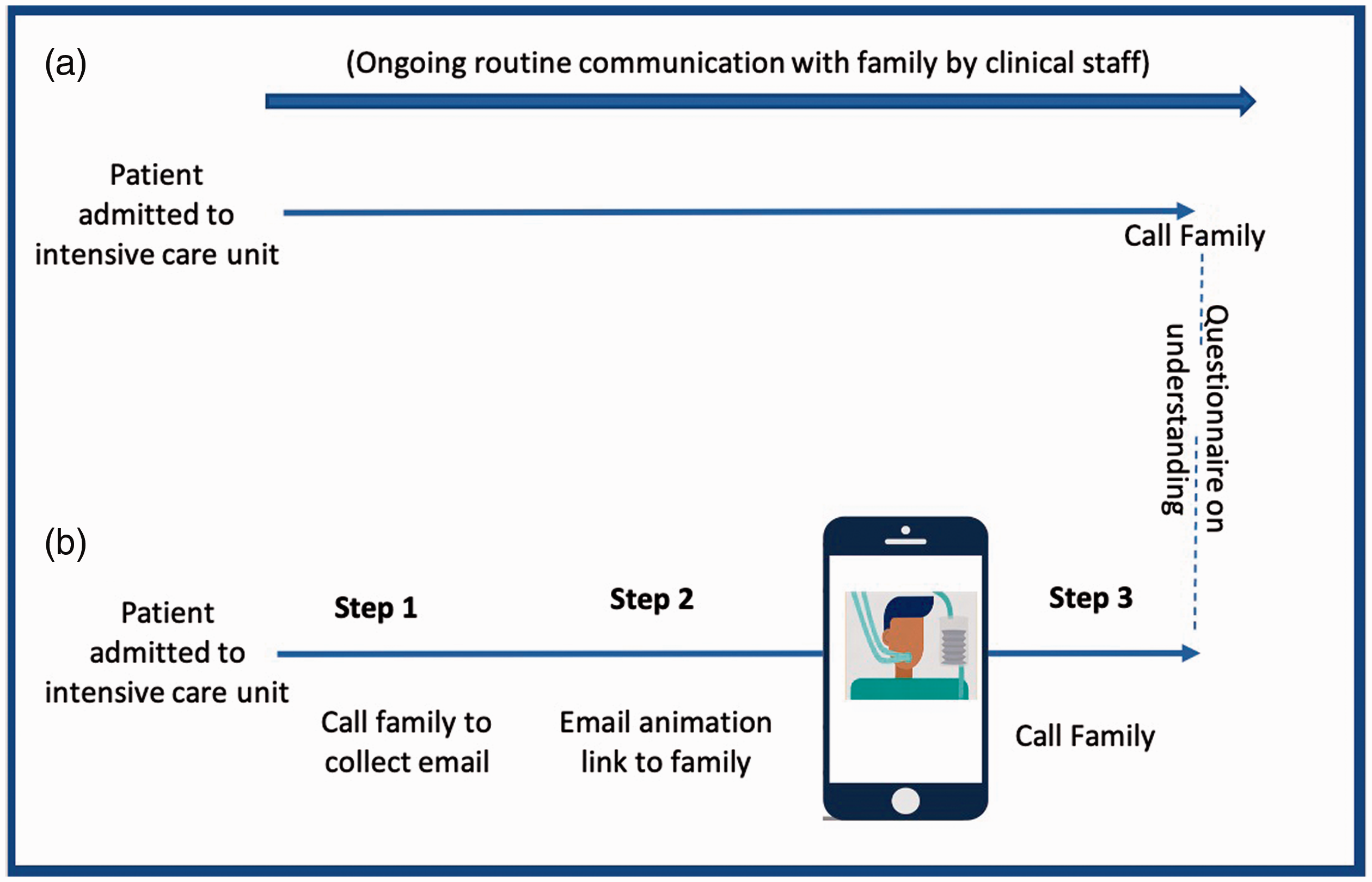
Sequence for 39 relatives before (a) and 32 relatives after (b) introduction of animation explaining mechanical ventilation.
