
Abstract
Introduction
The variability of acute respiratory distress syndrome management may affect the referral practice to severe respiratory failure centres. We described the management of acute respiratory distress syndrome in our catchment area.
Methods
An electronic survey was administered to 42 intensive care units in South-East England.
Results
Response rate was 71.4%. High-flow nasal oxygen and non-invasive ventilation were used ‘often’ in moderate-acute respiratory distress syndrome by 46.7% and 60%. During invasive ventilation, 90% preferred pressure control, targeting tidal volumes of 6–8 ml/kg (53.3%) or 4–6 ml/kg (46.7%). Positive end-expiratory pressure was selected by positive end-expiratory pressure/inspiratory fraction of oxygen tables (50%) or decremental positive end-expiratory pressure trials (20%). Neuro-muscular blockers were widely used, although routinely by only 3.3%. High-frequency oscillatory ventilation (10%) and inhaled nitric oxide (13.3%) were rarely used. None used oesophageal manometry. Recruitment manoeuvres were used ‘often’ by 26.7%. Equipment (90%) and protocols (80%) for prone position were common, with sessions mostly lasting 12–18 h.
Conclusions
Although variable, practice well reflected the available evidence. Proning was widely practiced with good availability of educational resources and protocolised care.
Keywords
Introduction
Acute respiratory distress syndrome (ARDS) is a prevalent condition characterised by hypoxaemic respiratory failure and associated with a mortality up to 46.1%. 1 The management of patients with ARDS is often challenging and requires supportive interventions of increasing intensity and complexity based on the severity of the syndrome. 2
Despite the publication of several national 3 and international guidance documents, 4 the implementation of recommended supportive and therapeutic measures varies across different centres. 5 An international survey observed that proven lung protective strategies including prone position (PP) are underused. 1 The implementation of advanced therapeutic and supportive measures such as PP may be limited by local knowledge and expertise, lack of education or under-recognition of their indication.6,7
The management of severe acute hypoxaemic respiratory failure (SRF) including extracorporeal membrane oxygenation (ECMO) in England is coordinated by a national specialised committee via a hub and spoke system. Each SRF centre in England functions as a referral centre for a segment of the population with multiple peripheral referring centres. Guy’s and St Thomas’ NHS Foundation Trust (GSTT) is a commissioned SRF centre in London which supports 42 centres in South East England. We receive an average of 300–370 ECMO referrals/year, and our annual ECMO runs number around 100–110 cases. The total activity, seasonal variation, patient severity and proportion of patients referred to patients retrieved are also dependent on the capabilities, expertise and practices of referring critical care units.
The aim of this study was to describe the practice and capabilities in the management of SRF by the hospitals in the South East of England.
Methods
We conducted a cross-sectional regional survey using an electronic questionnaire emailed to 42 intensive care units (ICUs) in the South-East of England. An invitation to participate in this study was sent to the local contact of the 42 centres. Email addresses were retrieved from our contact database and from the authors’ personal contacts. Participants were initially contacted by email. The email included a cover letter explaining the purpose of the survey and a link to the web-based survey. Two follow-up reminders were sent in the month following the initial email. Participation was voluntary and no incentives were provided for responding to the survey.
Development and administration of the online questionnaire
Using an iterative process, the survey questionnaire was developed by three authors (LC, AJ and BS). This was followed by internal pilot testing amongst clinicians at our institution. The pilot was followed by further retesting to refine and finalize question stems, response formats, and to assess face validity and clarity.8,9 The survey was self-administered using a Google Form. 10
The survey consisted of 50 questions arranged in three broad domains, organised as follows.
In the first domain, participants answered questions about ICU staffing and caseload: structured responses were provided to questions regarding the number of hospital and ICU beds, case-mix, caseload, nursing and physician ratios.
The second domain explored the availability of Respiratory therapies and their use. Various sections examined in detail, the centre’s availability, capabilities and utilisation of different respiratory therapies, i.e., high-flow oxygen, continuous positive airway pressure (CPAP), non-invasive ventilation (NIV) and prone position (PP). Structured responses were sought in the form of yes or no and four-/five-point Likert scale. The responses on Likert scale were percentages in the order of increasing frequency defined as – never (0%), rarely (1%–20%), sometimes (21%–50%), often (51%–99%) and always (100%).
