
Abstract
Introduction
The average age of the surgical patient in the UK is increasing. Frailty and cognitive impairment have been shown to be important risk factors in elderly patients with surgical pathology. Limited work has previously assessed the outcomes of acute pancreatitis in the elderly population and the usefulness of current severity scoring methods. We aimed to assess the mortality rates in this cohort and identify any factors that may influence patient outcome.
Methods
All patients ≥ 80 years admitted with acute pancreatitis between 1 January 2014 and 31 May 2018 were retrospectively identified. Disease severity scores were measured by a modified Ranson score, and patients' co-morbidities were quantified with the Charlson Comorbidity Index. Primary endpoint was whether the patient was alive at discharge; multilevel logistic regression was used to identify any independent risk factors for patient outcomes.
Results
Eighty-seven patients were included, with an average age of 86 years. The most common aetiology was gallstones. Nine patients died during admission, and ITU admission was the only predictor of mortality (p = 0.027). Twenty-three patients had died by one year. Endoscopic retrograde cholangiopancreatography was more common in patients with gallstone disease who were alive at one year (p = 0.029).
Discussion
Risk severity and co-morbidity scores are not predictive of outcomes in elderly patients with acute pancreatitis. The use of endoscopic retrograde cholangiopancreatography should be considered in elderly patients with acute gallstone pancreatitis where suitable. Further work is needed to identify improved mortality prediction tools in the elderly with acute pancreatitis and optimal management strategies.
Introduction
The average age of the surgical patient in the United Kingdom (UK) is increasing. 1 Surgical teams are having to rapidly adapt to meet this aging demographic, with risk predictive models being trialled in an attempt to tailor management specifically to this elderly cohort. Indeed, frailty scores and cognitive impairment have already been identified as important factors in determining older surgical patients' outcomes.2,3
Incidence of acute pancreatitis has been rising globally in recent decades, 4 and patients presenting to hospital with the condition will often require admission. Whilst commonly treated conservatively, the condition can cause systemic complications that necessitate higher levels of monitoring and organ support. 5 As such, several clinical scoring systems for acute pancreatitis are available, in an attempt to stratify which patients may need such intervention. 6
Unfortunately, little work has previously assessed the outcomes of acute pancreatitis in an older population, and specifically the usefulness of severity scores. The most common cause in the UK of acute pancreatitis in the elderly is biliary disease 7 ; however, historic data have demonstrated a sizeable number who present in an atypical manner. 8 More work is needed to better understand the nuanced management required for this patient group.
As such, our study aimed to determine the overall mortality rate in an elderly patient cohort presenting with acute pancreatitis and to identify any discernible factors that may influence patient outcomes.
Methods
Data collection
A retrospective observational study was conducted across two separate district general hospitals based in the UK, with all data collected through electronic patient records. The hospitals involved have a combined capacity of over 1000 beds, with sizeable surgical departments, covering both emergency and elective practice. The study was registered as an audit and was also approved by the local Caldecott Guardian.
Patients aged 80 years or over who were admitted with acute pancreatitis between 1 January 2014 and 31 May 2018 were identified through hospital coding. Inclusion into the study was then confirmed through the presence ≥2 factors of (1) abdominal pain (2) serum amylase value ≥ 300 iU/L (3) computerised tomography (CT) scan features suggestive of acute pancreatitis. Those with a previous diagnosis of chronic pancreatitis were excluded.
Patient data were collected from admission to a one-year follow-up. Admission data collected included age, gender, Charlson co-morbidity score, and any identified underlying cause. Due to the retrospective nature of the study, only a Ranson score could be calculated; the biochemistry laboratories provided alanine transaminase (ALT) values, as opposed to aspartate transaminase (AST) values required for the conventional score; therefore, a modified Ranson was employed (see Appendix 1).
Follow-up data collected included mortality at discharge, patient length of stay, any intensive care unit (ITU) admission, unplanned readmission within 30 days (for any reason), and mortality at one year. Any magnetic resonance cholangiopancreatography (MRCP) performed, any endoscopic retrograde cholangiopancreatography (ERCP) or cholecystectomy performed, or any pseudocyst formation or pancreatic necrosis identified were also included.
