
Abstract
Cannulation of the subclavian vein has many advantages when compared to other anatomical sites for central venous access. Difficulty in its ultrasonic visualisation, and the perceived consequent ‘higher’ complication rate, mean that this approach has fallen out of favour. This barrier, however, may now have disappeared. In this article, we discuss the indications, contraindications and complications associated with subclavian vein cannulation, and present an ultrasound-guided approach to infraclavicular subclavian cannulation.
Keywords
Introduction
Central venous cannulation is frequently necessary in the critical care environment. In recent years, the internal jugular and femoral veins have been most frequently accessed, largely due to the mandate to use ultrasonography for placement. 1 Subclavian vein cannulation, once commonly encountered, has since fallen out of favour – predominantly due to difficult ultrasonic visualisation and the perceived consequent ‘higher’ risk of mechanical complications such as pneumothorax.1,2 Persistence with the traditional ‘blind’ anatomical landmark technique has meant that for many units, cannulation of the subclavian vein has become a ‘last resort’, and as a consequence, the inevitable deskilling of clinicians is occurring, and many trainees have never performed subclavian cannulation. This approach, however, offers many advantages: rates of infection and thrombosis are substantially lower, patient comfort and tolerance are greater, and cannulation is often easier in hypovolaemic patients (as the clavipectoral fascia holds the vessel open).2–4 Furthermore, it may well be that the ‘high complication rate’ 1 of blind subclavian cannulation was overstated. Complication rates often reported metrics which were not serious or a problem, for example ‘failure of insertion’, 5 and a recent Cochrane review found no difference in rates of mechanical complications between subclavian, and internal jugular or femoral routes. 6 Despite this, a recent large multi-centre trial in 2015 did show that subclavian vein catheterisation was associated with a three-fold higher risk of pneumothorax when compared to jugular vein catheterisation (1.5% versus 0.5%). 3
Techniques for safe and efficient ultrasound-guided subclavian (or more specifically proximal axillary) vein cannulation have been described, but have yet to be commonly applied in clinical practice. 7 The predominant method involves the infraclavicular approach, using either the longitudinal (in-plane) or short (out-of-plane) ultrasound axis. Numerous studies compare ultrasound-guided and ‘blind’ subclavian cannulation.8–13 The largest of these (a randomised controlled trial involving 401 participants) demonstrated that cannulation rates by experienced operators improved when using longitudinal axis ultrasound (100% vs 87.5%), and rates of mechanical complications including pneumothorax, arterial puncture and haematoma formation reduced. 12 A similar advantage was reported amongst ‘less-experienced’ operators too (92% versus 44%), 9 with the findings subsequently confirmed in two large systematic reviews.11,13 In two Cochrane analyses evaluating the effectiveness of ultrasound for central venous cannulation, the success and complication rates of ultrasound-guided subclavian cannulation appear similar to that of ultrasound-guided internal jugular cannulation: success rate 944 per 1000 (subclavian) versus 952 per 1000 (internal jugular) and complication rate 58 per 1000 (subclavian) versus 39 per 1000 (internal jugular).11,14 In light of these data, and given the benefits of subclavian cannulation, perhaps it is time to revisit this approach now that this procedure can be real time ultrasound-guided.
Indications
The indications for central venous access are well rehearsed and need not be reiterated here. 15 Subclavian venous access can be considered whenever central venous access is required. Specifically, it is preferred in cases of cervical spine injury, and where tunnelled catheters or subcutaneous ports are needed for long term intravenous access, when maximising patient comfort and minimising infection rates are especially important.
Contraindications
Absolute contraindications to subclavian vein cannulation include thrombosis of the target vein, cellulitis or soft tissue infection of the overlying area, and fracture of the clavicle or proximal ribs. Whilst not an absolute contraindication, subclavian vein cannulation should also be avoided in patients with end stage chronic kidney disease, as the risk of subsequent vessel stenosis may compromise venous access options for future haemodialysis.16,17 Relative contraindications include coagulopathies (because of the difficulties in applying pressure to the vessels as they pass under the clavicle), and due to the increased risk of pneumothorax, the subclavian technique should be carefully considered in patients with severe respiratory failure or lung disease where a pneumothorax could cause significant deterioration in respiratory function.
