
Abstract
The COVID-19 pandemic of 2020 imposed significant strain on critical care services worldwide. The South London region experienced the largest numbers of critical care admissions in the United Kingdom with King’s College Hospital one of the busiest centres. This article outlines, using a descriptive narrative, the significant changes that occurred within King’s Critical Care as a result of the pandemic and the decisions that were taken to provide effective co-ordination and control to the expanded service, in part drawing on the military experience of two of the authors. The wider context of crisis and major incident leadership and management is also discussed contrasting different approaches used in civilian and military settings.
Introduction
In the first six months of 2020 healthcare systems worldwide came under enormous strain as the COVID-19 pandemic produced an unprecedented demand on hospital, and especially critical care, services. Within the United Kingdom, the South East London region recorded the highest numbers of COVID-19 related critical care admissions between March and June 2020, with King’s College Hospital one of the busiest centres nationally. 1 This surge in patient numbers required a dramatic expansion of critical care capability and added greatly to the complexity of service provision. In order to ensure that clinical management continued to be delivered to the best possible standard our department rapidly reviewed and revised existing management and leadership structures and developed a new Command, Control and Communication (C3) framework. Two of the authors who were involved in the development of this framework are serving military medical officers and aspects of the resulting structures are based around an adaptation of military C3 concepts.
We present a descriptive account of the approach and decisions taken by King’s Critical Care in tacking the crisis and discuss them in the wider context of health care leadership theory.
King’s critical care prior to COVID-19
Immediately before the COVID-19 surge King’s College Hospital in South East London had capacity for sixty nine critically ill patients in four distinct intensive care units. King’s Critical Care provides support for a wide range of patient groups including cardiothoracic surgery, liver transplant and specialist hepatology, an acute heart attack and cardiac arrest centre, major trauma, haematological malignancy including bone marrow transplantation and the full range of neurosurgery and neuroscience services.
Nursing staff for each unit were managed individually by that units matron and senior nursing leadership team, with a twice daily staffing meeting allowing flexibility in allocating staff between units if required. Junior medical staff were allocated to specific units for blocks of time and consultant grade doctors generally worked across multiple units as part of an annualised job plan. A separate consultant led outward facing team of clinicians and nurses, termed “iMobile”, provided support to the wider hospital, acting as the initial point of contact for referrals.
Historical critical care bed occupancy rates were usually very close to or exceeding 100% and a full time critical care bed manager was essential in ensuring effective patient flow. Day to day co-ordination of the clinical service was provided by the four duty attending unit consultants and nurses-in-charge alongside the iMobile consultant and critical care bed manager. A daily scheduled bed meeting provided an overview of capacity and served as a forum for general discussion.
Longer term strategic leadership and management was provided by a clinical director, head of nursing and general manager; weekly meetings attended by area and speciality clinical leads and matrons provided the forum for policy making decisions.
Scope of change during the COVID-19 pandemic
At King’s the first patient with COVID-19 was admitted to critical care on 10 March and peak bed occupancy occurred on 11 April when 115 patients were receiving intensive care support. Patients with COVID-19 made up the majority of the patient population during much of April and May but there were still around 20 patients a day within King’s Critical Care receiving treatment for non COVID-19 related conditions. The number of utilisable critical care beds expanded from a baseline of sixty nine to one hundred and sixty four in the week of 20 April (Figure 1). The number of physical areas set up to provide critical care expanded from four at the beginning of March to a peak of nine in the week of 20 April (Figure 2).