Statistical analysis
All data were presented as median (interquartile range) where appropriate. Chi-squared testing was used for categorical data comparisons, and Mann-Whitney testing was used for continuous data comparisons.
Independent risk factors were assessed via multilevel logistic regression; use of the multilevel model accounted for both individual patient-level risk (at level 1) and centre-level random effects (at level 2). Plausible variables were identified for use in the analysis by our group prior to the analysis. Only patients with complete data were included in the regression analysis.
All statistical analyses were performed using the R 3.5.3 software package (R Foundation for Statistical Computing, Vienna, Austria), using the tidyverse, ggplot2, dplyr, and finalfit packages. A p value < 0.05 was deemed statistically significant.
Results
Patient demographics
Summary of patient admission demographics.
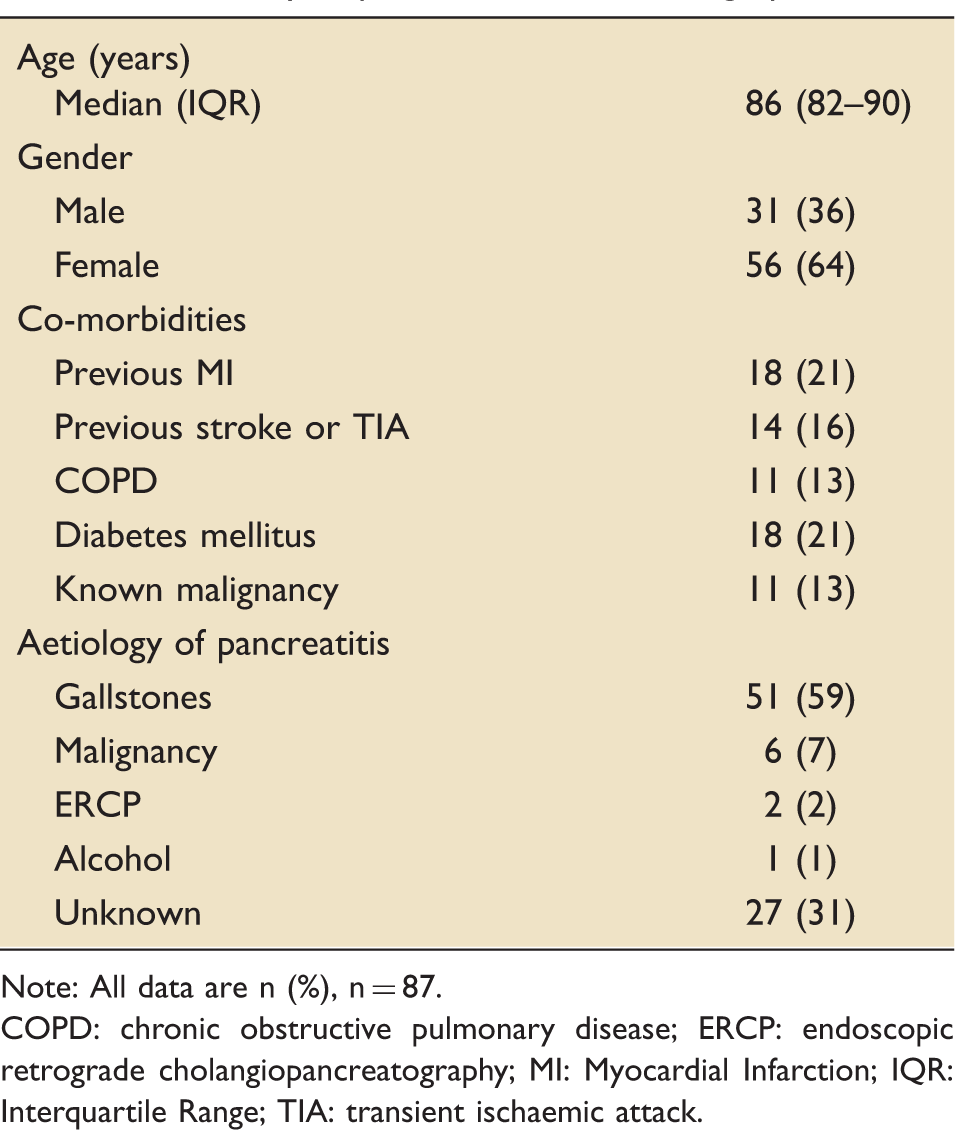
Note: All data are n (%), n = 87.