Animations
The animation explaining mechanical ventilation was created according to the NHS Information Standard 9 by Explain my Procedure Ltd (www.explainmyprocedure.com/icu). The animation consisted of a 5 minute video of moving images and characters explaining mechanical ventilation, its benefits, risks and alternatives narrated by a native language-speaker. The information was generic rather than individualised. Families were able to select from one of the five languages (English, Bengali, Hindi, Turkish and Polish) that were most commonly spoken among patients served by Barts Health NHS Trust. Families could view the animations multiple times before speaking to the healthcare professionals familiar with the care of their relative.
Implementation
A standardised approach to introducing the animation into practice at each hospital was adopted based on three steps: (i) calling the next of kin following a patient admission and requesting an email to send the animation web-link (ii) emailing the web-link from a dedicated Trust email account (iii) providing each family with a minimum of 24 hours before further contact by phone to administer the questionnaire and answer questions. The website also had a contact button which families could use to directly call or email the ICU where their relative was receiving care, bypassing the hospital switchboard. For each family, and in almost all cases, the first and second phone calls were made by the same clinician, whilst the email containing the animation link was sent by a communication coordinator from a single patient liaison mailbox.
Survey
In the 6 weeks before introducing the animation, the next of kin of 39 consecutive patients who had been admitted to one of the two ICUs were contacted by phone. They were asked four questions; whether they understood (i) what was meant by mechanical ventilation, (ii) the possible benefits of the treatment (iii) the possible risks and (iv) the possible alternatives. Respondents were asked to answer using one of three responses (understand completely, understand partly, don’t understand). In families where the next of kin did not speak English, a friend or an English-speaking relative translated for them. Following introduction of the animation into practice and over a further 6 weeks, the next of kin of another 32 consecutive patients were contacted and asked the same four questions, followed by three more; whether they had watched the animation prior to being called, whether watching the video had helped their understanding of the treatment and whether it had affected their anxiety levels (increased, decreased or no change). Responses were recorded on a questionnaire (Supplementary Appendix) by clinicians who were familiar with the care the patient was receiving. For reasons of sensitivity, we did not question families of patients who were receiving end-of-life care. There were no other exclusions. All families received usual practice communication with hospital staff that would have applied without use of the animation. This involved a call from a communications hub within 24 hours of admission and updates from doctors if there was a significant change in clinical state or if key decisions were required. Sample size was determined by the time available to complete each audit cycle (6 weeks), anticipating this would include about 35 patients. Assuming an initial level of understanding of 20% a study of 70 patients provided in excess of 80% power to show a 3-fold or greater improvement in reported understanding at a p value of 0.05.
The primary analysis was a comparison of the responses after introducing the animations (animation group) with the responses before their introduction (no animation group). Responses to the questions were analysed categorically (complete understanding versus partial or no understanding) and the data from all three categories reported separately. P values were determined using Fisher’s exact test. Stata V.15 was used for all analyses. The Quality Improvement project was an audit that did not require ethical approval and was registered with the Clinical Effectiveness Unit at Barts Health NHS Trust.
Results
Table 1 shows that the patient and family characteristics before and after introduction of the animations were well matched in terms of age and the proportion of native English speakers, with no statistically significant differences between the groups. There was an expected difference in the proportion of patients admitted with COVID-19 in the second period which corresponded with the second wave of the UK pandemic.
Characteristics of patients and relatives before and after introduction of animation to support communication on Intensive Care.