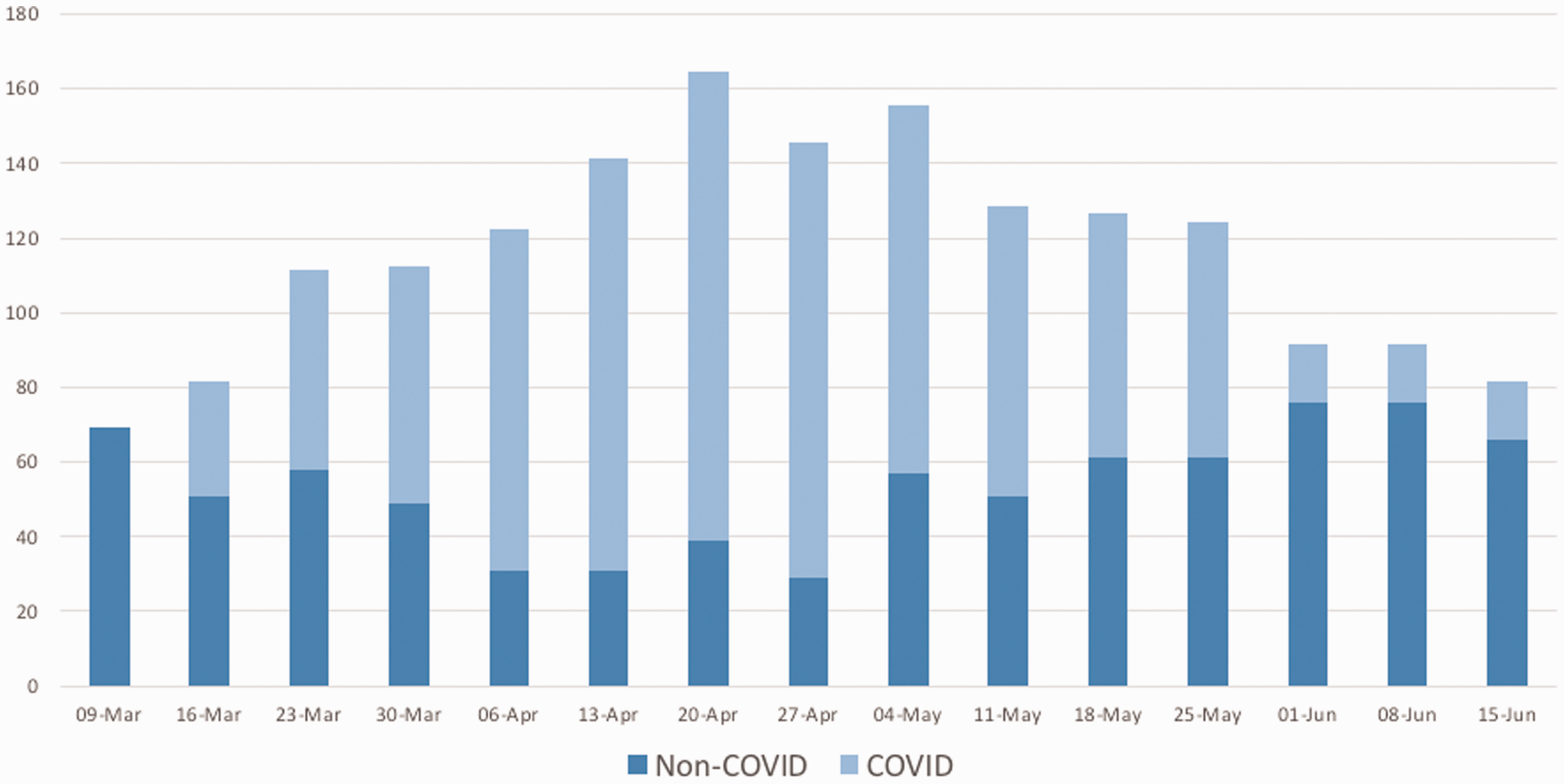
Expansion of critical care beds during the COVID-19 pandemic. Beds are divided into those available for patients with actual or suspected COVID-19 and those for non COVID-19 patients. Numbers shown reflect the maximum number of beds at any time during the 7 day period.
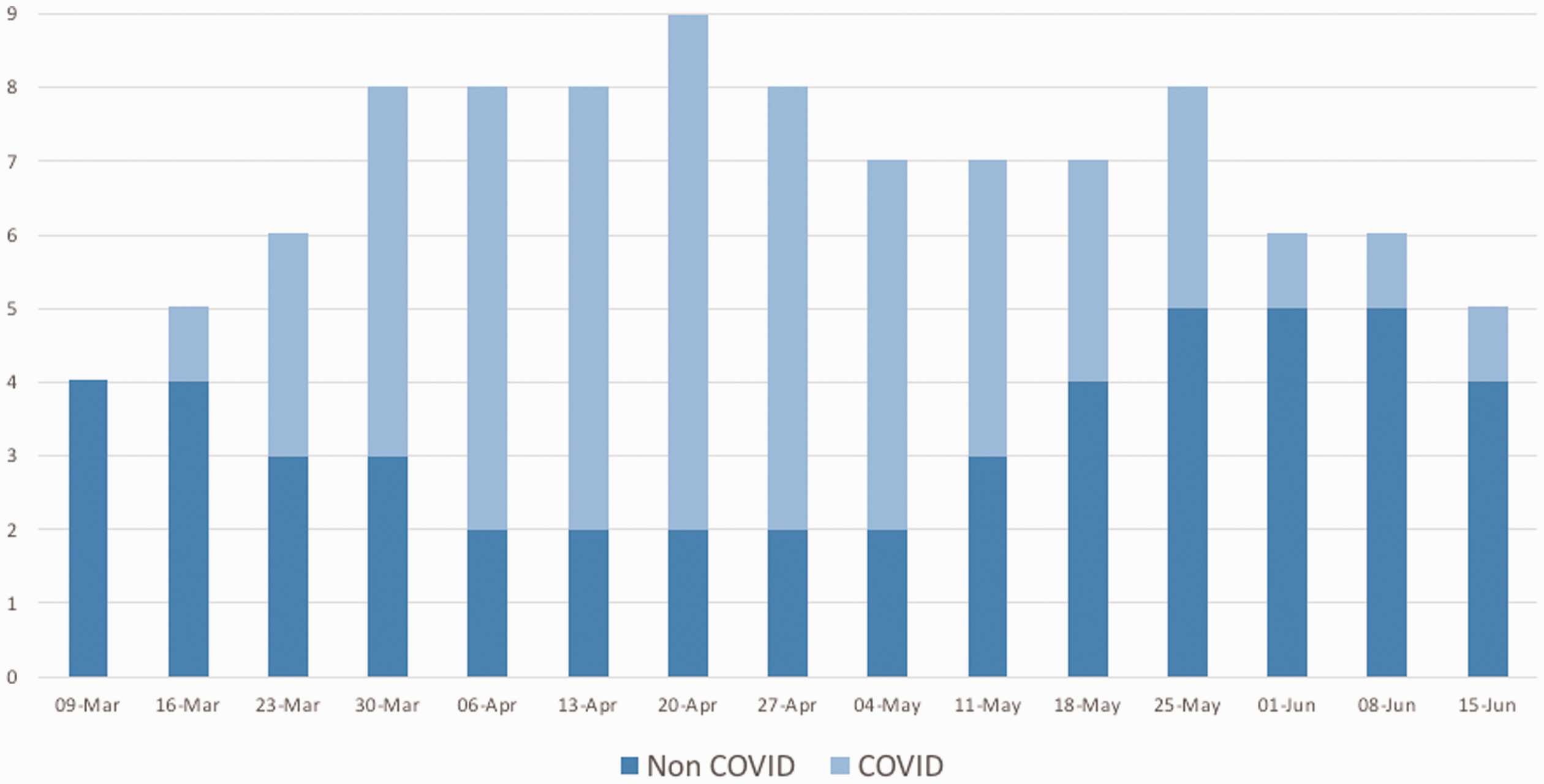
Expansion of clinical areas dedicated to the management of critically ill patients during the COVID-19 pandemic. Areas are divided into those admitting patients with actual or suspected COVID-19 infection and those reserved for patients with other conditions. Numbers shown reflect the total areas open during the 7 day period in question.
A significant expansion of the nursing and medical workforce was required in order to support this increased capacity, illustrated in Figure 3. Nursing numbers increased by 32% from baseline and the dilution of experienced staff, increase in patient numbers and expansion of the physical footprint resulted in a reduction in the usual ratio of one critical care nurse to one patient. The worst ratios were recorded in the weeks commencing 13 and 20 April 2020 when one experienced nurse simultaneously cared for three patients (1:3) and the mean ratio across all critical care areas was 1:2 for the period between 16 March and 8 June.
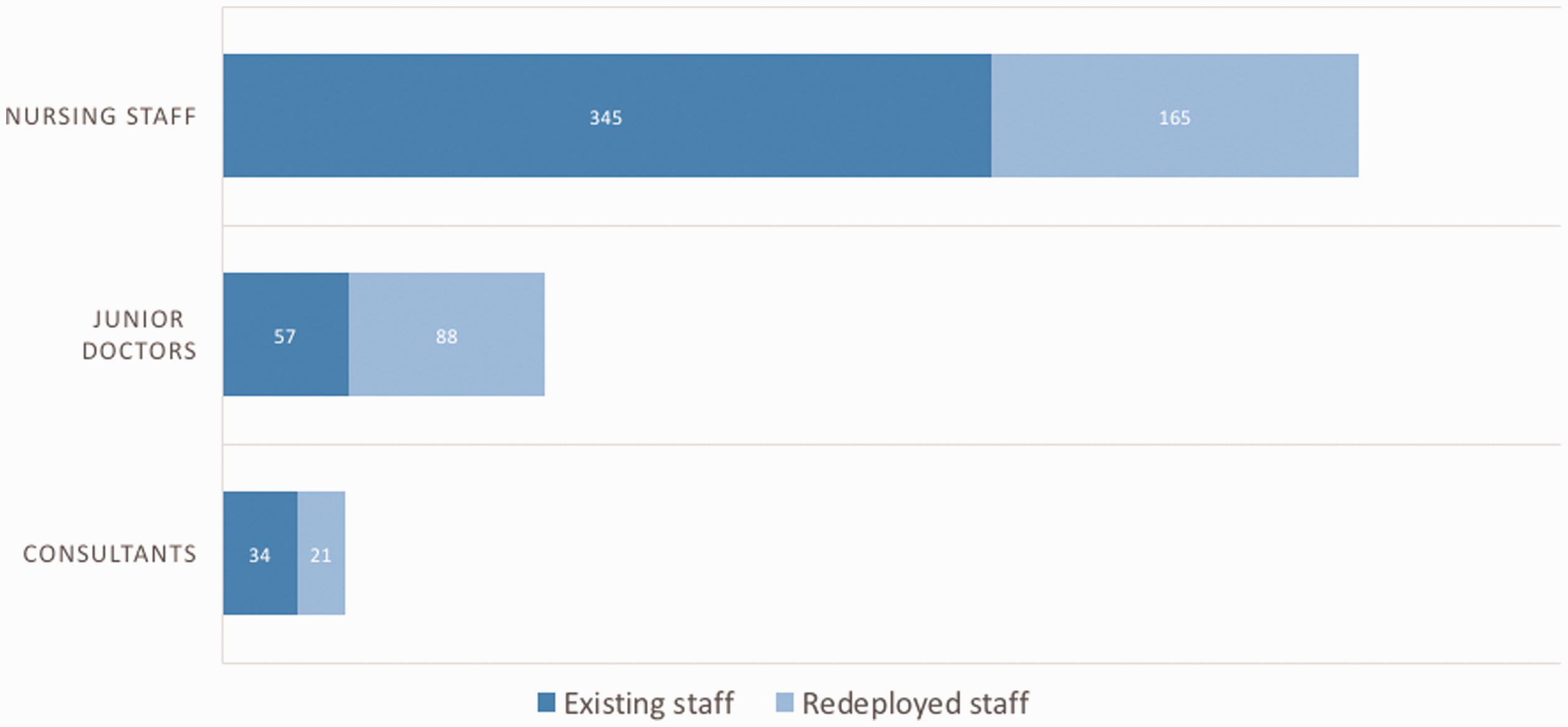
Expansion in critical care staff during the COVID-19 pandemic. Numbers shown reflect the total number of staff prior to the pandemic and the number of staff re-deployed to critical care between March and June 2020.
