
Abstract
Objective
To investigate the clinical characteristics and prognoses of patients with postpartum acute kidney injury (PPAKI).
Methods
We retrospectively reviewed the clinical presentations, laboratory examinations, treatments, and outcomes of patients with PPAKI admitted to our hospital from January 2013 to December 2017. We then analyzed the clinical characteristics and prognoses of the mothers and their infants.
Results
Of 37 patients diagnosed with PPAKI, 26 (70.3%) received treatment in the intensive care unit, mainly for hemolysis, elevated liver enzymes, low platelet count (HELLP) syndrome (28/37, 75.7%), pre-eclampsia (26/37, 70.3%), and postpartum hemorrhage (22/37, 59.5%). Twenty patients required renal replacement treatment (RRT), but renal recovery times were similar in the RRT and non-RRT groups. Renal function recovered completely in 30 patients (81.1%) and partially in one patient (2.7%), and was not re-examined in two patients (5.4%). Three patients (8.1%) were lost to follow-up. Only one patient (2.7%) remained dialysis-dependent, and no maternal deaths occurred. The preterm birth, low birth weight, and infant survival rates were 70.7% (29/41), 68.3% (28/41), and 78.0% (32/41), respectively.
Conclusion
RRT does not reduce renal recovery time compared with non-RRT. Overall, the prognoses of both mothers and their fetuses are good following treatment for PPAKI.
Keywords
Introduction
Acute kidney injury (AKI) refers to the sudden loss of renal function. It is characterized by a sudden and usually reversible decrease in glomerular filtration rate, 1 which in turn results in increased serum concentrations of products that are normally excreted from the kidney, including creatinine, blood urea nitrogen, and other waste products. 2 The incidence of AKI in developed countries varies from 3% to 18.3%. 3 A previous study indicated that hospitalizations for AKI increased by 139% among adults with diabetes and by 230% among those without diabetes in the US from 2000 to 2014. 4 In Asia, recent reports demonstrated that AKI accounted for 34.8% and 52.9% of critically ill intensive care unit (ICU) patients in Laos and Thailand, respectively,5,6 while the reported incidence of AKI in China is 6.9% to 11.6%,7,8 with an estimated 2 million people diagnosed with AKI in 2013. 8 AKI thus causes a huge medical burden globally.
AKI can be particularly challenging to treat during pregnancy, and a thorough understanding of the causes of AKI during pregnancy are necessary to allow appropriate treatment to be administered. AKI can also occur during the postpartum period, when it is referred to as postpartum acute kidney injury (PPAKI). 9 PPAKI can be caused by severe pregnancy-associated complications (e.g., pre-eclampsia, hemolysis, elevated liver enzymes, low platelet count (HELLP) syndrome, atypical hemolytic-uremic syndrome), especially if these complications are present prior to delivery and remain unresolved.10,11 PPAKI is an uncommon but life-threatening condition that affects the health of the mother. PPAKI was reported to account for 60% of all obstetric AKI cases in a study in India; 10 however, its true incidence is difficult to estimate because of variations in the diagnostic criteria used.
Severe PPAKI requiring renal replacement therapy (RRT) has been reported to occur in approximately 1 in 20,000 pregnancies, 12 and this low incidence rate means that there is a lack of clinical research related to PPAKI. The incidence rates of pregnancy complications increase with increasing maternal age, with a corresponding increase in the incidence of PPAKI. Lanzhou University Second Hospital is one of the largest hospitals in Gansu Province, China, with more than 8000 deliveries over the past 5 years. We designed this study to investigate the clinical characteristics and prognoses of patients diagnosed with PPAKI in our hospital over the past 5 years, and analyzed the maternal and infant outcomes to provide evidence to support future clinical guidance.