Anatomy
The subclavian vein is a paired deep vein which drains the upper extremities. Each subclavian vein, the left and right, is a continuation of the axillary vein. The axillary vein begins at the lower border of the teres major and continues proximally until the lateral margin of the first rib where it becomes the subclavian vein. The subclavian vein then arches cephalad and passes posterior to the clavicle, before angling towards the sternal notch to join the internal jugular vein at the medial border of the anterior scalene muscle forming the brachiocephalic vein. The axillary and subclavian artery runs parallel alongside the vein, lying posterior and slightly superior.
At first glance, the anatomical path below and behind the clavicle suggests that the subclavian vein may be difficult to visualise using ultrasound. Moving the ultrasound probe laterally along the clavicle, however, enables visualisation of the infraclavicular proximal axillary vein and its surrounding structures, and thus real-time ultrasound-guided needle advancement into, and cannulation of, the vein. Strictly speaking, whilst the technique we describe is commonly referred to as ‘subclavian vein cannulation’ in the published literature, anatomically it is in fact an infraclavicular proximal axillary vein cannulation.
The structures lying close to the axillary and subclavian veins are of obvious concern when considering cannulation and can be identified using ultrasound. Laterally, the brachial plexus and axillary vein lie in close proximity and travel together in a neurovascular bundle (Figure 1). The brachial plexus usually lies posterior to the axillary vein placing it at risk of injury. In the middle section of the axillary vein, there are no vulnerable structures posterior to the axillary vein, and a misplaced needle is only likely to pass through axillary fat or muscle. More medially, the rib cage lies posteriorly to the axillary vein. As the axillary vein becomes the subclavian vein at the first rib, the pleural apex of the lung lies just inferior to it leading to the risk of pneumothorax. The thoracic duct terminates at the junction of the left subclavian vein and internal jugular vein, and this can also be injured during central venous cannulation. Tributaries of the axillary vein also need to be considered. The cephalic vein joins in the lateral portion of the axillary vein above the pectoralis minor. There are other tributaries that correspond with the branches of the axillary artery including the thoracoacromial, lateral thoracic, subscapular, anterior circumflex humeral and posterior circumflex humeral veins.