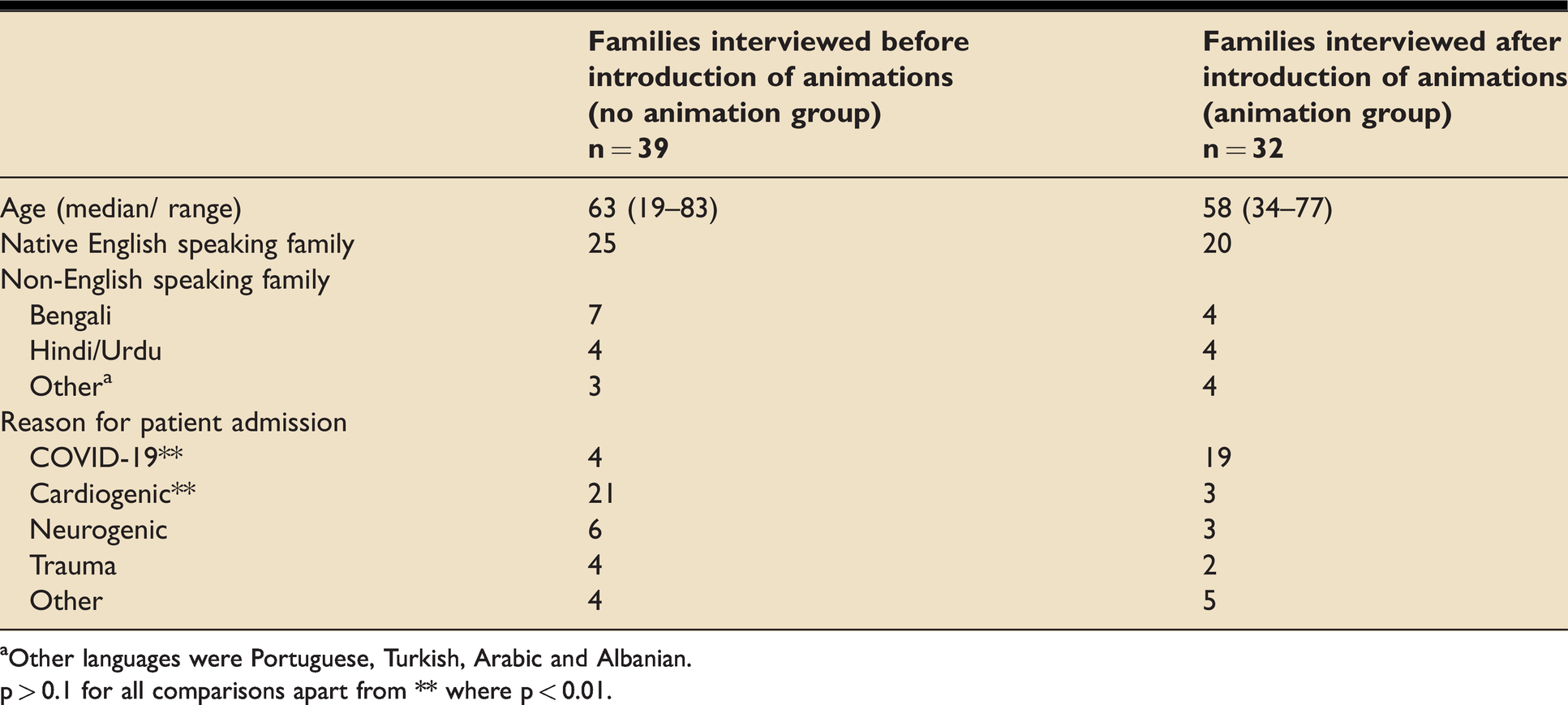
aOther languages were Portuguese, Turkish, Arabic and Albanian.
p > 0.1 for all comparisons apart from ** where p < 0.01.
Figure 2 shows that in the no animation group (n = 39), 15% of relatives reported that they understood what mechanical ventilation involves, 28% that they understood the possible benefits, 0% that they understood the possible risks and 3% that they understood the possible alternatives. In the animation group (n = 32), the respective proportions were, 94%, 97%, 84% and 66% (p < 0.0001 for each comparison with the no animation group). All relatives who were sent the animation watched it and all said it helped their understanding of mechanical ventilation. Among the 32 respondents in the animation group, 7 said the animation made them more anxious, 9 said it made them less anxious and 16 said it did not change their anxiety levels. Supplementary Table 1 gives a summary of the qualitative comments made by relatives after implementation of the animation.
