
Abstract
During the Coronavirus Disease 2019 (COVID-19) pandemic institutions have needed to develop pragmatic clinical pathways to balance the excess critical care demand and local resources. In this single-centre retrospective cohort study we describe the outcomes of COVID-19 patients admitted to Guy’s and St. Thomas’ NHS Foundation Trust (GSTT) critical care service. Patients were managed according to a local respiratory failure management pathway that was predicated on timely invasive ventilation when indicated and tailored ventilatory strategies according to pulmonary mechanics. Between 2 March and 25 May 2020 GSTT critical care service admitted 316 patients with confirmed COVID-19. Of the 201 patients admitted directly through the Emergency Department (ED) with a completed critical care outcome, 71.1% survived to critical care discharge. These favourable outcomes may serve to inform the wider debate on optimal organ support in COVID-19.
Introduction
The rapidly evolving understanding of Coronavirus Disease 2019 (COVID-19) respiratory failure pathogenesis, limited disease-specific evidence and demand-resource imbalances have posed significant challenges for intensive care clinicians. These uncertainties have engendered a debate on optimal organ support strategies and highlighted the need for more data to help design clinical trials. However, in the interim period, institutions have needed to develop pragmatic clinical pathways to balance the excess critical care demand and available local resources.
The objective of this study was to evaluate the outcomes of critically ill COVID-19 patients managed in the initial phase of the pandemic at a high-volume Severe Respiratory Failure (SRF) and Extracorporeal Membrane Oxygenation (ECMO) centre in the United Kingdom (UK).
Methods
Guy’s and St. Thomas’ NHS Foundation Trust (GSTT) is both a nationally-commissioned SRF and airborne High Consequence Infectious Disease (HCID) centre. In response to the pandemic, the critical care capacity at GSTT was increased to 187 beds capable of invasive ventilatory support and a respiratory failure management pathway for COVID-19 was developed (Figure 1).
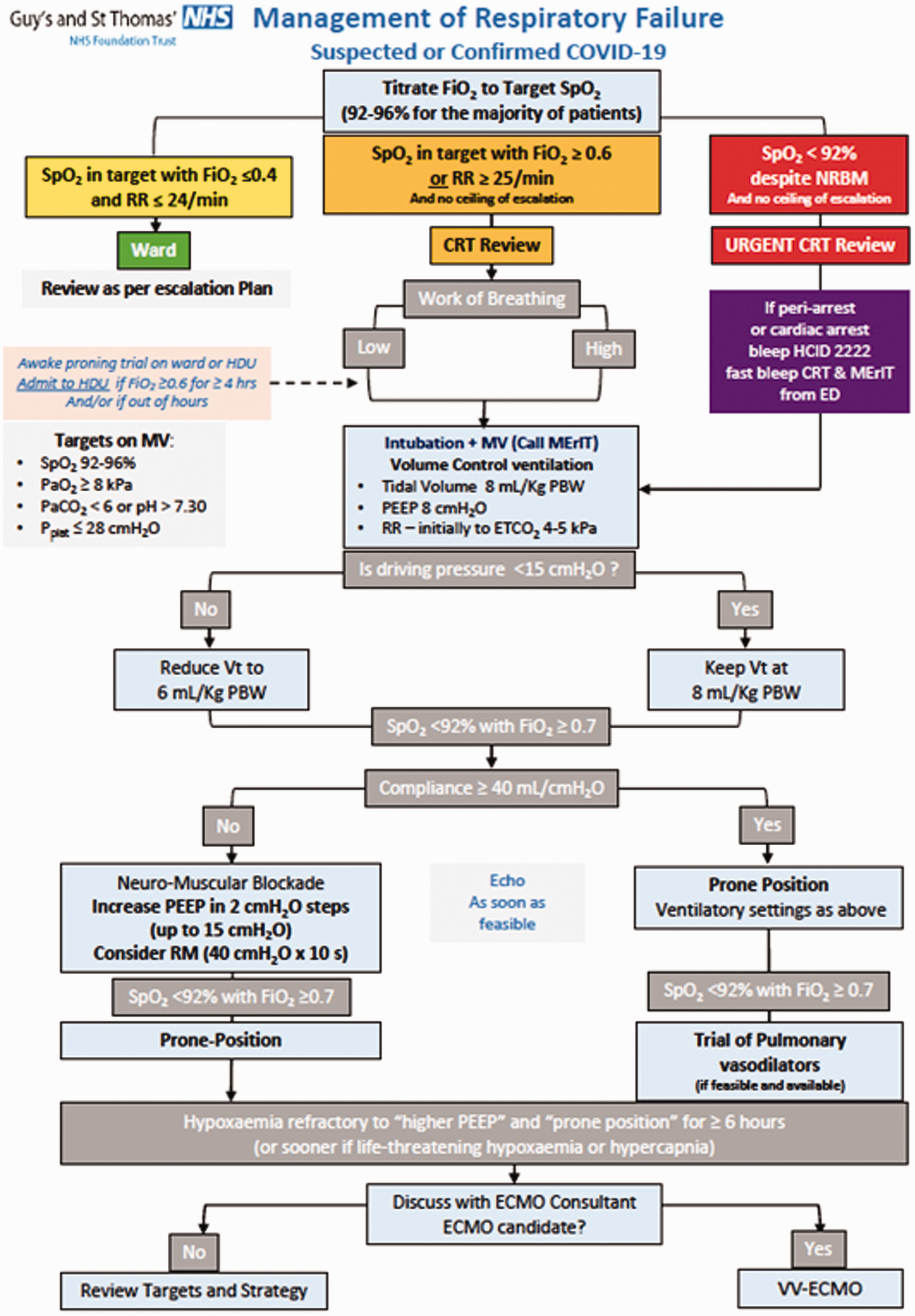
Guy’s and St. Thomas’ NHS Foundation Trust suggested management of respiratory failure in Coronavirus Disease 2019 (COVID-19).
This was a retrospective single-centre cohort study of all confirmed COVID-19 cases admitted to the critical care service at GSTT from 2 March to 25 May 2020. Our primary outcome was critical care mortality in patients admitted directly to GSTT.
Results
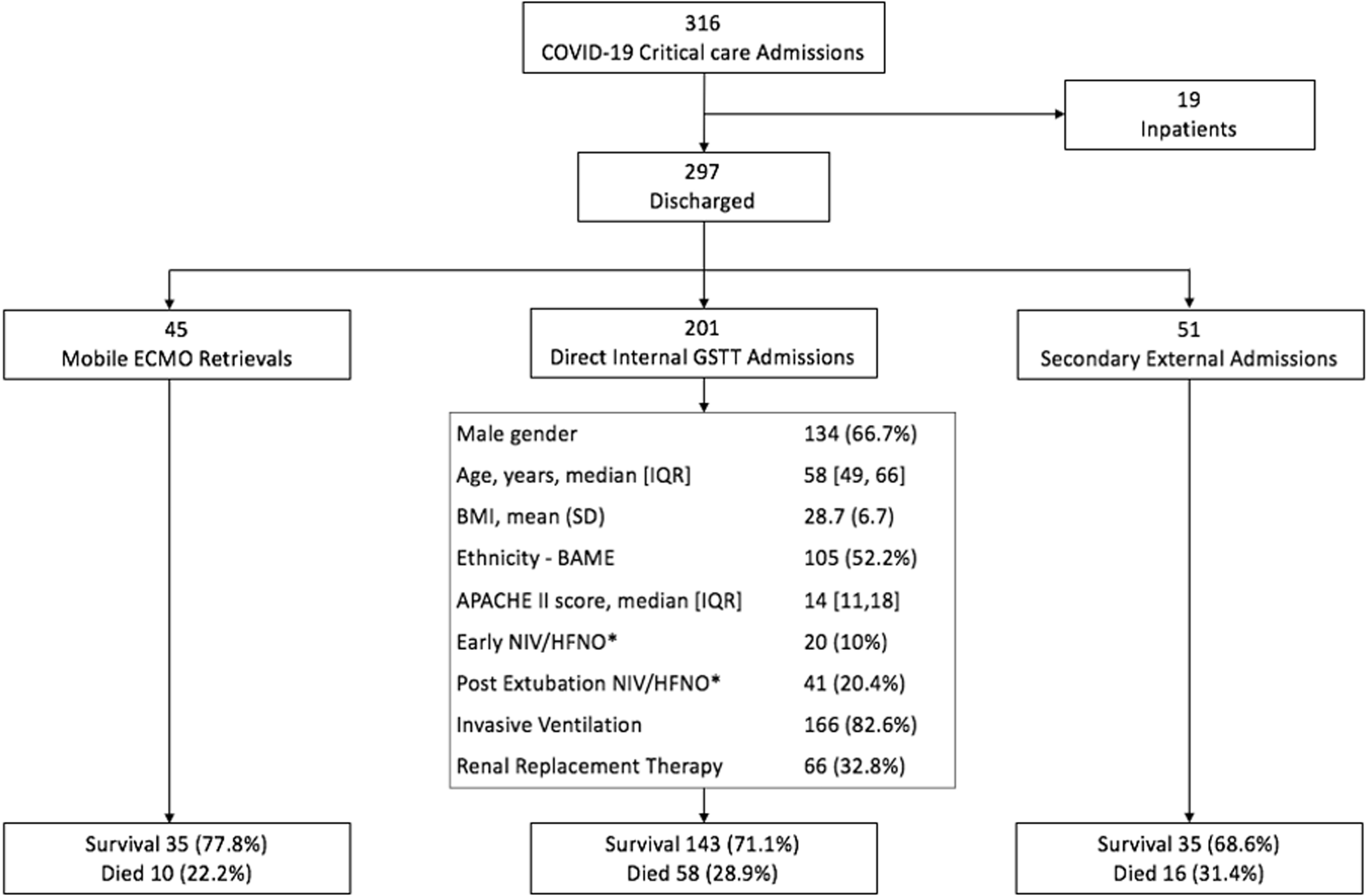
During the study period, the critical care service admitted 316 confirmed COVID-19 patients, including 52 mobile ECMO retrievals and 51 non-ECMO critical care transfers from other institutions (Table 1).