Numbers of medical staff also increased markedly (Figure 3). The majority of re-deployed consultants were dual trained in intensive care medicine and worked within cardiac or liver transplant anaesthesia. Although there was therefore overlap in terms of skills few had current exposure to general critical care outside of their area of expertise. Of the re-deployed junior doctors
49% had no previous exposure to work within critical care.
Response – Development of the king’s critical care tactical service
The principal factor differentiating King’s Critical Care from many other intensive care facilities is the scale and complexity of the service. Even during normal periods of activity, co-ordinating a service providing nearly 70 beds across 4 units is challenging and, as we have discussed, required a dedicated bed manager and a consultant led external clinical team. However, within days of the first COVID-19 patient being admitted to intensive care it became apparent that the existing leadership and management structure would struggle to cope with the challenge of more than doubling clinical capacity and co-ordinating a service which had expanded almost beyond recognition. The wider Trust management structure adopted a standard NHS major incident response model based around Silver and Gold levels of command for the duration of the crisis, but this model did not really address the dynamic response required within critical care at the unit and pan-unit level. Early in the pandemic we set out broad aims that we wanted a crisis leadership and management model to deliver, shown in Table 1.
Aims of the King’s critical care tactical service.

Our solution comprised three parts. Firstly we created an agile Tactical Team with a remit to provide hour-by-hour co-ordination of the critical care service. The focus of this team was broadly on oversight and co-ordination rather than delivery of clinical management; individual patients requiring intensive care were still reviewed and managed by the externally facing iMobile service but the Tactical Team would decide which clinical area to admit such patients to.
The second component was the creation of a Critical Care Tactical Hub which was envisaged to be a single interface between critical care, other hospital departments and Trust level management. We envisaged a physical space, populated predominantly by non-clinical staff, with specific pre-defined roles that would each support an aspect of service provision, such as workforce, logistics and communication. The idea for the Critical Care Tactical Hub was loosely based on a military staff and command framework. Finally, we formalised the structure and pace of the working day by introducing a new daily work pattern which we termed a Battle Rhythm, again loosely based on a structure used in military organisations to provide command and control on operations.