The veins of the right axilla. Source: Henry Gray (1918) Anatomy of the human body (Bartleby.com: Gray’s anatomy – Open access).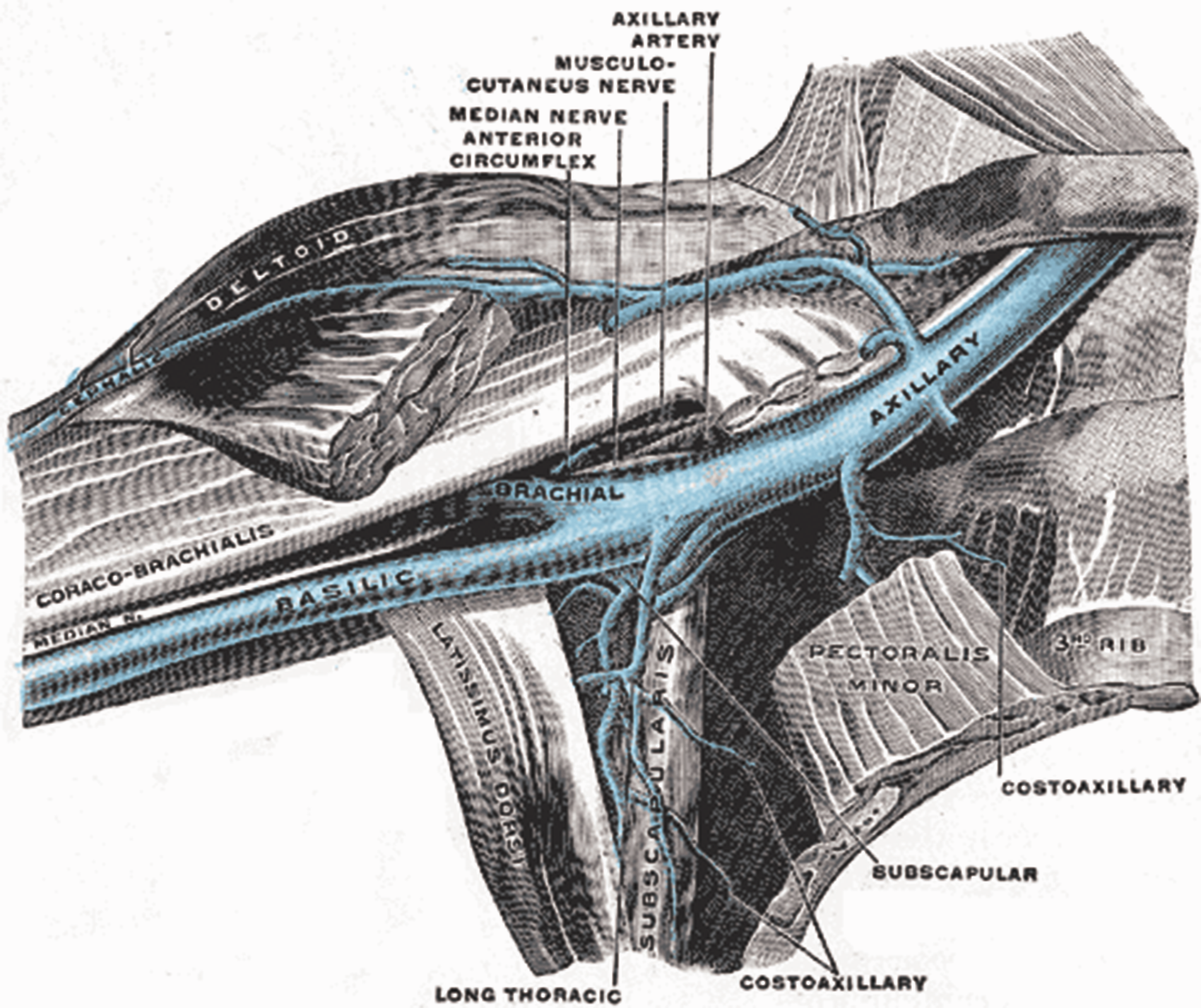
Short axis versus longitudinal axis view
Ultrasound-guided cannulation of the subclavian vein can be performed using both the longitudinal (in-plane) and short (out-of-plane) axis views in the infraclavicular proximal axillary approach. In the short axis view, the ultrasound beam is orientated in a transverse plane perpendicular to the target vessel such that the vessel is seen as a circular structure. The needle passes through the ultrasound beam; hence this view is also called ‘out-of-plane’. Advantages of this approach include better visualisation of nearby structures and relative ease for less experienced operators. 18 The disadvantage of the short axis view is that because a cross sectional image is produced, the needle tip looks similar to any other part of the shaft which may lead to unintended posterior wall puncture of the target vessel. In contrast, the longitudinal axis approach is performed with the ultrasound beam aligned parallel to the target vessel, and the needle is maintained within the plane of the ultrasound beam. The advantage of this approach is that entire needle can be visualised as it is inserted into the vessel. A study comparing the longitudinal versus short axis approach for subclavian vein catheterisation using simulation models demonstrated a decreased number of needle redirections (relative risk (RR) 0.5, 95% confidence interval (CI) 0.3–0.7) and posterior wall punctures (OR 0.3, 95% CI 0.1–0.9) when using a longitudinal axis approach. 19
Short axis view (out-of-plane)
This is obtained by placing the probe inferior and perpendicular to the clavicle, at a point roughly delineating the lateral third of the clavicle (Figure 2). This view offers the operator a good mid-line orientation for an out-of-plane guided needle approach.