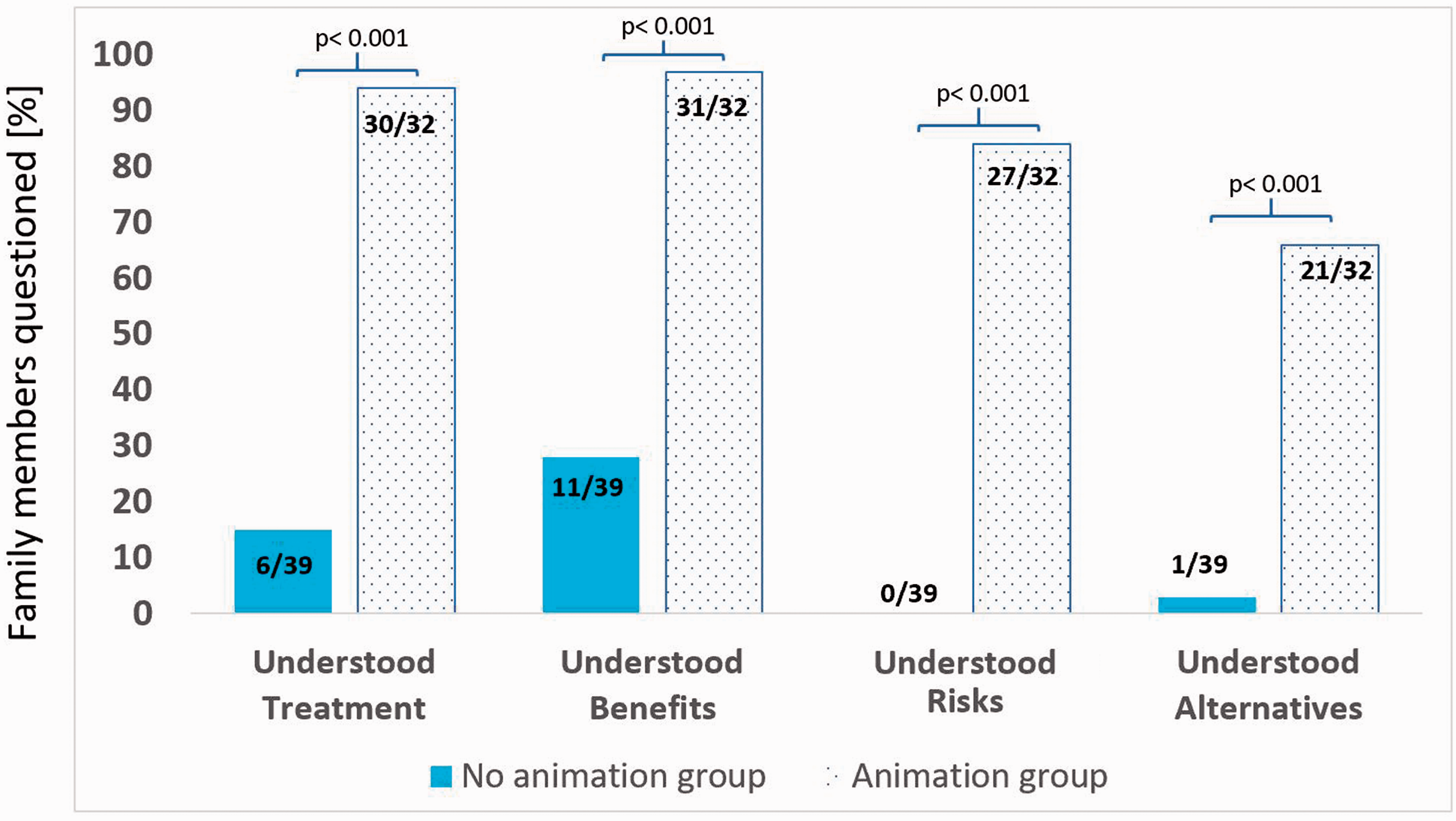
Family-reported understanding of mechanical ventilation in the no animation group (n = 39) and in the animation group (n = 32).
Supplementary Table 2 shows the results for each of the three possible responses (complete understanding, partial understanding and no understanding) to each question in the animation and no animation groups. The proportions reporting “no understanding” of mechanical ventilation, its benefits, risks and alternatives were 28% (11/39) v 0% (0/32), 18% (7/39) v 0% (0/32), 69% (27/39) v 9% (3/32) and 90% (35/39) v 22% (7/32), respectively (p < 0.0001 for all comparisons).
