
Abstract
A thirty-year-old pregnant woman was admitted to hospital with headache and gastrointestinal discomfort. She developed peripheral oedema and had an emergency caesarean section following an episode of tonic-clonic seizures. Her delivery was further complicated by postpartum haemorrhage and she was admitted to the Intensive Care Unit (ICU) for further resuscitation and seizure control which required infusions of magnesium and multiple anticonvulsants. Despite haemodynamic optimisation she developed an acute kidney injury with evidence of liver damage, thrombocytopenia and haemolysis. Haemolysis, Elevated Liver enzymes and Low Platelets (HELLP) syndrome, a multisystem disease of advanced pregnancy which overlaps with pre-eclampsia, was diagnosed. HELLP syndrome is associated with a range of complications which may require critical care support, including placental abruption and foetal loss, acute kidney injury, microangiopathic haemolytic anaemia, acute liver failure and liver capsule rupture. Definitive treatment of HELLP is delivery of the fetus and in its most severe forms requires admission to the ICU for multiorgan support. Therapeutic strategies in ICU are mainly supportive and include blood pressure control, meticulous fluid balance and possibly escalation to renal replacement therapy, mechanical ventilation, neuroprotection, seizure control, and management of liver failure-related complications. Multidisciplinary input is essential for optimal treatment.
Case presentation
A thirty-year old year old primigravida presented at twenty-nine weeks gestation, carrying twins, feeling generally unwell and with upper gastrointestinal discomfort and headache. Her vital signs were initially normal and there was no hyperreflexia or focal neurological deficit. She had previously been diagnosed with mild pregnancy-induced hypertension but had not started any medication.
She was admitted to the labour ward for close monitoring and, as early delivery was anticipated, was given dexamethasone to promote fetal lung maturation. Blood tests showed normal leucocytes (14 × 10³/mm³), platelets (155 × 10³/mm³), alkaline phosphatase (ALP; 80 U/L), aspartate aminotransferase (AST; 28 mU/ml), alanine aminotransferase (ALT; 30 mU/ml), haemoglobin 97 g/L (with normal iron studies), whilst her creatinine was 95 μmol/L, which was high for her stage of pregnancy. She was initially stable but by the fourth day of her admission had developed hypertension, marked peripheral oedema and oliguria. No proteinuria was detected, but her platelets had fallen to 105 × 103/mm3.
Management and treatment
An intravenous magnesium sulphate infusion was started, and the obstetric team decided to proceed with urgent operative delivery because of maternal deterioration. Immediately before her planned spinal anaesthetic she had a short tonic-clonic seizure; an emergency caesarean section under general anaesthesia was then performed. Surgery was complicated by major haemorrhage requiring multiple uterotonics, transfusion of four units of packed red cells (PRC) and two units of cryoprecipitate, guided by arterial blood pressure monitoring, blood gases and thromboelastography (TEG).
Post-operatively, whilst still intubated and ventilated, she was transferred to the Intensive Care Unit (ICU) for management by a multidisciplinary team of obstetricians, obstetric anaesthetists, critical care physicians, nephrologists, haematologists, and midwives. Even with an adequate intravascular volume, the patient remained acidotic and anuric, and renal replacement therapy (RRT) was instituted. Despite propofol sedation and therapeutic levels of magnesium, ongoing fitting was observed, alongside marked hypertension. Lorazepam, levetiracetam and phenytoin were required to achieve seizure control, with labetalol and hydralazine to manage her hypertension. Laboratory results from the time of ICU admission showed highly elevated ALT and AST with thrombocytopenia and microangiopathic haemolytic anaemia on the blood film. Seizure suppression was confirmed on electroencephalogram whilst an MRI scan of her head showed very small cortical infarcts but no other lesions.
Over the next three days, sedation was gradually weaned off and the patient was extubated. The hypertension gradually subsided and there was renal recovery. The patient was discharged back to labour ward. Phenytoin was stopped whilst an inpatient and levetiracetam was weaned after she was discharged home.