Transducer placement and ultrasound image of the short axis view obtained for subclavian vein cannulation. Note the proximity of the pleura to the posterior wall of the vein. SCA: subclavian artery; SCV: subclavian vein.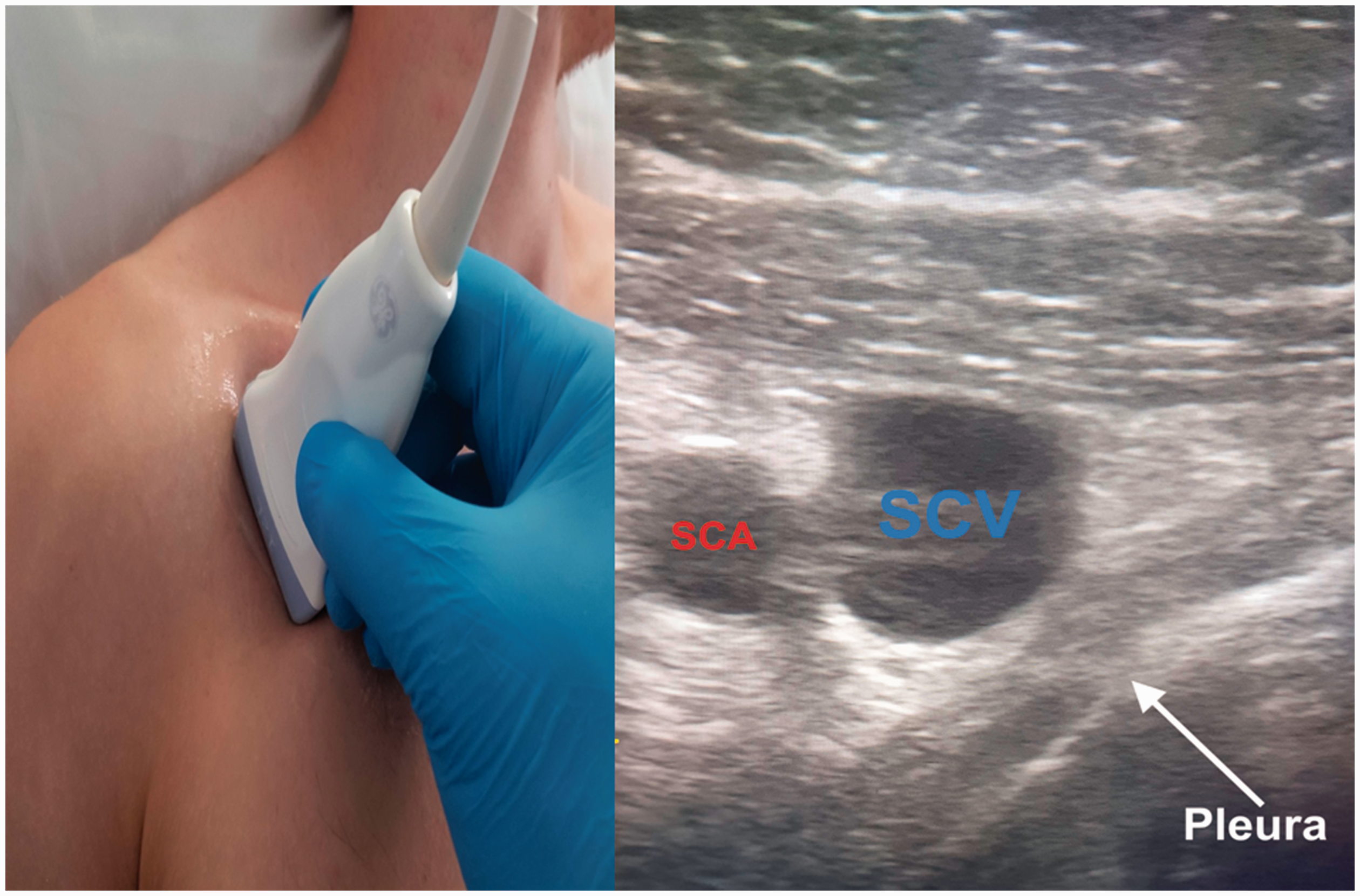
The probe marker should be orientated cephalad. The clavicle is visualised by moving the probe slightly cephalad and will appear as a bright echogenic line at the left of the ultrasound screen. The subclavian/proximal axillary vein will be visible, with the subclavian/proximal axillary artery typically visualised between the clavicle and vein. The vein is generally larger than the artery, is non-pulsatile and can be compressed under gentle pressure. Colour-flow Doppler imaging can help identify the vessels and determine their patency. The pleura is visible as a thin echogenic line below the vessels. Prior to needle insertion, the skin should be infiltrated with local anaesthetic. The introducer needle and syringe are then aligned with the midpoint of the transducer, with the long axis of the needle directed towards the sternum at an angle of around 45° to the skin. The skin is punctured, upon which the needle tip should be visible on the screen of the ultrasound machine. To minimise the risk of mechanical complications, the tip of the needle should remain visible at all times when advancing it towards the vein. This can be achieved by tilting the transducer back and forth, and it is imperative not to advance the needle if visualisation has been lost. The depth of the vein should be estimated using the ultrasound image, and the extent to which the needle has been advanced is closely monitored to avoid puncturing the pleura directly below the vessels. Venous puncture should be seen on ultrasound and is confirmed by aspiration of blood into the syringe. The syringe should then be disconnected