The survey also examined in greater detail the departmental practice of PP in the referring centres. This was of interest to us, as application of and response to PP provided crucial information to the decision-making process surrounding initiation of ECMO. Patients failing to respond to appropriately applied PP after optimisation of ventilation, neuromuscular blockade (NMB) and fluid management who otherwise met the criteria were more likely to benefit from veno-venous-ECMO. Respondents were also asked about the availability of trans-thoracic echocardiography out of hours in their ICUs.
In the third domain, participants responded on the implementation of lung-protective ventilation and the use of adjunctive therapies like NMB and recruitment manoeuvres (RMs). Information was sought around the preferred NMB, dosing regimen and monitoring during NMB. Respondents were also probed on the likelihood of performing a RM and the preferred method of doing so.
Survey respondents
The response rate was 71.4% (30/42 centres). More than 90% of respondents (n = 27) were consultant grade, 1 (3.3%) staff grade physician and 2 (6.7%) senior nurses (Band 7 and above).
Analysis of data
Descriptive analyses and frequencies were calculated for demographic and qualitative data.
Results
Centres’ background, case-volume and experience
Most of the ICUs were mixed medical-surgical (83.3%), while 10% were exclusively medical. Moreover, 11.1% had no high-dependency unit (HDU) beds, 44.4% had between 1 and 5 HDU beds, 25.9% between 6 and 10 HDU beds and 18.6% > 10 HDU beds. In addition, 89.9% of the units were able to offer 1:1 patient to nurse ratio in the ICU.
Of the 365 patients referred to GSTT over the previous calendar year, 55.2% of the centres referred 0–5 patients; 27.5% referred 6–10 patients, while 17.2% referred > 10 patients.
Ventilation capabilities
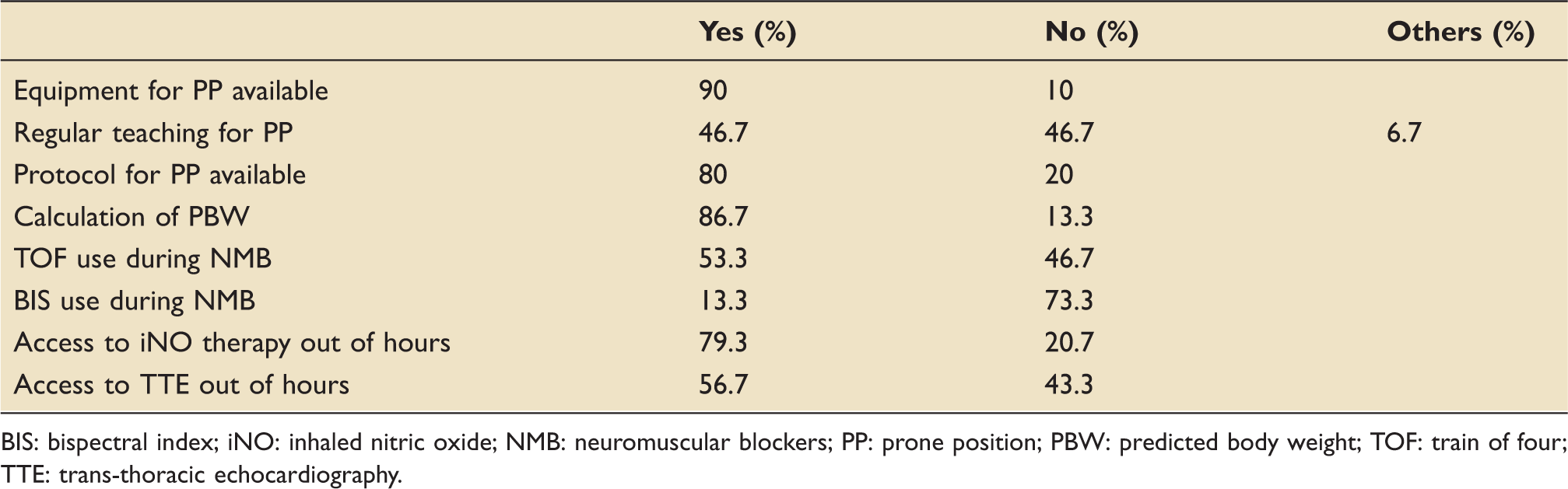
Findings were summarised in Table 1 and Figure 1.