Discussion
Our results show that understanding of mechanical ventilation among the families of patients admitted to Intensive Care is low. About 1 in 8 understood what mechanical ventilation was, about 1 in 4 why it was needed and less than 1 in 30 understood the possible risks or alternatives. Introduction of online multi-language animations substantially improved reported understanding.
The use of images over text has been shown to increase patient understanding and recall of health information and video recordings have been used to reduce anxiety and improve patient satisfaction and comprehension before surgical procedures.10–15 Introduction of digital animations in a network of 9 hospitals lead to a 3-fold increase in understanding of urgent angiography and a 10-fold increase in appreciation of risks before consent. 7 The present work, using multi-language animations, extends this approach to supporting families of patients on intensive care, rather than patients themselves. The striking differences in reported understanding between the animation and no animation groups, particularly in understanding what mechanical ventilation involves (94% v 15%) and appreciation of risk (84% v 0%) quantifies the benefit but also highlights the sizeable gap in understanding that exists and that has, no doubt, been worsened by the COVID-19 pandemic restrictions on visiting and communication.
Anxiety among relatives is high when family require ICU treatment and perhaps even more so when visiting is not allowed. There is uncertainty how individuals will respond to enhanced information in such circumstances, with the possibility of anxiety increasing as well as decreasing. Family satisfaction with information is one of the 3 domains judged most important by families and a key quality measure used for improvement on Intensive Care in the UK. 4 Our results showed an improvement in understanding following introduction of the animations with no material change in anxiety.
The qualitative feedback, summarised in Supplementary Table 1 suggested some unexpected benefits. The style of the animation connected with children as well as adults in families, prompted further learning before the call with hospital staff and provided families with a genuine understanding of treatment rather than the need to pretend they understood after speaking to medical staff. These were anecdotal reports which may prompt future formal evaluations. Further opportunities for development were also highlighted, including a request for explanation of other treatments, such as ECMO and providing translations in other languages.
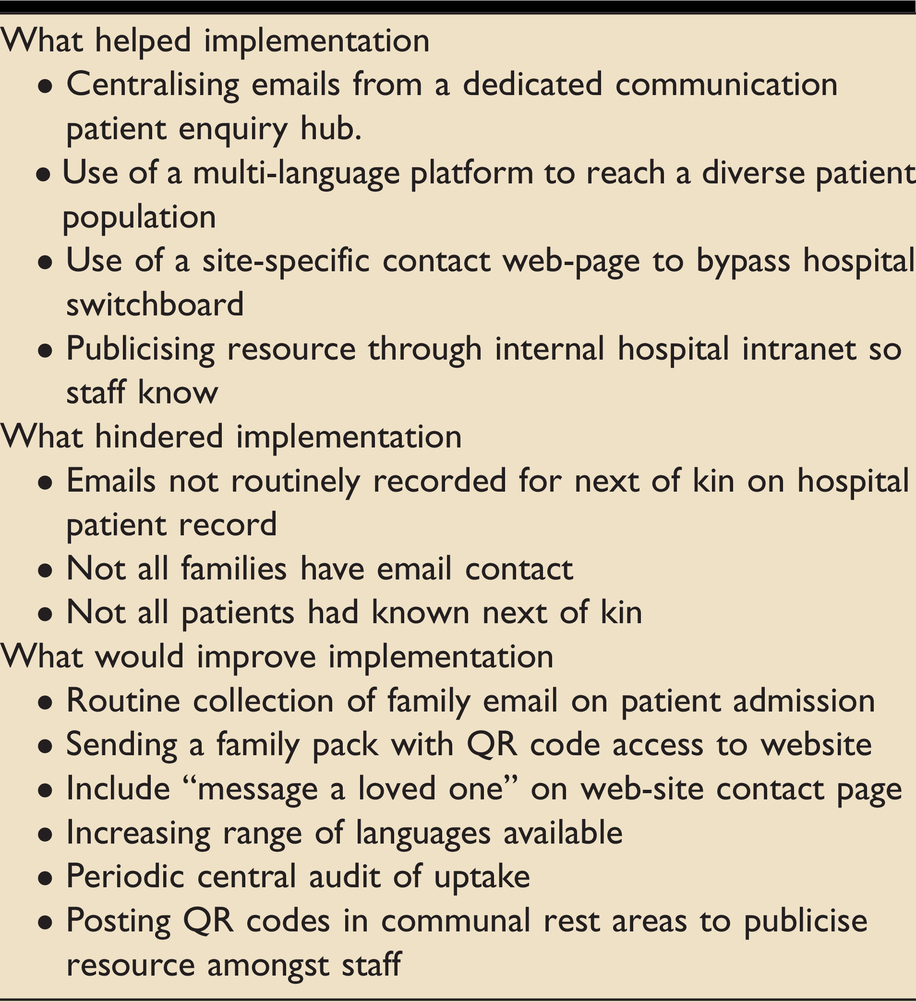
Introducing any new initiative into a busy hospital is challenging and was even more so during a pandemic. The availability of a dedicated communications hub helped with rapid implementation, taking the administrative task of sending emails away from front-line staff. Alternative approaches could include sending a letter containing the web-link or QR code to families as soon as a patient is admitted. Other practical steps which could be applied usefully are summarised in Table 2, together with simple strategies to improve and sustain the initiative going forward. The success of this project benefited from early engagement with intensive care staff before implementation, who generally welcomed the initiative because the problems confronting families and staff were so acute.
Factors influencing implementation of animation- supported communication.