Tactical team
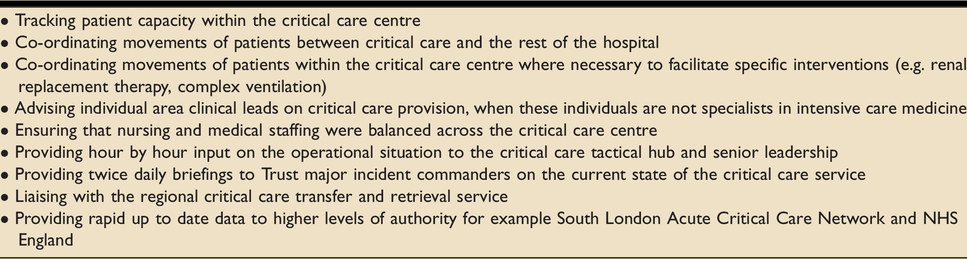
The Tactical Team comprised three individuals; an intensive care consultant, a critical care matron (Band 8) and a critical care bed manager which functioned for twelve hours a day, seven days a week. Functions of the tactical team are shown in Table 2. The principal function of the team was co-ordination, a task that became increasingly complicated as the pandemic progressed and the size of the service increased. Tactical team members were highly mobile, connected by Wi-Fi phones, but constantly moving between clinical areas in order to ensure that the right patients were being managed in the correct location in accordance with their current clinical needs. For example, some areas were universally equipped with critical care ventilators, others had a mixture of anaesthetic machine ventilators which proved sub-optimal in some patients. We intend to fully describe elsewhere the challenge of providing renal replacement therapy during the pandemic; ultimately patients at King’s critical care were managed using three different renal replacement modalities, utilising intermittent haemodialysis and acute peritoneal dialysis in addition to continuous renal replacement therapy; some of these treatments were limited by location. Selecting appropriate patients for each modality and moving them between areas to facilitate treatment required constant action and close co-ordination with other specialties such as renal medicine and anaesthesia.
Functions of the King's Critical Care tactical team.
Many patients required prone positioning to facilitate effective oxygenation and ventilation. The tactical team co-ordinated a multi-disciplinary proning team to enable this treatment. At peak activity, this team positioned or repositioned twenty five patients within a single twelve hour period.
At the outset we identified workforce planning and co-ordination as the biggest challenge of the surge and this proved the case. Of the nine clinical areas within King’s Critical Care at the peak of the surge, only five had an established pre-surge staffing footprint. The situation was compounded by the significant attritional aspect related to staff sickness from COVID-19 infection and self-isolation requirements. It quickly became apparent that even with support from an expanded administration team this role required detailed knowledge of individuals, teams and areas that only senior nursing staff possessed. The role of the command matron during the peak of the surge became almost exclusively one of continuous workforce planning, often carried out in a just in time fashion.
Tactical hub
The initial concept for the Tactical Hub was a central control point for the entire critical care response. We envisaged a team of predominantly non-clinically facing staff who would be brought together in a defined structure to support the tactical team and individual clinical areas. Each member of this team would have clear roles and would form a single point of contact between the clinical teams and the essential support infrastructure that underpinned effective clinical management. Proposed titles for this concept of operations were the “Kings Critical Care COVID Co-ordination Centre” or the “Command Hub” but once operational it quickly came to be known simply as the “Hub”. The Hub was intended as both a physical space and a description of the crisis organisational structure. We considered that even in an era of remote working and improved connectivity having a defined physical space within the hospital was vital to effective command and control and identified a conference room with adequate physical space, computer and communication infrastructure, conveniently located next door to the Trust major incident control room.
We explicitly based the Hub concept on a military staff model of operations which is classically divided into seven sectors, termed J (Joint) 1-7; we utilised five of these domains with most relevance to the situation. Our original intent was to populate the Hub with specifically assigned “desk officers” with individuals rapidly identifiable to any visitors to the Hub by the use of physical signage. Ultimately, this was one area in which our initial aspirations fell short in reality; restrictions imposed by social distancing limited the number of people who could be gathered together in one space and in practice, outside of scheduled meetings, much of the work of the Hub was carried out remotely. J1: Personnel
People are at the heart of any organisation, whether civilian or military and so this was undoubtedly the most important individual domain with overarching responsibility for medical and nursing workforce provision including rota creation and propagation. This was also the part of the hub responsible for staff wellbeing including psychological support, wellbeing and liaising with staff on issues arising around illness, COVID-19 testing, self-isolation and return to work. J2: Operational Intelligence
In the military this domain is responsible for obtaining an up to date picture of the operational battlespace including enemy dispositions and intentions. Effective intelligence depends on accurate contemporaneous data and the response to COVID-19 was no exception. The tactical team collected daily data on bed occupancy, admission rates, number of patients requiring renal replacement therapy; tracheostomy and prone position ventilation. Daily collection of this data enabled effective allocation of patients and resources across the service. Data was shared nationally and with the local critical care sector network in South East London and helped inform regional and national resource allocation.