COPD: chronic obstructive pulmonary disease; ERCP: endoscopic retrograde cholangiopancreatography; MI: Myocardial Infarction; IQR: Interquartile Range; TIA: transient ischaemic attack.
Patient outcomes during admission
Nine patients (10%) died during their admission. The median length of stay was six days (IQR 4–12 days), with seven patients (8%) being admitted to ITU. Two patients developed pseudocysts, whilst no patients developed pancreatic necrosis.
Multilevel logistic regression for patient outcome at discharge, n = 60, data shown as either n (%) or odds ratio (confidence intervals).
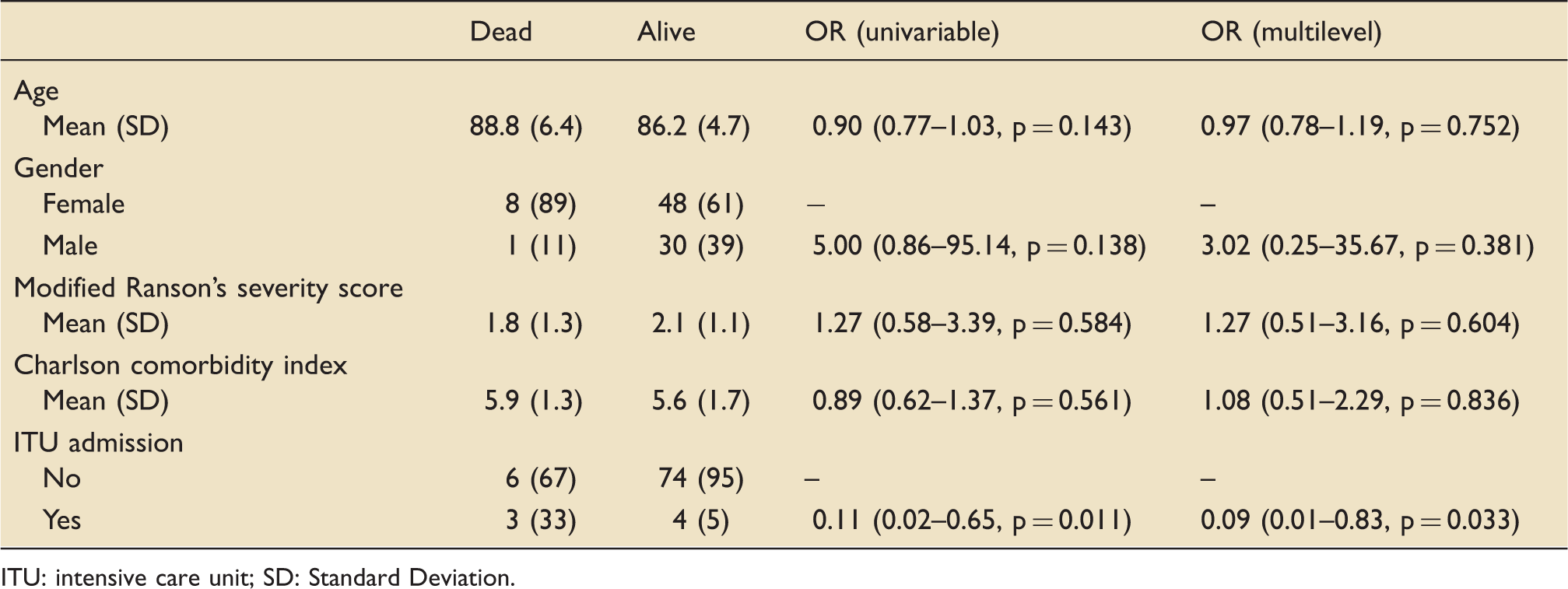
ITU: intensive care unit; SD: Standard Deviation.
For the patients who were admitted to an ITU setting, equivocal Ranson scores (2 vs. 2 respectively, p = 0.824) and co-morbidity scores (5 vs. 6 respectively, p = 0.982) were observed, compared to those that received purely ward-based care.