Limitations
Not all families of patients on intensive care were included in this assessment. Over the three month period, 23 families identified by the audit team were not questioned, either because there was no known next of kin or because the patients were receiving end-of-life care; it was judged excessive to ask our questions in such a situation. It is therefore uncertain how this would have influenced the results, but it is likely that even in this group, families would benefit from access to the animation, providing it is introduced soon after admission. The comparison between the no animation and animation groups was not randomised so bias is possible. However, the patients were consecutive and evenly matched in age and language, so it is unlikely that such a large difference in results between the two groups is due to anything other than use of the animation. Having relatives interpret for non-English speaking families could have introduced bias but this would have been similar in both the animation and no animation groups. Objective assessment of understanding was not assessed; our results, like practice in general, were based on person-reported understanding of the treatment offered. At the time of this service development the animations were only available in five different languages and the population of patients spoke eight different languages (overall about 35% were from families who were not native English speakers). Expanding translation to other languages could improve understanding further. Our results relate to ICUs in one hospital Trust and may not be generalisable but may provide a starting point for further evaluations in other ICUs.
Since implementing the mechanical ventilation animations at Barts Health NHS Trust, Explain my Procedure Ltd have created a further four animations; (ICU environment, tracheostomy, induced coma, and COVID treatment, each in five languages. Welsh has been added as this is a legal requirement for patient information in Wales. The Explain my Procedure ICU animations were used in 45 ICUs around the UK for free during the second wave of the pandemic and thereafter by subscription (www.explainmyprocedure.com/icu).
Conclusion
Use of online multi-language animations to support communication with families of patients admitted to ICU was feasible during the COVID-19 pandemic, acceptable and associated with substantially greater reported understanding of mechanical ventilation and its associated benefits, risks and alternatives. The approach can be applied to other treatments on ICU and to practice beyond the pandemic.
Supplemental Material
sj-pdf-1-inc-10.1177_17511437211031841 - Supplemental material for Animation supported communication on intensive care; a service improvement initiative
Supplemental material, sj-pdf-1-inc-10.1177_17511437211031841 for Animation supported communication on intensive care; a service improvement initiative by Marta Wachtl, Frances Ledesma, Hannah Malcolm, Connor Toal, Charlotte Kavanagh, Julia Hadley, James Pennington, Stephen Shepherd and David S Wald in Journal of the Intensive Care Society
Footnotes
Acknowledgements
We thank Caroline Slater, Leisa Griffiths, Shibolin Nahar and Barbara Vassel for their help in administering the project. We thank Shibolin Nahar for her help with sending emails to families of patients admitted to Intensive Care.
Declaration of conflicting interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.