to ensure that the blood flow is not bright red and pulsatile which may suggest arterial puncture; however, this is not a definitive test and if there are any concerns, consider transducing the needle to confirm venous cannulation. Introduce around 15–20 cm of the guidewire and confirm its placement in the vein by using the ultrasound to visualise it in the lumen in both the short and longitudinal axis views. Whilst holding the guidewire, remove the introducer needle and continue with catheter placement as normal.
Longitudinal axis view (in-plane)
This view is gained by first obtaining the short axis view as above. Once the target vessel is identified, position the vessel in the centre of the screen and rotate the transducer 90° to enable visualisation of the axillary vein/distal subclavian vein (Figure 3).
Ultrasound image of the longitudinal axis view obtained for subclavian vein cannulation. Confirmation of the vein should be carried out by colour/pulse wave Doppler and an assessment of vessel compressibility.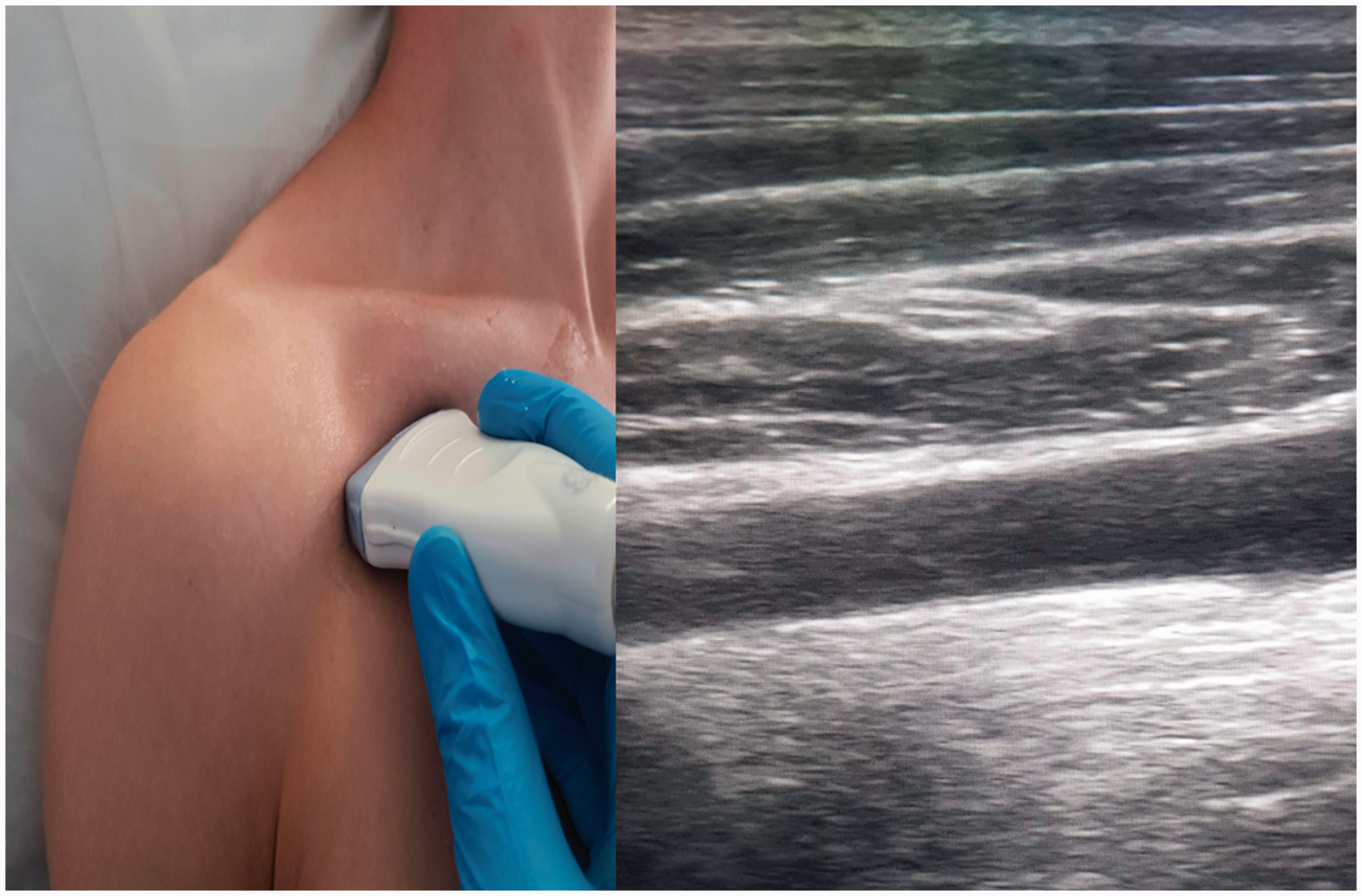
Tilting the probe cephalad allows visualisation of the pulsatile and non-compressible subclavian artery, which helps to differentiate between the artery and vein, and pulse wave Doppler can also be used to confirm identity of the vessel. Following skin infiltration with local anaesthetic, the introducer needle and syringe is aligned with midpoint of the short axis of the transducer, with the long axis of the needle directed towards the sternum. The skin is pierced, and needle advanced slowly towards the vein under direct visualisation. If sight of the needle is lost, then it is essential to stop advancing and either adjust the ultrasound probe to visualise the needle, or failing that, withdraw slightly until the needle is relocated. Venous puncture should again be confirmed by direct vision under ultrasound and aspiration of blood, whereupon the syringe should be disconnected, and the flexible guidewire introduced as above.