Patients and methods
This study was approved by the ethics committee of Lanzhou University Second Hospital (2019A-201) and informed consent for treatment was obtained from all patients. Consent for publication was waived based on the retrospective study design. All case details were de-identified. We retrospectively identified patients who met the following diagnostic criteria for PPAKI: (1) in line with the 2012 Kidney Disease Improving Global Outcomes (KDIGO) AKI diagnostic criteria: renal function suddenly decreased within 48 hours, mainly manifesting as an increase in the absolute value of serum creatinine to >0.3 mg/dL (≥26.5 µmol/L), an increase in serum creatinine of at least 50% (1.5 times the baseline value), or urine volume <0.5 mL/kg/hour for more than 6 hours; (2) AKI occurring immediately after delivery for up to 6 weeks postpartum; and (3) normal renal function before and during pregnancy.
The following maternal and fetal variables were extracted from our hospital database: demographics, onset time of AKI, symptoms, maternal complications and management, systolic and diastolic blood pressure, serum creatinine levels, RRT and method, renal outcome, health status of the newborn, fetus sex, and birth weight. All women with AKI were followed for at least 1 year after delivery.
Gestational hypertension was defined as elevated blood pressure (≥140/90 mmHg) after 20 weeks of pregnancy, pre-eclampsia was defined as pregnancy-associated hypertension plus proteinuria ≥0.3 g/24 hours, and eclampsia was defined as the occurrence of new-onset, tonic–clonic seizures or coma in pregnant women with pre-eclampsia. 13 HELLP syndrome was defined as hemolysis, elevated liver enzyme levels, and low platelet count, and postpartum hemorrhage was defined as postpartum uterine or vaginal bleeding of ≥400 mL. Renal prognosis was categorized as described previously, 8 with complete recovery if the serum creatinine concentration decreased to within the normal range, and partial recovery if renal function improved, but with persistently elevated serum creatinine levels in dialysis-independent patients.
The data were analyzed statistically using SPSS Statistics for Windows, Version 21.0 (SPSS Inc., Chicago, IL, USA). Normally distributed data were expressed as mean ± standard deviation, and were compared between the two groups using independent t-tests. Non-normally distributed data were expressed as median and interquartile range, and were compared using the non-parametric Wilcoxon’s rank sum test. Numerical data were expressed as percentages and compared using χ2 tests. For all tests, P<0.05 was considered statistically significant.
Results
Thirty-seven cases met the diagnostic criteria for PPAKI during the 5-year study period, including 16 primipara and 21 multigravidae. Of these 37 PPAKI patients, 26 (70.3%) required treatment in the ICU. The patients’ ages ranged from 17 to 46 years (mean 29.65 ± 6.70 years). Thirty-two patients were Han Chinese and five were from ethnic minorities. Pregnancies ended in cesarean section in 27 patients (73.0%) and spontaneous vaginal delivery in 10 (27.0%). All cases of PPAKI occurred within 1 week after delivery.
Etiology of PPAKI
The patients had various conditions that might have contributed to the development of PPAKI, with many patients having multiple complications (Tables 1 and 2).
Etiology of postpartum acute kidney injury.

PPAKI, postpartum acute kidney injury; HELLP, hemolysis, elevated liver enzymes, low platelet count.
Diagnoses of all patients with postpartum acute kidney injury.

PPAKI, postpartum acute kidney injury; MOF, multiple organ failure; TMA, thrombotic microangiopathy; ATN, acute tubular necrosis; AFP, acute fatty liver during pregnancy; PPH, postpartum hemorrhage.
Clinical manifestations and renal pathology
Serious clinical manifestations occurred in many PPAKI patients, including oliguria and anuria, coma, eclampsia, and cardiac arrest, while other cases presented with symptoms such as nausea, vomiting, abdominal pain, shortness of breath, headache, blurred vision, and other symptoms (Table 3). Three patients received renal biopsy because of persistent renal failure and one because of persistent proteinuria. Of these four patients, one had thrombotic microangiopathy accompanied by acute tubular necrosis, one had intracapillary proliferative glomerulonephritis, one had acute tubular necrosis, and one had a mild glomerular lesion. Notably, the patient with persistent proteinuria had prolonged proteinuria (1.0–0.5 g/24 h) for 4 months, and her kidney function recovered (serum creatinine 52 µmol/L) in the third month after delivery.