Discussion
Haemolysis, elevated liver enzymes and low platelets (HELLP) syndrome
HELLP syndrome is a rare but life-threatening pregnancy-related disease. Reports show that it is one of the most common pregnancy-related causes of ICU admission in the UK, and the latest MBBRACE report suggests around a third of deaths from hypertensive disorders of pregnancy are due to HELLP.1,2 It occurs in about 0.5%–0.9% of all pregnancies and complicates 10–20% of pre-eclamptic pregnancies. 3
Aetiology/pathophysiology
Many investigators consider HELLP syndrome to be a severe form of preeclampsia, but the relationship between the two disorders is controversial. Unlike preeclampsia, up to 30% of women with HELLP syndrome will not have hypertension or proteinuria, and pre-eclampsia may only partially manifest prior to the clinical presentation of HELLP, as in this case. 4 The pathogenesis of HELLP remains unclear, but evidence from many studies supports the involvement of immunological dysfunction. 5 Risk factors include multiparity, white ethnic group, and older maternal age. Two thirds of the cases are diagnosed antenatally, usually in the third trimester. It is uncommon to observe clinical features of HELLP syndrome after 48 hours from delivery, but it may occur up to seven days post-partum. 6
The main pathological changes in HELLP syndrome include vasospasm, endothelial injury and vascular fibrin deposition with platelet aggregation and consumption. This leads to hepatic sinusoidal obstruction, intrahepatic vascular congestion with end-organ ischaemia, and ensuing hepatic necrosis occasionally causing fulminant liver failure. Hepatic rupture can occur if intrahepatic pressures exceed that which Glisson’s capsule can withstand. 3
Diagnosis
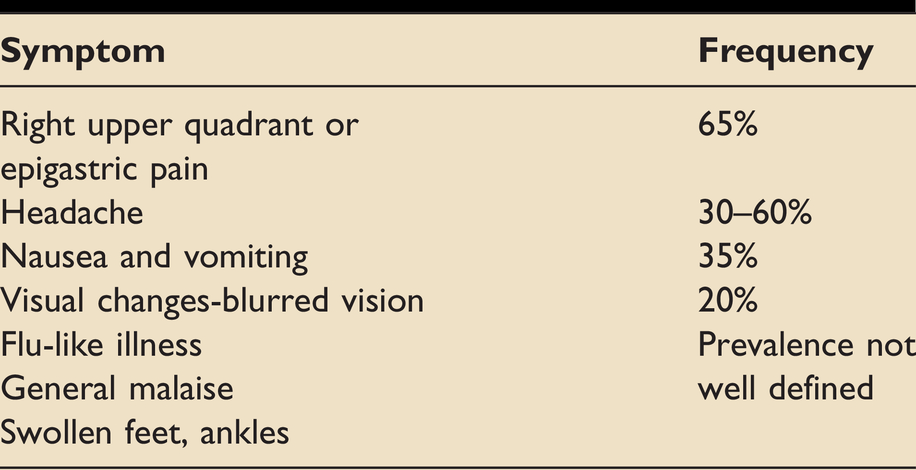
The symptoms of HELLP are listed in Table 1.3,7 HELLP syndrome may be difficult to diagnose, especially when hypertension and proteinuria are absent. Its symptoms are sometimes mistaken for gastritis, respiratory infection, other hepatobiliary diseases (including those related to pregnancy), pyelonephritis and acute pancreatitis. 4 Spontaneous rupture of a subcapsular liver haematoma should always be suspected in cases of acute onset epigastric pain, backache, right shoulder pain, anaemia, and shock. 8 Radiological imaging with ultrasound and/or MRI (considered safer during pregnancy) may be preferable to computed tomography (CT) prior to delivery. Neuroimaging is particularly helpful in the investigation of seizures and can aid clinical diagnosis through the exclusion of subarachnoid haemorrhage (SAH), ischaemic stroke, tumours, cerebral venous thrombosis, and Posterior Reversible Encephalopathy Syndrome (PRES). Cranial CT presents a minimal radiological risk to the fetus. 9
Common symptoms in HELLP syndrome.