Practices in the management of ARDS within intensive care units in South East England. BIS: bispectral index; iNO: inhaled nitric oxide; NMB: neuromuscular blockers; PBW: predicted body weight; PP: prone position; TOF: train of four; TTE: trans-thoracic echocardiography. Practices in the management of ARDS within intensive care units in the South East of England. BIS: bispectral index; iNO: inhaled nitric oxide; NMB: neuromuscular blockers; PP: prone position; PBW: predicted body weight; TOF: train of four; TTE: trans-thoracic echocardiography.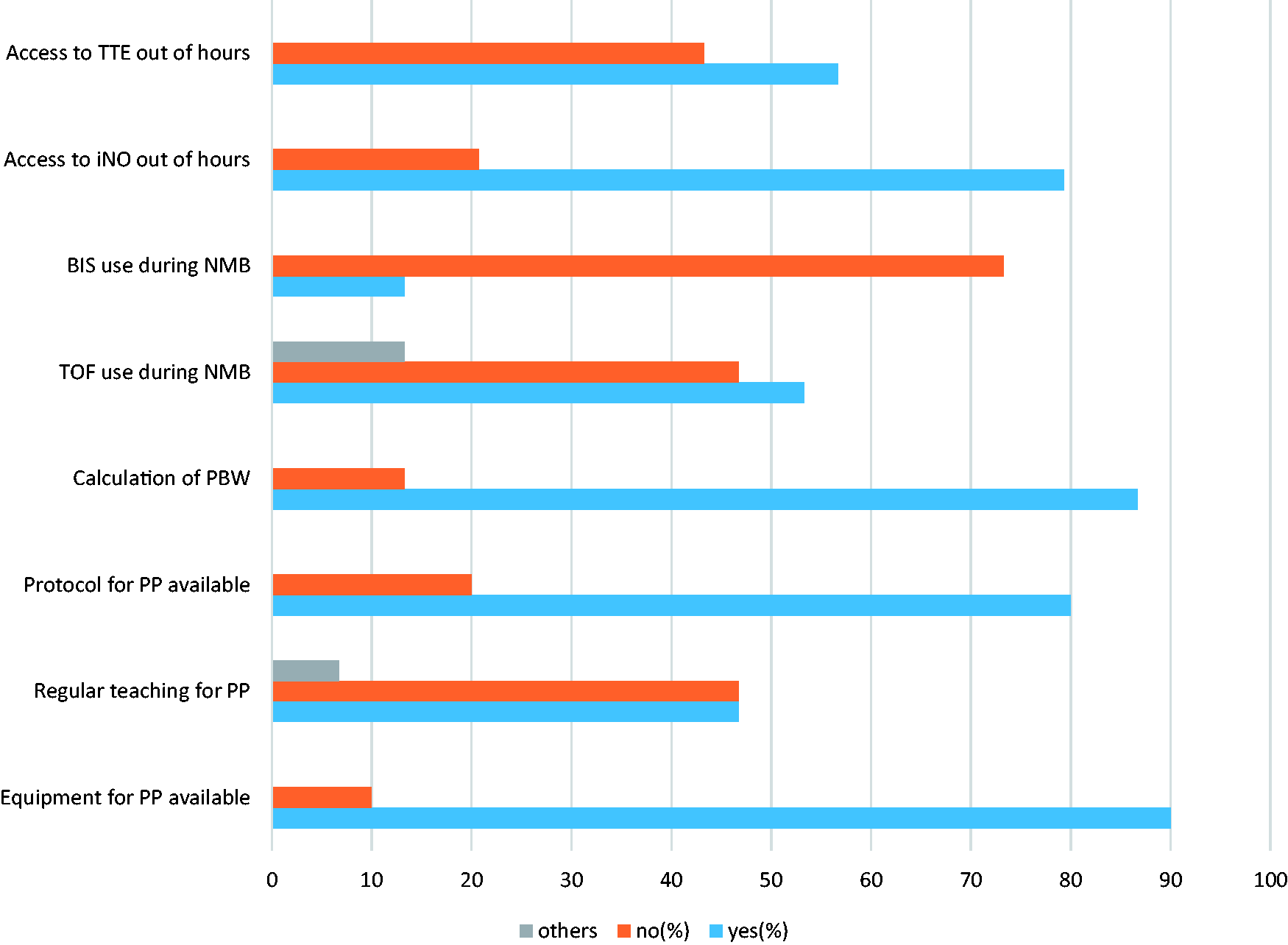