Clinical manifestations.

PPAKI, postpartum acute kidney injury; BP, blood pressure.
Treatment and kidney function recovery
Among the 37 PPAKI cases, 20 (54.1%) received RRT while the remaining 17 (45.9%) were not treated with RRT. Other treatments included plasma transfusion (26/37, 70.3%), red blood cell transfusion (24/37, 64.9%), platelet infusion (22/37, 59.5%), and glucocorticoid treatment (7/37, 18.9%). Additionally, 14 patients (37.8%) received antibiotics for anti-infective treatment. RRT was predominantly administered as continuous RRT (CRRT; 100%), and 15 patients (40.5%) underwent sequential hemodialysis after CRRT. Three patients (8.1%) required blood purification treatment.
The characteristics and outcomes of patients treated with and without RRT are shown in Table 4. There was no significant difference in renal recovery times between the RRT and non-RRT groups. The median recovery times in the non-RRT and RRT groups were 15 and 21 days, respectively. However, the mean maximum serum creatinine concentration was significantly higher in the RRT group compared with the non-RRT group (P<0.001). There were no significant differences in other factors including maternal age, gestational age, cesarean delivery, highest blood uric acid, minimum hemoglobin level, and lowest platelet count between the RRT and non-RRT groups (Table 4).
Characteristics and outcomes of patients treated with and without renal replacement therapy.
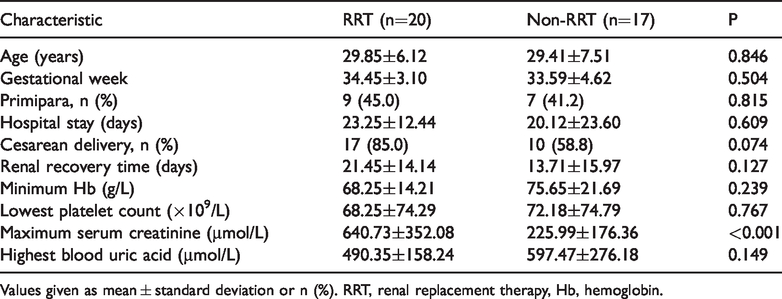
Values given as mean ± standard deviation or n (%). RRT, renal replacement therapy, Hb, hemoglobin.
AKI stages and prognoses in PPAKI patients
According to the 2012 KDIGO Guidelines for AKI staging, 1 20 patients (54.1%) met the criteria for stage 3 AKI. The median hospital stay was 23 days, and the median time to recovery of urine volume was 14 days. Renal function outcomes are presented in Table 5.
Acute kidney injury staging and kidney function outcomes in patients with postpartum acute kidney injury (n=37).
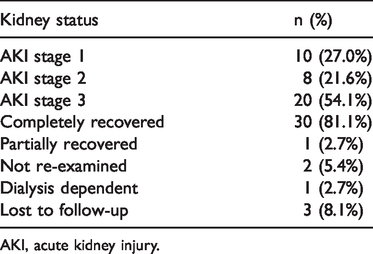
AKI, acute kidney injury.
Fetal health and prognosis
The 37 PPAKI patients included four twin pregnancies, and we therefore assessed the outcomes for 41 fetuses. Twenty-four fetuses (58.5%) were female and 17 (41.5%) were male. There were 29 preterm births (70.7%) with an average gestational age of 32.38 ± 3.19 weeks, and 12 term births (29.3%). Of the 41 fetuses, eight died in utero at an average gestational age of 30.25 ± 4.80 weeks. The infant survival rate was 78.0% (32/41), and one infant died 2 hours after birth. The other infants were delivered healthy and well-developed.
Discussion
PPAKI is a rare but life-threatening condition, but good outcomes are possible with appropriate treatment. We retrospectively summarized the clinical manifestations, treatments, and prognoses of 37 patients with PPAKI.