Secondary outcomes
For those alive at 30 days, a further 14 patients (18%) died at one-year follow-up and 12 patients (15%) had an unplanned readmission. 39 patients (50%) had an MRCP performed and 22 patients (28%) underwent an ERCP. No variables were identified as independent predictors of one-year mortality from multilevel analysis.
Outcomes variables at one year in patients with gallstone disease, n = 51, data shown as n (%).

ERCP: endoscopic retrograde cholangiopancreatography; SD: Standard Deviation.
Discussion
With an aging population, optimising the management of older patients presenting with surgical pathologies is a growing priority. Acute pancreatitis proves no exception to this mantra, as we demonstrated a mortality rate of 10% in this patient cohort, significantly above nationally reported rates of 5%. 9 Importantly, neither the co-morbidity score nor risk severity score assessed proved predictive of patient outcomes. As such, we suggest that urgent work is needed to develop improved models in risk stratifying and optimising patient management in the elderly cohort presenting with acute pancreatitis.
This is not the first time that such concepts for this disease have been suggested. A small study by Somasekar et al. showed not only similar high mortality rates in the elderly presenting with acute pancreatitis, but that the Glasgow scoring system is also of limited predictive value. 10 Indeed, notions of developing unique risk scores for older patients are already growing for other surgical conditions; the recent Emergency Laparotomy and Frailty (ELF) study conducted in the UK demonstrated frailty itself as an independent risk factor of post-operative outcomes in elderly patients undergoing emergency laparotomy, advising such a scoring system should be integrated into acute surgical assessment practice. 2
Acute pancreatitis has long been known to cause a significant physiological insult to the body. Whilst the majority of cases are mild and can be managed conservatively, moderate to severe cases can lead to significant systemic involvement and multi-organ failure, requiring higher levels of care. Elderly patients often have multiple co-morbidities and limited cardiovascular reserve; thus, even mild cases of acute pancreatitis can lead to significant morbidity in this group.11,12 This is reflected in our data, with the average length of stay and one-year mortality rates at six days (IQR 4–12 days) and 26%, respectively. In our dataset, those who were admitted to ITU had a higher mortality rate than those who received purely ward-based care; whilst we identified no difference in their disease severity scores or patient co-morbidity states, there will be several unmeasured cofounders and modifiers not accounted for by the retrospective observational nature of the study, limiting any additional conclusions that can be made from this.
Intervention can play an important role in the management of patients with acute pancreatitis when there is a known treatable cause. In the elderly cohort specifically, ERCP has previously been shown to have a high degree of success with low rates of complications, across a range of biliary pathologies. 13 We were able to demonstrate that ERCP is both feasible in octogenarians following acute gallstone pancreatitis, being performed on average six weeks after the initial admission, and an association with ERCP and overall survival at one year. This is by no means causative, as those who are well enough to tolerate such a procedure are naturally more likely to have better outcomes; however, we do advocate that early ERCP in elderly patients with acute gallstone pancreatitis should be considered in those deemed suitable. Conversely, biliary surgery in the elderly is already known to be high risk, 14 and with only a small number of patients included in our study undergoing a laparoscopic cholecystectomy, we are unable to comment further regarding its potential impact.
We appreciate the limitations from the retrospective nature of the study, restricting the conclusions drawn; however, these data should help push towards further prospective studies to develop tailored risk severity scores and optimal management for elderly patients with acute pancreatitis. NHS England defines the term “elderly” as an individual aged 65 years or more 15 ; however, as previous research in this area has focused solely on patients aged 80 years or more, 10 we opted for a similar cohort to maintain consistency in this area of research. Use of a modified prediction score may limit its validation; however, this was employed to ensure maximal data completeness. Whilst we have only collected data on a relatively small number of patients, increasing the risk of type II error, our work is strengthened by the multicentre methodology employed.
Conclusion
Mortality rates in elderly patients presenting with acute pancreatitis are high, and improved models are needed to help stratify risk, potentially with the incorporation of frailty assessments on admission. ERCP is known to be safe in elderly patients following acute pancreatitis episodes and should always be considered in elderly patients with acute gallstone pancreatitis where suitable.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support for the research, authorship, and/or publication of this article: MB is funded by the National Institute for Health Research. The views expressed in this publication are those of the author(s) and not necessarily those of the funding bodies.