Diagnostic criteria for HELLP syndrome are based on a series of laboratory results indicating microangiopathic haemolytic anaemia (MAHA). Currently there are two major definitions in use (Table 2). Morbidity and mortality are higher in cases of complete versus partial HELLP syndrome, with diminishing platelet count being useful in prognostication. 10 Given the overlap between pre-eclampsia and HELLP some centres have suggested using Placental Growth Hormone (PlGF) to triage women who fit into the varied spectrum of hypertensive disorders of pregnancy. 11
Definition and classification of HELLP syndrome.

Investigations
The constellation of advanced pregnancy or very recent delivery, MAHA, deranged LFTs and features overlapping preeclampsia strongly suggest HELLP. However, haemorrhagic shock, coagulopathy and organ dysfunction that may follow a difficult delivery can make it difficult to interpret vital signs and laboratory parameters such as transaminases, prothrombin time and lactate. The picture may be further confused by pre-existing hypertension or liver disease. There are some differential diagnoses with very different treatment strategies which need to be considered (Figure 1). The absence of MAHA in a peripartum patient with thrombocytopenia is a useful indicator to seek an alternative diagnosis (Table 3). Although peripartum sepsis is frequently associated with haemostatic abnormalities, unless it is severe enough to progress to disseminated intravascular coagulation (DIC) it does not cause MAHA.
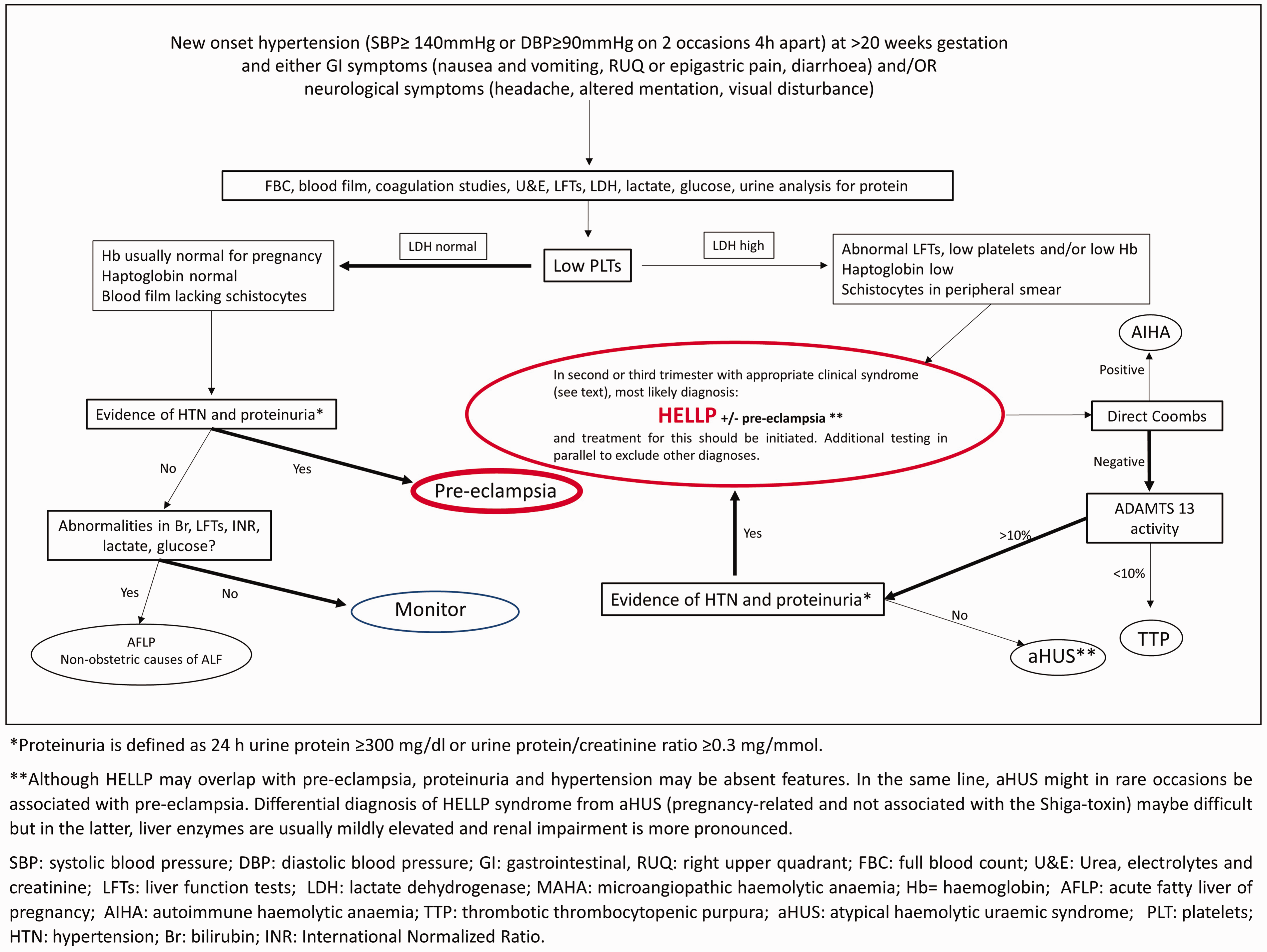
Differential diagnostic approach in clinically suspected pre-eclampsia/HELLP; suggested algorithm. Flowchart representation of the investigations (rectangles) used to help differentiate between the preeclampsia/HELLP spectrum (red oval shapes) and other diagnoses (black oval shapes). In the appropriate clinical content (top of the figure) and following initial investigations (top rectangle), the critical step in differential diagnosis is evidence of thrombocytopenia with (right arm) or without (left arm) MAHA features. Altered thickness of ovals and arrows indicates the likelihood of diagnosis and test results (more likely=thickest). Management plan depends on the diagnosis (see text for details), but in the absence of severe adverse features simple close monitoring may be advised (blue oval shape).
Differential diagnosis of HELLP syndrome.
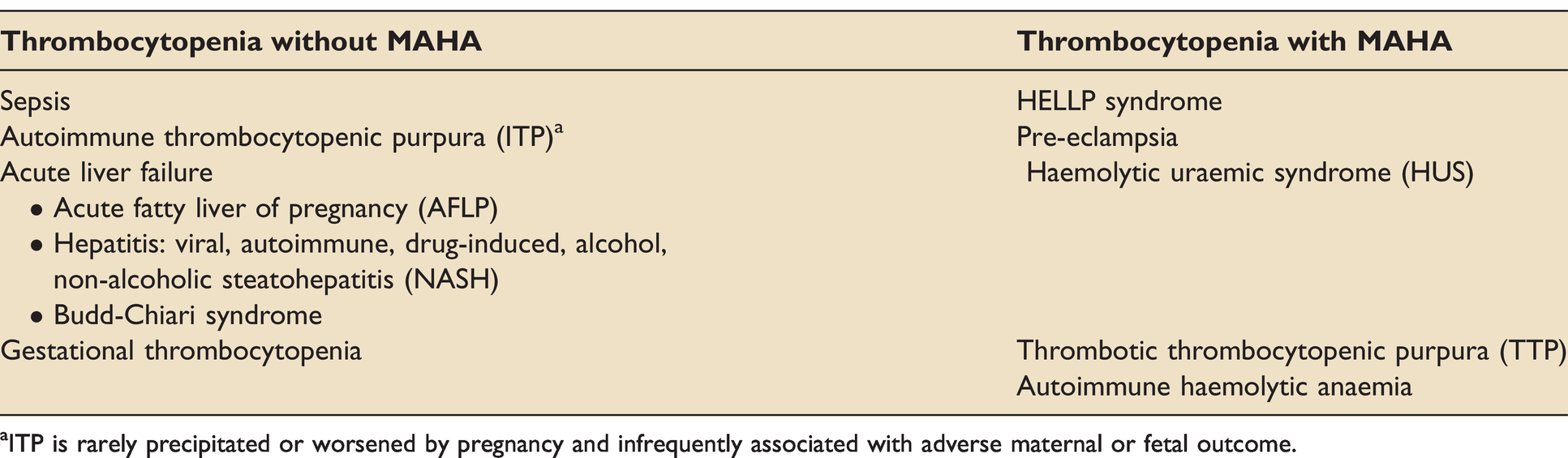
ITP is rarely precipitated or worsened by pregnancy and infrequently associated with adverse maternal or fetal outcome.