High-flow nasal oxygen
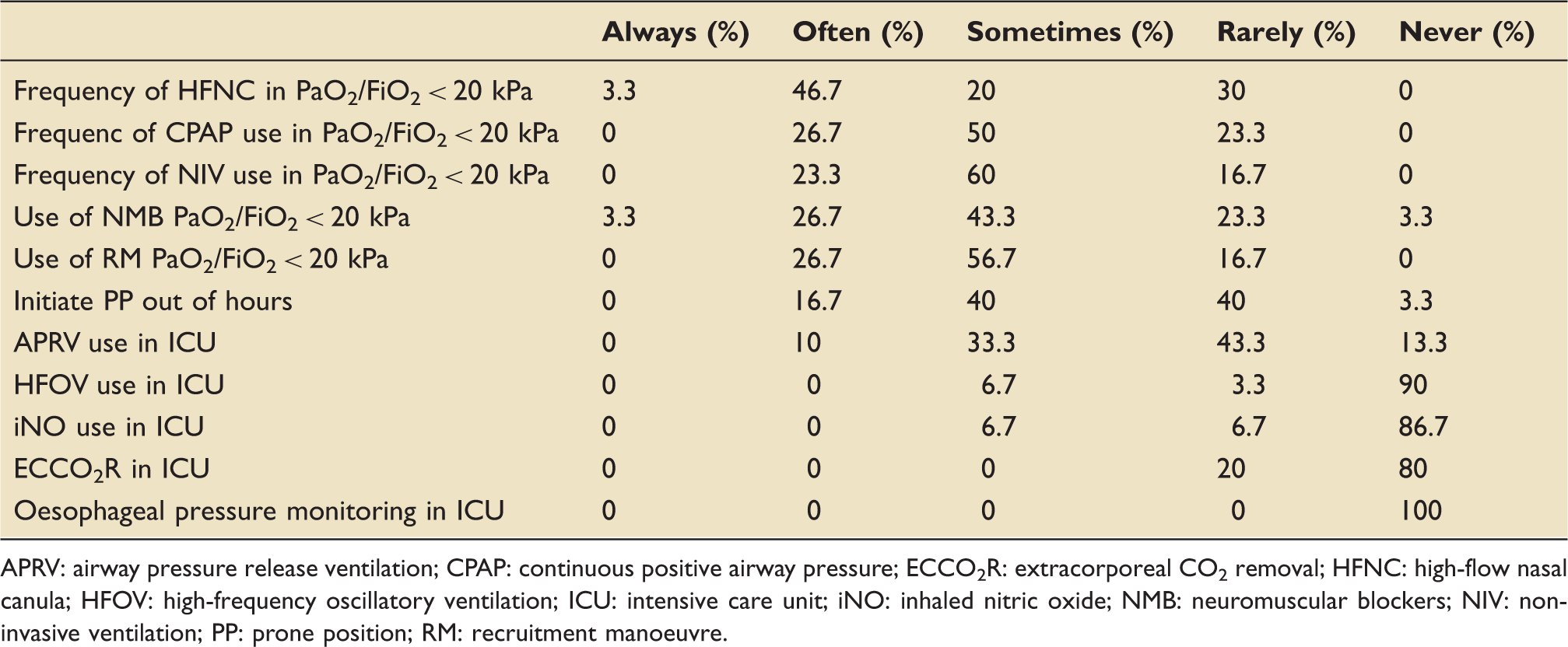
High-flow nasal oxygen (HFNC) was prevalent in South East England. When asked whether centres had the ability to provide HFNC on the ward, 66.7% reported they could do so, and 93.3% delivered high flow via dedicated device, e.g., Optiflow. HFNC was used in moderate hypoxaemic respiratory failure with PaO2/FiO2 < 20 kPa as a first therapy ‘often’ in 46.7% of respondents, and ‘sometimes’ in 20% of respondents.