Underpinning all aspects of operational intelligence was the requirement to collect and synthesise data. At the onset of the pandemic we utilised a computer based clinical information system that covered three of the four existing critical care areas. This was significantly expanded as the pandemic progressed to the point where 77% of critical care beds at peak surge capacity were linked to the clinical information system. Real time availability of clinical data was vital in ensuring that patients were in the optimal clinical area. J3: Current Operations
In the military this domain is responsible for planning and overseeing the conduct of operations; translated to the fight against COVID-19 this Hub area was responsible for continuously planning capacity expansion, deciding on which clinical areas would be opened and later closed and agreeing timescales for these events with the Trust. Existing critical care operational managers and clinical leaders fulfilled this requirement, working closely with the Tactical Team. J4: Logistics
Logistics in a military context is the process of delivering supplies and material to enable effective operational activity. After personnel this was the most crucial aspect of the COVID-19 response as individual hospitals tried to ensure the delivery of a range of equipment and consumables for which the demand had increased rapidly over a short time scale. At King’s, under normal circumstances, each clinical area was responsible for their own stock taking and re-ordering but the rapid expansion in both areas and beds rendered this extremely challenging. We envisaged a central logistics hub for critical care with desk officers responsible for consumables and electro-medical equipment procurement. Specialist pharmacy also interfaced with this area, advising on rates of stock depletion for key drugs, especially sedatives and working with clinicians to incorporate alternative agents into practice. J6: Communication
Communication is regularly identified as an important aspect of leading through a crisis, when the levels of stress, burnout and fear amongst staff can be significant. All staff within King's Critical Care, including those who were redeployed from other areas received daily email updates; which included information on patient numbers within critical care, plans for opening and closing of critical care areas and updates on policies and procedures providing situational awareness to the whole workforce.
Effective and compassionate communication with the relatives and families of critically ill patients is a core part of critical care medicine and nursing. The restrictions on hospital visiting and the frenetic nature of the clinical workload early in the pandemic precluded such communication under most circumstances and was a source of concern to many in our service. Colleagues within King’s Critical Care developed an innovative family communication service which involved senior doctors from re-deployed specialities. These teams communicated with families by phone and video call after being briefed by the attending critical care staff. This was an incredible service which we intend to fully describe elsewhere.
Daily battle rhythm
In a military organisation a battle rhythm describes a set daily cycle of events used by military commanders and their staff to regulate and co-ordinate the activity of a military unit. During the crisis phase of the COVID-19 response we instituted a daily battle rhythm structure to co-ordinate activity across all clinical areas and to effectively integrate the critical care service with the wider hospital and other key specialities. This daily structure is shown in Figure 4.
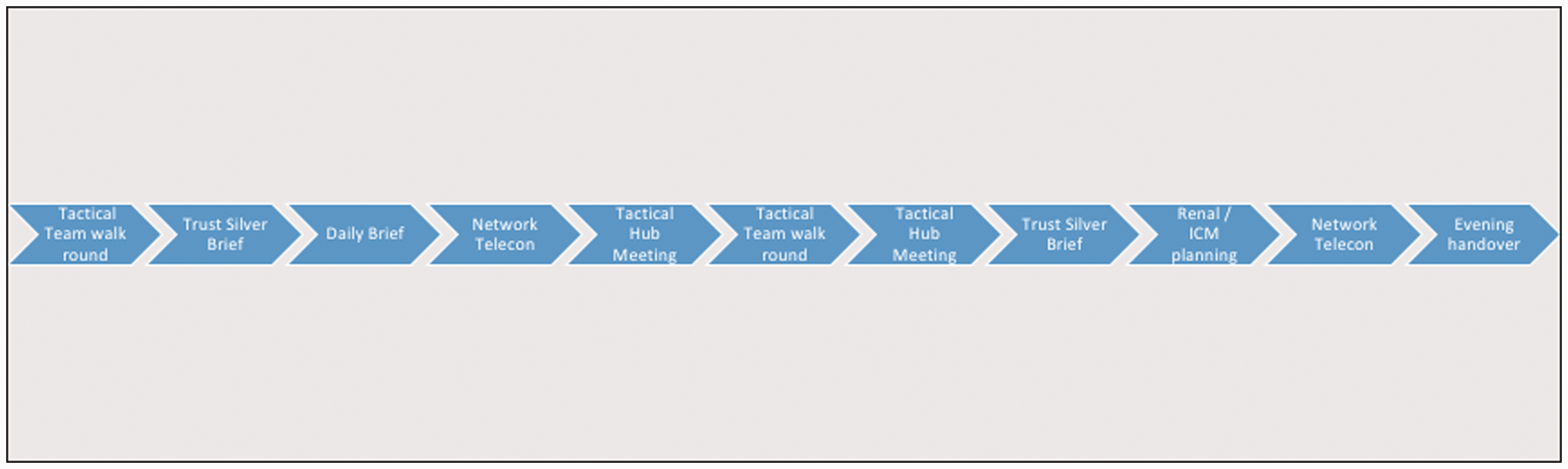
Daily Battle Rhythm adopted by King’s Critical Care during the COVID-19 pandemic. A battle rhythm is a term used by military organisations to describe a predictable pattern of daily tasks undertaken on operations.