Strobe flowchart of the 316 patients admitted to Guy’s and St. Thomas’ NHS Foundation Trust (GSTT) Critical Care with confirmed Coronavirus Disease 2019 (COVID-19).
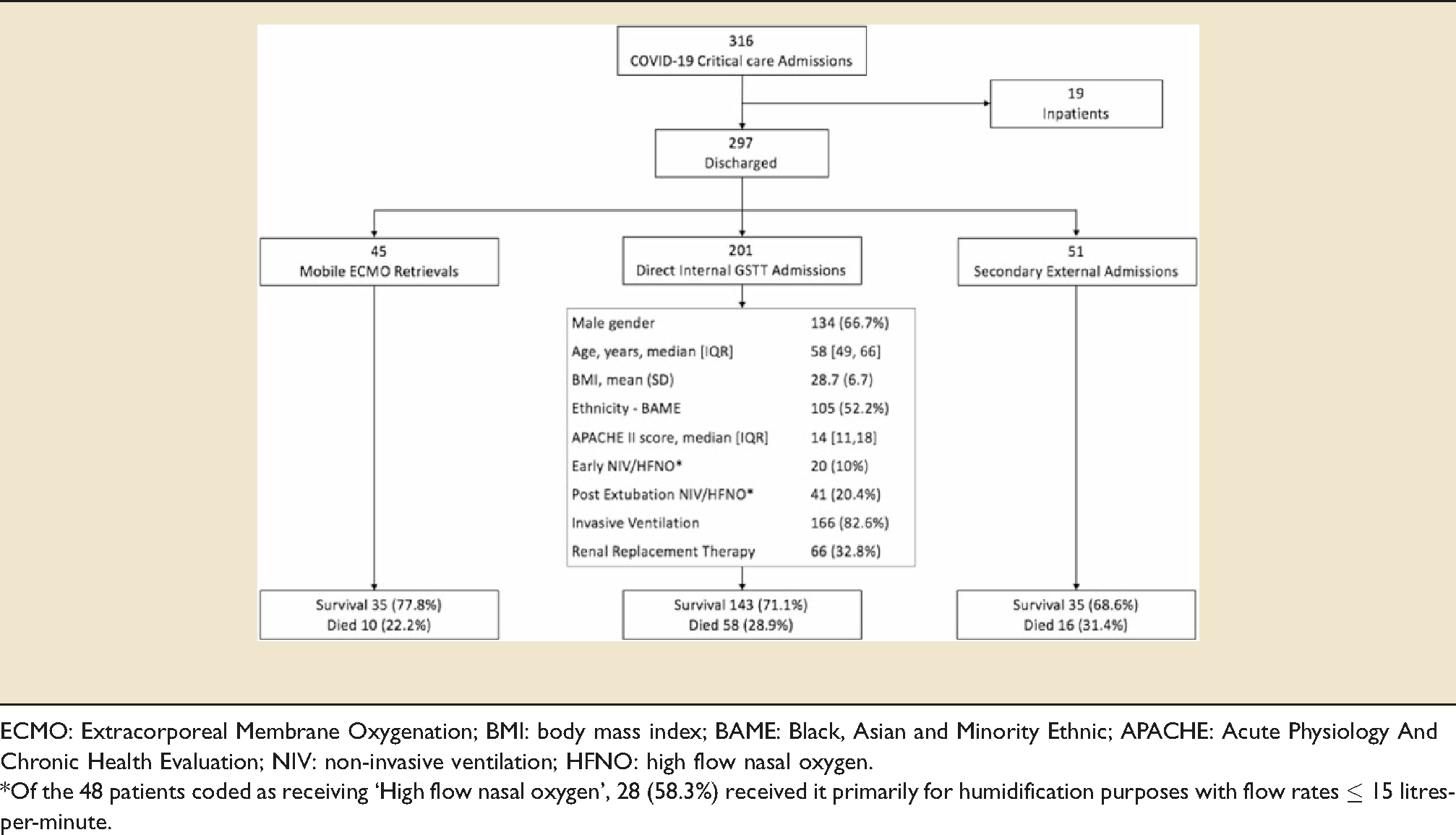
ECMO: Extracorporeal Membrane Oxygenation; BMI: body mass index; BAME: Black, Asian and Minority Ethnic; APACHE: Acute Physiology And Chronic Health Evaluation; NIV: non-invasive ventilation; HFNO: high flow nasal oxygen.