In pregnant patients with MAHA, differentiating HELLP from atypical haemolytic uraemic syndrome (aHUS) and thrombotic thrombocytopenic purpura (TTP) can also be challenging. 12 It is important to differentiate between TTP-aHUS and HELLP; TTP and aHUS require plasma exchange and glucocorticoids, and platelet transfusions will exacerbate TTP, increasing the risk of neurological and cardiovascular events and death. 13 In patients where suspected HELLP does not improve within 3 days of delivery, or they have persistent/worsening renal or neurological function, or it starts more than seven days after delivery, an alternative diagnosis should be considered. 12 Liver function tests are usually mildly elevated in TTP and HUS compared to patients with HELLP syndrome, whilst proteinuria is absent in HUS and TTP, but present in most HELLP cases. 12 TTP is rare in pregnancy, but occasionally occurs. Low levels of a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS13) is strongly indicative of TTP.14,15 Clearly, close liaison between obstetricians, haematologists, renal, hepatology, critical care physicians and anaesthetists is essential to make a correct diagnosis and manage appropriately.
Acute liver failure (ALF) can occur as a consequence of HELLP or acute fatty liver of pregnancy (AFLP), but non-obstetric causes should also be excluded, including drugs (especially paracetamol), toxins/poisoning, trauma or decompensation of pre-existing liver disease. Other causes of ALF may be exacerbated by pregnancy such as viral hepatitis or Budd-Chiari syndrome (which can occur acutely in pregnancy); additionally, postpartum haemorrhage (PPH) can cause ischaemic hepatitis which may progress to ALF.
The clinical differentiation of HELLP from AFLP can be difficult, but in AFLP hypertension and haemolysis are less common, thrombocytopenia and transaminitis is usually milder, and functional hepatic impairment can be severe with coagulopathy, hypoglycaemia and hyperammonaemia seen. 14 Low levels of cholesterol and triglycerides, leucocytosis and a more profound jaundice is also usually seen with AFLP. 16 Anti-thrombin III levels are severely impaired in AFLP and MRI may be of use in differentiating between the two clinical entities. Patients should be monitored for the development of hypoglycaemia, pancreatitis and diabetes insipidus. 17 In general, patients with peripartum causes of liver impairment tend to improve, but progression to liver failure in HELLP is still associated with a 11.5% mortality rate. Notably, King’s College criteria are poor predictors of death or need for liver transplantation in this cohort of patients and the presence of encephalopathy and a high lactate are better predictors of disease severity. 18
Treatment and management
Definitive treatment of HELLP syndrome is delivery of the fetus and placenta. 19 The decision to deliver the fetus must balance the maternal and fetal risks. Thus, a pregnant patient with HELLP syndrome admitted to the ICU should trigger multidisciplinary care, which includes fetal monitoring, potential labour and a delivery plan. Equipment for an emergency bedside caesarean delivery should also be readily accessible. Patients with preeclampsia and HELLP syndrome may have airway oedema and appropriate specialist expertise is essential. 20 Cornerstones of management include blood pressure control (when over 140/90 mmHg), correction of abnormal coagulation and management of seizures. Antihypertensives with a robust safety profile in pregnancy include labetalol, hydralazine and nifedipine. 21 Administration of obstetric-specific magnesium sulphate infusion regimes for seizure prophylaxis is essential. 14 Seizures are usually controlled with magnesium sulphate, but rarely other anticonvulsants, such as benzodiazepines or anaesthetic induction agents, may be required. Magnesium levels are rarely monitored but this is a necessity when kidney function is impaired, or seizures are uncontrolled and adjusted levels of infused magnesium are administered. 22 Continuous magnesium (usually for 24 hours) administration and assessment for toxicity (loss of patellar reflexes, diminished respiratory rate and urinary output) is an important element of standard care in these patients. The critical care management of pregnant patients require the additional consideration of the fetus and placenta, which can be also harmed by treatments intended to benefit the mother. The uteroplacental blood flow is maternal pressure dependent and not autoregulated thus, a significant drop in maternal blood pressure by antihypertensives and sedatives may decrease placental perfusion causing fetal compromise. 23 Carers should also be alerted to the deleterious hypotensive effects of aortocaval compression by the gravid uterus and its management with a tilt.