CPAP and NIV
CPAP was used in moderate hypoxaemic respiratory failure with PaO2/FiO2 < 20 kPa as an additional therapy ‘sometimes’ in 50% of respondents and ‘often’ in 26.7% of respondents, while was ‘rarely’ used by 23.3% of respondents.
NIV was used in moderate hypoxaemic respiratory failure with PaO2/FiO2 < 20 kPa as an additional therapy ‘sometimes’ in 60% of respondents and ‘often’ in 23.3% of respondents, whilst it was ‘rarely’ used by 16.7% of respondents. Moreover, 83.3% of respondents could also use NIV on the ward if required.
Preferences on the use of RMs
Moreover, 56.7% of respondents reported only ‘sometimes’ using RMs in ICU, while 26.7% used it ‘often’. Only 16.7% of responders ‘rarely’ used RM. The largest proportion (30%) of centres perform recruitment by stepping up the PEEP level to 40 cm H2O with a specified duration of 40 seconds, while 13.3% used a decremental PEEP trial. In addition, 16.7% reported perform manual/bag recruitment.
Preferences on the use of ventilation strategy
When asked to describe the preferred ventilation mode, 90% used pressure-controlled ventilation, while 10% reported using volume-controlled ventilation. Tidal volume set was 6–8 ml/kg predicted body weight (PBW) in 53.3% and 4–6 ml in 46.7%. No participant reported using tidal volumes > 8 ml/kg PBW.
The PEEP selection was based on PEEP/FiO2 table in 50% of respondents and 20% reported using a decremental PEEP trial to identify “best PEEP” (PEEP associated with best compliance of the respiratory system).
Neuromuscular blockade
Infusion of NMB was used by 93.3% of participants. The preference was for atracurium infusion (43.3%), followed by cisatracurium (33.3%) and rocuronium (33.3%). However, NMB was used ‘often’ in 26.7%, ‘rarely’ in 23.3% and ‘sometimes’ in 43.3% in patients with P/F < 20 kPa. Only 3.3% of respondents used NMB routinely in all patients. Depth of blockade was measured with train of four by 53.3% of respondents and bispectral index monitoring routinely in only 13.3%.
Use of rescue and adjunctive treatments