Although cases of pregnancy-related AKI are generally decreasing worldwide, 14 incidences in the United States, Canada, and other developed countries have increased in recent years. 15 In a study in France, out of 182 of 59,302 women admitted to ICU because of postpartum complications, 68 had AKI. 11 Although there were no deaths in the present study, 54.1% of cases reached stage 3 AKI, and 70.3% required ICU treatment.
The main causes of PPAKI in developed countries are currently hypertensive disorders of pregnancy such as pre-eclampsia and thrombotic microangiopathy, 15 while infection and bleeding remain the most common causes in some developing countries.16,17 Previous studies suggested that the most common causes of pregnancy-related AKI in China were pregnancy-induced hypertension and postpartum hemorrhage, 18 while the present study found that HELLP syndrome and pre-eclampsia were the most frequent causes. In addition, PPAKI patients often experience multiple complications that jointly promote the occurrence of PPAKI. Furthermore, the incidence of pre-eclampsia was high among PPAKI patients who needed dialysis after delivery. 19 The current results were consistent with these previous studies, indicating that the etiology of PPAKI typically involves multiple factors.
The etiology and pathogenesis of PPAKI are complicated and currently unclear. During pregnancy, the mother’s blood flow increases, together with a 60% to 80% increase in cardiac output immediately after delivery, followed by a rapid decrease within 10 minutes to values approaching normal at 1 hour postpartum.20,21 It has been postulated that severe hypovolemia (due to postpartum hemorrhage) and complex pregnancy-related coagulopathy may lead to PPAKI. In addition, levels of atrial natriuretic peptide and brain natriuretic peptide are both increased postpartum, and both have potent diuretic effects and help mediate the diuresis noted in the early postpartum period. 21
RRT plays an important role in the treatment of severe AKI. A study in India showed that 88.2% of patients with PPAKI required RRT treatment, 22 while a Canadian study reported that 53.7% of patients with pregnancy-related AKI who required dialysis had PPAKI. 19 The present study also showed that more than 50% of patients needed RRT treatment, but there was subsequently no significant difference in renal recovery times between patients with and without RRT. To the best of our knowledge, no studies have investigated the effect of RRT on kidney function recovery time in PPAKI patients. The timing of RRT in patients with PPAKI needs to be evaluated comprehensively according to each patient’s condition, and optimal timing standards require further investigation.
Previous studies showed relatively good outcomes in women with pregnancy-related AKI after active treatment.18,19 In the present study, 81.1% of patients experienced complete recovery of renal function, with only one case (2.7%) of partial recovery and one patient (2.7%) who remained reliant on dialysis. There were no deaths, consistent with previous studies. 22
To the best of our knowledge, no follow-up studies have reported on the prognoses of infants born to mothers with PPAKI. In addition to reporting the health statuses of the fetuses, the current study also followed-up on the survival and growth of the infants for at least 1 year after birth. Although the incidence rates of preterm delivery and low birth weight were high (70.7% and 68.3%, respectively), the survival rate was 78.0% (32 cases), with eight intrauterine deaths (19.5%). All newborns were healthy and exhibited good growth and development.
The present study had some limitations. First, it was a single-center retrospective study with a small sample size. Second, some prenatal examinations were not carried out in our hospital, and some prenatal data were therefore missing. Third, some patients were lost to follow-up, and long-term follow-up data were therefore not available for these patients. Finally, we could not acquire the histopathology images for the patients who underwent biopsy.
In conclusion, we retrospectively reviewed 37 cases of PPAKI and summarized the causes, manifestations, treatments, and prognoses of the disease. We also reported on the health of the fetuses of mothers with PPAKI and on their post-birth development. The results of this study may provide guidance to clinicians to aid the management of patients with PPAKI, as well as contributing information regarding the prognosis of the disease.
Footnotes
Availability of data and materials
The datasets used during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.