Due to endothelial dysfunction and a risk of pulmonary oedema, a restrictive fluid strategy, as used in preeclampsia, is advocated. This is supported by the latest MBBRACE report which highlights that greater attention to fluid therapy has coincided with a disappearance in mortality due to pulmonary oedema and renal failure, both common in the past. However fluid management is more challenging where there is concurrent haemorrhage with hypovolaemia or coagulopathy. 14 Nevertheless, the restoration of circulating volume following haemorrhage is essential, with a preference for using blood products to avoid coagulopathy if haemorrhage is ongoing. Additional fluid therapy should be based on the replacement of fluid losses and guided by appropriate haemodynamic monitoring, with specific focus on stopping fluid replacement and moving to a restrictive strategy once the patient is euvolaemic. 24 Oliguria is a key clinical feature of HELLP and PET but overzealous fluid administration to try and drive urine output may lead to iatrogenic fluid overload and pulmonary oedema. Repeated and careful clinical assessment is therefore imperative, and the use of advanced haemodynamic monitoring might help avoid over-resuscitation. However, the dynamic state of the peripartum period coupled with the rarity of HELLP mean that few large studies of cardiac output monitoring have been conducted in this area. Our experience includes the use of focussed echocardiography alongside serial clinical examination, metabolic assessment (lactate and central venous oxygen saturations) and repeat straight-leg raise tests.
Corticosteroid administration for fetal lung maturation is well-established. 25 However, its role in maternal management is not clear. Improvements in maternal platelet count, liver enzyme levels, urine output and various cytokine levels have been reported following steroid administration, but this has not been demonstrated to improve maternal outcomes. 26 Plasma exchange (PLEX) has been used in patients with refractory disease with case reports suggesting effectiveness, although this remains essentially experimental. 19 Regimes have included 24–48-hour exchanges until there is clinical and/or biochemical improvement. Complications include increased infection rates so meticulous attention to preventing this is required. 14
Maternal and neonatal outcomes
Maternal mortality in HELLP may reach up to 30% and is increased with complications, with risk factors for death including severe disease, multiorgan failure and concurrent infection. 14 Complications of HELLP include those related to coagulopathy (DIC, subcapsular liver haematoma), acute kidney injury, pulmonary oedema, neurological events (eclampsia, stroke, PRES and retinal diseases) and feto-placental complications (placental abruption, fetal loss). DIC is possibly the most common complication, with a reported incidence of around 25%. 27 Acute respiratory distress syndrome (ARDS) and liver haematoma/rupture occur in approximately 1% of cases, and both have a high mortality.28,29 Liver rupture may be treated conservatively, with surgery, or by transplantation; all have been reported as successful management options.8,30
The perinatal mortality rate in HELLP is in the rage of 7.4%–34% of cases, linked to gestational age at delivery. 19 Complications include intrauterine growth retardation, preterm delivery, intracranial bleeding, thrombocytopenia and neonatal respiratory distress syndrome.
In the long term, women who develop HELLP syndrome are at increased risk of hypertensive disorders in subsequent pregnancies and the rate of recurrent HELLP syndrome ranges from 2% to 19%. 14 HELLP is also associated with hypertension and increased risk of cardiovascular disease in later life. 31 Maternal mental health disorders, depression, anxiety and memory impairment, are also increasingly recognised. 32
In conclusion, HELLP is a rare but serious complication of pregnancy. Its diagnosis is often challenging, and it may be difficult to differentiate from other diseases with somewhat different clinical management. Multispecialty input is essential for successful management of these patients. Although these patients frequently require intensive care admission, the unique pathophysiology of HELLP and preeclampsia mean management, especially of fluids and magnesium, needs to be tailored appropriately.
This article covers
Footnotes
Author's Note
Mansoor Nawaz Bangash is also affiliated with Department of Critical Care, University Hospitals Birmingham NHS Foundation Trust, Birmingham, UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.