The survey included domains about the use of additional and more advanced monitoring or ventilator techniques. Findings were summarised in Table 2 and Figure 2. None of the centres reported using oesophageal pressure monitoring to guide mechanical ventilation. As for advanced modes of ventilation, airway pressure release ventilation (APRV) was ‘never’ used in 13.3% of centres, while was ‘rarely’ or ‘sometimes’ used in 43.3% and 33.3% of cases, respectively. Moreover, 90% of respondents ‘never’ used high-frequency oscillatory ventilation or inhaled nitric oxide (86.7%).
Practices in use of respiratory therapies within intensive care units in South East England. APRV: airway pressure release ventilation; CPAP: continuous positive airway pressure; ECCO2R: extracorporeal CO2 removal; HFNC: high-flow nasal canula; HFOV: high-frequency oscillatory ventilation; ICU: intensive care unit; iNO: inhaled nitric oxide; NIV: non-invasive ventilation; NMB: neuromuscular blockers; PF:PF: Ratio of arterial partial pressure of oxygen to fractional inspired oxygen (PaO2/FiO2); PP: prone position; RM: recruitment manoeuvre. Practices in the use of respiratory therapies within intensive care units in the South East of England. APRV: airway pressure release ventilation; CPAP: continuous positive airway pressure; ECCO2R: extracorporeal CO2 removal; HFNC: high-flow nasal canula; HFOV: high-frequency oscillatory ventilation; ICU: intensive care unit; iNO: inhaled nitric oxide; NMB: neuromuscular blockers; NIV: non-invasive ventilation; PP: prone position; RM: recruitment manoeuvre.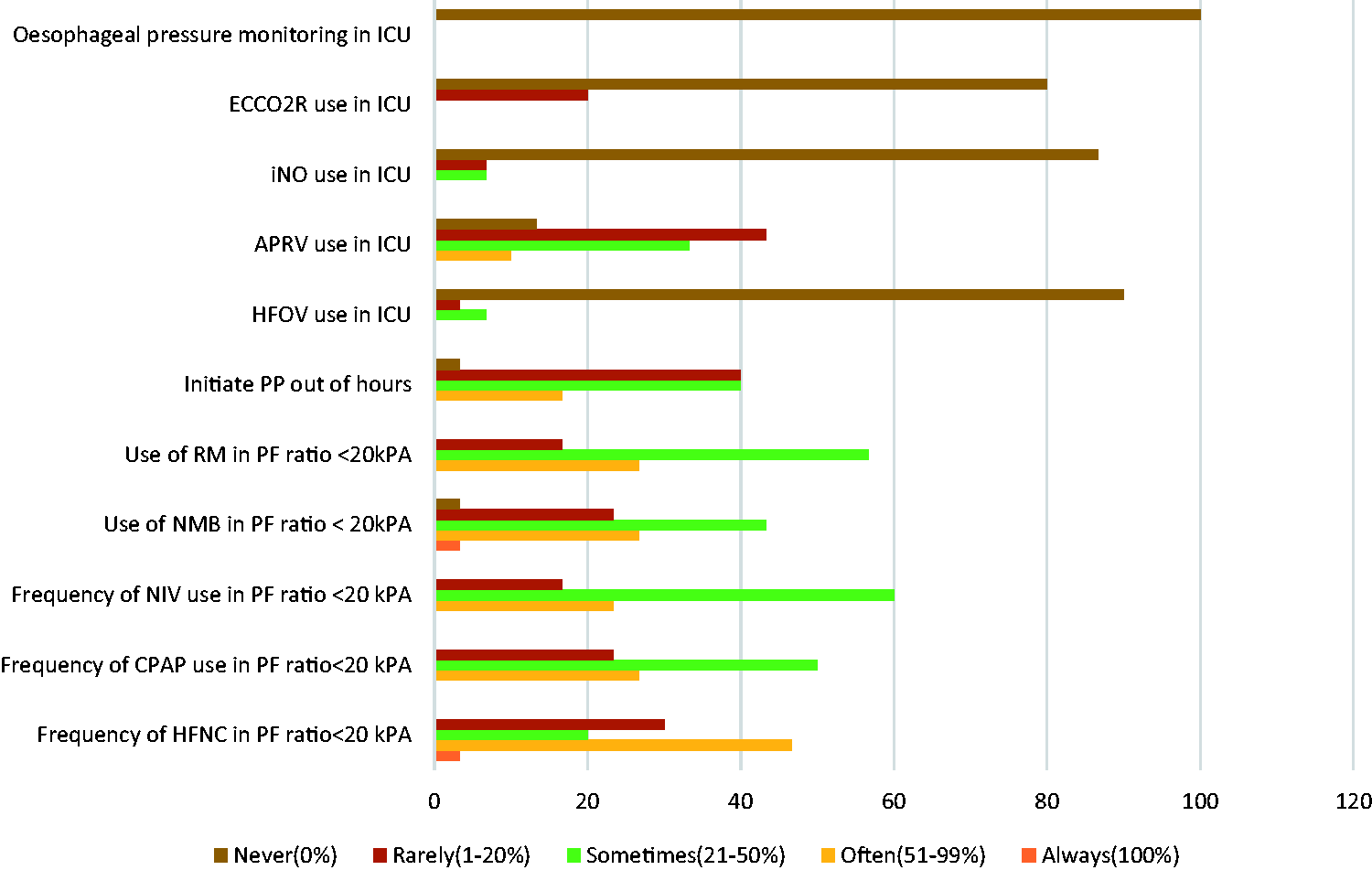
Prone positioning
Interestingly, the reported use of PP was high and its use as therapy for SRF was reported to be widely prevalent amongst centres. In addition, 90% of respondents had equipment for PP readily available in their ICU. Moreover, 80% of the centres reported to have a protocol in place and 46.7% of respondents have access to regular teaching or simulation in PP; 10% of respondents reported using PP for > 20 patients in one year; 26.7% between 11 and 20 patients/year and 30% between 6 and 10 patients/year. The most frequently reported duration of a PP session was 12–18 h. No respondent reported a PP session of less than 6 h. Only 3% of respondents reported ‘never’ using PP over the previous year. PP was initiated only occasionally out of hours with only 16.7% of respondents reporting out of hours PP ‘often’.