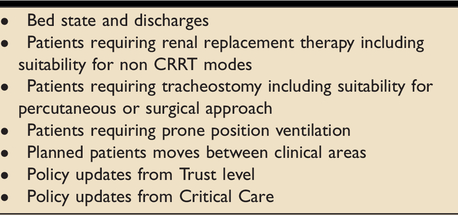
Central to the daily battle rhythm were regular walk rounds of all areas by the Tactical Team in the early morning, afternoon and evening to identify any acute issues; often the tactical consultant would jointly review patients with the area consultant when that individual had been re-deployed to critical care. A daily team briefing; attended by clinical area duty consultants, representatives from renal medicine and maxillofacial surgery, anaesthesia and the lead clinician (doctor or advanced critical care practitioner) from the daily proning team followed a standardised format, shown in Table 3, which ensured that all factors relevant to the delivery of effective patient management were considered systematically on a daily basis.
Structured format for King’s critical care daily briefing during the COVID-19 pandemic.
Other key daily meetings occurred in the Hub, again following a pre-defined agenda based around the individual Hub sectors. Twice daily remote conferencing calls co-ordinated by the South London Adult Critical Care Network ensured that all hospitals across the sector retained situational awareness. Due to significant resource constraints the interaction with renal medicine was crucial; we scheduled a specific daily meeting to plan which patients would receive specific renal replacement modalities during the next 24 hour period.
Discussion – Leadership and management in a crisis situation
Before considering crisis leadership, it is important to examine what constitutes a crisis. Crises in the broadest sense are critical junctures in the life of systems, when their ability to function can no longer be relied upon. 2 This differs from a more routine ‘challenge’ or ‘problem’ where the system is trying to be improved or protected from a threat that would not threaten its very existence. Crises can be defined in relation to their speed, as either exploding or unfolding. 3 The COVID-19 pandemic fell into the latter category and was a more complex and varied crisis than any of the authors have confronted heretofore.
The National Health Service in common with other healthcare systems is an organisation more used to medium to long term planning rather than rapidly adapting to a dynamic situation. When there is a requirement to quickly adopt a different command and control structure in the face of a major incident or mass casualty situation the approach taken is commonly based on the Major Incident Medical Management and Support (MIMMS) structure first described by Tim Hodgetts and colleagues in 1994. 4 This publication and training course laid out three tiers of command and control; Gold or Strategic which provides broad support for operational commanders, Silver or Tactical which controls and co-ordinates activity at the incident site and Bronze or Operational with a focus on triage and direct patient care. The MIMMS framework is designed for relatively short duration medical incidents and is deliberately focussed on traumatic injury and mass casualty situations, essentially an exploding as opposed to an unfolding crisis. Arguably the MIMMS format is not optimised for a prolonged or unfolding medical crisis that involves protracted workforce planning and logistic considerations.
Military organisations should be adept at handling rapidly evolving crises, which in many respects represent their reason d’etre. Military leadership can be described as the projection of personality and character to get subordinates to do what is required of them and to engender within them the confidence that breeds initiative and the acceptance of risk and responsibility. Effective military command is achieved by decisive action; clear direction and guidance; precept and example; advice, encouragement and where necessary admonishment; and by giving subordinates every opportunity to contribute to mission success through appropriate delegation of authority. Management, probably best defined succinctly as the effective utilisation of available resources, both human and logistic, is not a substitute for leadership, but is a key element of command.