*Of the 48 patients coded as receiving ‘High flow nasal oxygen’, 28 (58.3%) received it primarily for humidification purposes with flow rates ≤ 15 litres-per-minute.
A total of 213 COVID-19 patients were admitted directly to our critical care service through our Emergency Department, 201 patients had a completed critical care discharge outcome and 13 were still being supported. The median [IQR] age of patients was 58 [49,66] years, 66.7% were men, 52.2% were from Black, Asian and Minority Ethnic (BAME) groups, and the median [IQR] Acute Physiology And Chronic Health Evaluation (APACHE) II score was 14 [11,18]. 166 (82.6%) patients required invasive ventilation and 61 (30.3%) non-invasive respiratory support. Of the 61 patients who received non-invasive support, 41 (67.2%) received it only following extubation. Of the 48 patients coded as receiving ‘High flow nasal oxygen’, 28 (58.3%) received it primarily for humidification purposes with flow rates ≤15 litres-per-minute. Only one patient originally admitted to GSTT required ECMO initiation due to a concurrent massive pulmonary embolism. The critical care mortality in patients admitted directly to GSTT was 28.9%.
Discussion
This is one of the largest single-centre studies describing outcomes of critically ill COVID-19 patients. Despite a significant surge of critically ill COVID-19 patients, the survival to discharge of 71.1% provides reassurance that a strategy predicated on timely invasive ventilation and meticulous organ support 1 in a high-volume SRF centre can confer favourable outcomes. When comparing to the contemporaneous Intensive Care National Audit and Research Centre (ICNARC) report of 9,026 COVID-19 patients admitted to critical care in the UK, our cohort had comparable baseline characteristics (age, sex, BMI and APACHE II scores) but with higher rates of advanced respiratory support (82.6% versus 72.5%), lower use of basic respiratory support (30.3% versus 63.3%) and a lower mortality (28.9% versus 44.3%). 2
COVID-19 is an inflammatory vasculopathy that is initially associated with minimal parenchymal oedema and atelectasis but significant pulmonary shunt, dead space and hypoxemia. 3 As lung oedema increases, use of non-invasive ventilation (NIV) may improve oxygenation, however, unless the work of breathing and lung shear stress are reduced, there are concerns that prolonged NIV can mask ongoing patient self-inflicted lung injury (P-SILI). 4 This may partially explain the significant mortality difference observed between our cohort and national data, and is congruent with prior evidence suggesting high failure rates and excess mortality in patients receiving NIV in moderate-to-severe acute hypoxaemic respiratory failure.5,6
This study has a number of limitations. With a single-centre retrospective study it is difficult to adjust for unmeasured confounders, including variability in resources, adjunctive management strategies and thresholds for critical care admission. When comparing local data to the national ICNARC data, the authors accept that confounding by indication influences any inference.
Despite these limitations, the management and associated outcomes reported may serve to inform the wider debate on optimal organ support strategies in future surges of COVID-19.
Footnotes
Ethical approval
The study had institutional approval (institutional research governance reference number: 10796) and qualified as a service evaluation as defined by the UK NHS Health Research Authority and therefore did not require review by the Research Ethics Committee (![]() ) and had waiver of individual informed consent, when used without breach of privacy or anonymity.
) and had waiver of individual informed consent, when used without breach of privacy or anonymity.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Shankar-Hari is supported by National Institute for Health Research Clinician Scientist Award CS-2016-16-011. The views expressed in this publication are those of the authors and not necessarily those of the National Health Service, the National Institute for Health Research, or the Department of Health and Social Care.