Discussion
The aim of this cross-sectional survey was to describe the practices and capabilities prevalent within the referral centres in South East of England. Overall, the respondents engaged well with the survey process with a response rate of over 70%.
Over two-third of respondents reported that high-flow therapy was available on the wards with more than half of them choosing HFNC as their first respiratory support in SRF. These findings are encouraging, as HFNC has been demonstrated to lower mortality in patients with acute hypoxaemic respiratory failure. 11
It was interesting to see that 83% respondents said that they could use NIV on the ward if required, but the prevalence of systematic or first-line use of NIV was low. This is in keeping with current literature showing that patients with moderate or severe ARDS had higher incidence of NIV failure and higher adjusted mortality, 12 particularly in de novo respiratory failure.13,14
In the FLORALI trial, authors found that the intubation rates were significantly lower in the HFNC as compared to the NIV group in patients with PaO2/FiO2 ratio < 200 mmHg. 11 There is lack of consensus in the use of NIV in non-hypercapnic respiratory failure. 15 This was evidenced by the variability in the use of NIV in various centres depending on case mix and local resources.
Regarding the tidal volume reported to be used, a large percentage of respondents aimed between 6–8 ml/kg PBW. This is consistent with the mean TV of 7.5 ml/kg observed in previous studies.16,17 This is in line with the current recommendations. 3
NMB was used by the majority of respondents – but not routinely and in all cases. This attitude and practice reflects both the evidence that NMB can help some patients with moderate and severe ARDS18,19 and the evidence from recent survey where it was found that NMB was used frequently to facilitate mechanical ventilation in patients with moderate to severe ARDS. 20 However, the fact that NMB is not routinely used is consistent with the recently published ROSE trial, 21 which showed that the systematic use of NMB does not appear to improve outcome.
The practice on the use of NMB was divided between atracurium (most prevalent), cisatracurium and rocuronium. Cisatracurium was used by one in three of respondents. The increased use of Cisatracurium over time may be due to its use in trials on ARDS.18,22 However, cost and availability may have reduced a more widespread use.
Well over half the respondents reported that they use RM in treatment of patients with moderate to severe ARDS. There was a wide variation in the way RM was performed. The response suggests that opinion on whether RM should be used and what technique applied is clearly divided. In the current literature, the application of RM has been a topic of debate. Although the use of the open lung concept has been suggested in refractory hypoxaemia, 23 in a multicentre trial examining the use of RM in moderate to severe ARDS, a strategy that included the systematic use of RM was associated with increased mortality. 24 In addition, RMs were used in 32.7% in patients with severe ARDS, which is slightly less than what was found in our survey.1,17 This may be due to a higher variability in practice amongst international centres as compared to regional centres which participated in the survey.
The most important and element of the survey is that PP was widely used with good governance in place. Indeed, almost all respondents reported good educational and infrastructure to deliver PP safely. Importantly more than one in three respondents reported having treated >10 patients in the year with 10% having delivered PP to more than 20 patients in the year of the survey. The duration and frequency of PP sessions were in keeping with a recent large prospective multicentre prevalence study which found the duration of the first PP session was 18 (16–23) h. The findings of our survey are consistent with increased use of PP in patients with moderate to severe ARDS. The increasing use of PP amongst the referral centres was encouraging. 19 This suggested that centres have the necessary expertise, protocols and educational resources for providing PP to patients with moderate to severe ARDS.
There are limitations to our study. Moreover, 90% of responses were from consultants, and their practice is assumed to be reflective of current practice in their ICUs. However, the potential for bias by the respondent’s personal preference cannot be ruled out. Furthermore, the application of a particular ventilation mode, such as APRV, or pharmacological intervention may be influenced by familiarity with their use.
Conclusions
In conclusion, we found variability in ventilatory practices. However, capabilities and practices well reflected recent evidence, including the use of high flow and the role of RMs. Additionally, in contrast to recent international surveys, PP was widely practiced with good availability of local protocols and educational resources.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.