Catheter choice
Catheter choice depends on patient diagnosis and intended treatment. The subclavian veins can theoretically be used for any central venous catheter device. It should be noted, however, that the Kidney Disease: Improving Global Outcomes (KDIGO) group recommend avoiding large bore haemodialysis catheters in the subclavian veins due to the risk of vessel stenosis, which may compromise future access for haemodialysis in patients with end stage renal failure. 20
The optimal position of the catheter tip is the junction between the superior vena cava and right atrium. Fluoroscopically assisted measurements of guidewire length from the cutaneous puncture site to the superior vena cava–atrial junction have revealed mean distances of 18.4 cm for the right subclavian and 21.2 cm for the left subclavian vein. 21 The Association of Anaesthetists recommends using fixed length catheters: 20 cm for the right subclavian site and 24 cm for the left subclavian site. 1 In most cases, to avoid intracardiac placement, catheters should not be inserted more than 18–20 cm from any upper body access site. 21
Strategies to avoid complications and catheter tip misplacement
Conclusion
The subclavian vein offers numerous advantages over other commonly used anatomical sites for central venous cannulation. Ultrasound-guided techniques are associated with reduced mechanical complications and improved success rates when compared to the traditional ‘blind’ anatomical landmark technique. Current literature supports the use of infraclavicular ultrasound-guided techniques for cannulation of the subclavian vein, and the approach should be considered when central venous access is required.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.