Military leadership and management is designed to mitigate the impacts of an environment where ‘crises’ or ‘emergencies’ are a regular part of daily operations. A culture is developed to ensure effective command leads to rapid enactment of a plan or set of actions. It is tempting to apply the principles of military leadership to civilian healthcare, particularly in times of crises, such as during the recent pandemic. However there are a number of challenges to this application, most notably the differing culture between the two organisations. Within healthcare a more questioning and debating style to team management is the norm and usually results in a collaborative environment where all team members feel enabled and empowered. However, such an approach, with the requirement for quorate decision making has the potential downside of producing relatively slow responses in a time of rapid change. There is also commonly a greater plurality between differing professions within civilian healthcare settings, with the potential for silo working that the more hierarchical military command structures mitigates to some extent. The final difference is the relative higher degree of autonomy that senior civilian clinicians and nurses have, or at least are perceived to have, with the consequent potential for a horizontal as opposed to a hierarchical command and control structure. Whilst having many advantages during a non-crisis working pattern this is another factor that potentially leads to slower response and decision making during a crisis.
Crisis leadership within healthcare has a limited literature base. Rubin described collaborative leadership as building - or helping to ensure the success of - a heterogeneous team to accomplish a shared purpose 5 which effectively describes the aims of the Tactical Team and Hub. Utilising leaders throughout a healthcare organisation, leading within their area of expertise should produce a more flexible and nimbler organisation. A group in Toronto, described an approach of collective or collaborative leadership being effective in response to the SARS outbreak. 6 They describe a ‘hub and spoke’ model where leaders took responsibility for one of a number of multiple important domains within a critical care service such as infection control, man power, communication, system thinking and lobby groups. Each had a multi-disciplinary team within which they worked. They highlighted the danger of the ‘silo’ nature of teams in many healthcare environments at a time of crisis. The breaking down of traditional ‘siloed’ teams within healthcare is frequently cited as method of tackling large scale crises. Simple, structured clinical or organisational problems are amenable to independent teams performing specialised tasks. However, when the problem facing an organisation becomes more unstructured or unpredictable then co-coordinative leadership is required and the unseen boundaries between different teams must be broken down. 7
The importance of a ‘command’ group has been highlighted in many other healthcare organisations where a rapid change and reconfiguration of services has been required.8–10 Although collaborative leadership principles form an important part of crisis leadership, there remains a requirement for oversight of the situation, particularly in the management of personnel and resources. As we found during the COVID-19 pandemic, the number of staff available can vary rapidly, due to illness, social lockdown measures and increased levels of staff volunteering for extra work. Ensuring a safe, balanced workforce requires oversight by a single leadership group. Resource allocation similarly requires management across a whole organisation. Supply chains can be affected during crises, something that was particularly apparent during the COVID-19 pandemic with fluctuating supplies of personal protective equipment and other consumables. Communication during crises must be clear, simple and accurate and benefits from central management. During the COVID-19 crisis NHS England recommended that critical care departments utilise a ‘strategic team’ responsible for coordinating the whole department. 11
Looking back at the first wave of the COVID-19 pandemic through the prism of a second, surge in cases allows some reflection on the actions undertaken at our institution. We strongly believe that the system we instituted allowed continuation of a high level of clinical care to all of our patients during a time of unprecedented demand. However, such a system necessarily relies on the effective replacement of normal clinical management structures and brings with it a partial loss of collective decision making processes. The system described in the present paper also works well when dealing with a single coherent clinical problem, less so when having to incorporate the needs and views of other clinical providers and patient groups. In summary it is probably an effective tool for dealing with a system at risk of being overwhelmed, but it’s utility, at least within the National Health Service is limited to times of existential crisis.
One area that we felt was crucial to managing the service, but that we failed to realise fully, was the effective use of data. The tactical team spent much of the time, collecting, transmitting and managing data. At the outset we identified this as a key area and initially planned for a dedicated team member to work with the tactical consultant who would capture hour by hour clinical data to enable more effective decision making. Examples of such data, were patients requiring renal replacement therapy, prone position ventilation or those with more complex ventilatory requirements. Our existing clinical information system was able, to some extent, to identify this data, but producing it on a daily basis was a very time consuming process. Having a real time dashboard that identified this data more readily would be invaluable.
Conclusion
The diverse and complex clinical situation that evolved at King’s College Hospital during the COVID-19 pandemic required an agile and dynamic command and control system with effective communication mechanisms. Although there is no one correct structure, the arrangements outlined in this account provided an environment in which every patient admitted to our centre received efficacious and compassionate critical care. Utilising some of the principles of military command and control allowed Kings Critical Care to co-ordinate a pandemic response in which critical care was central to the whole Trust’s efforts. It complimented the existing pan-Trust major incident structures and allowed ongoing and sustainable day to day management and leadership. This structure could be used in the management of future prolonged crises and major incidents within healthcare settings.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.