
Abstract
During right internal jugular vein cannulation, complications can arise due to transfixion of the posterior wall and damage to other vessels. The risks to the subclavian artery and its branches are less well appreciated than the carotid artery. Example images are lacking in the literature. Using ultrasound and cadaveric studies, we aim to provide clinically relevant images of at-risk vessels posterior to the right internal jugular vein to emphasise their close proximity, and provide strategies to avoid potential complications.
Using ultrasound in 24 patients, we found the presence of numerous arterial vessels (excluding the carotid) within 8.0 mm of the posterior wall of the right internal jugular vein at the levels of the mastoid, cricoid and supraclavicular region. Cadaveric dissections further highlighted the close proximity of numerous branches of the subclavian artery.
Vulnerable branches of the subclavian artery include the thyrocervical trunk, inferior thyroid and vertebral arteries. More inferior approaches to right internal jugular vein cannulation are likely to put more arterial branches at risk. Higher resolution ultrasound enables visualisation of these arteries prior to cannulation. If identified, measures should be taken to avoid vein transfixion and arterial damage.
Introduction
The right internal jugular vein (RIJV) is a common site for central venous cannula insertion. The use of ultrasound to guide placement is now recommended.1,2 Complications of insertion are numerous and include damage to vessels located posterior to the RIJV. This can result from transfixion of the posterior wall of the vein, which can commonly occur even when using ultrasound, due to the collapsible nature of low pressure veins. 3 While the carotid artery is most at risk if it is behind the vein, it should be recognisable even with low resolution ultrasound devices by relatively inexperienced users.
Lower in the neck, the subclavian artery and its branches can be punctured if the posterior wall of the RIJV is transfixed, or the vein is bypassed, resulting in haemorrhage or arteriovenous fistula formation.4,5 We believe many operators are relatively unaware of the proximity of such vessels and there is little information in the clinical literature, showing ultrasound images or outlining clinical risks from such vessels. It is likely that some arterial punctures, and subsequent complications, attributed to the carotid actually arise from these vessels. With higher resolution ultrasound devices and more experienced users, these vessels can be visualised in most cases and therefore potentially avoided.
Arterial supply in the upper neck arises from branches of the external carotid and low in the neck from branches of the subclavian artery. Variations in the anatomy of the subclavian artery branches are numerous. 6 The subclavian artery and branches arising from its first part may lie directly posterior to the RIJV, making them vulnerable to damage from vein transfixion. Branches include the vertebral artery and the thyrocervical trunk. The latter according to textbook descriptions almost immediately subdivides into the inferior thyroid, superficial cervical and suprascapular arteries, but many individuals have variable patterns of branching.
Following informal clinical observations and clinical experience of complications in the past, we felt further study of applied anatomy was of interest. Using ultrasound imaging and cadaveric dissection, this study aims to demonstrate clinically relevant images of vulnerable vessels posterior to the RIJV low in the neck.
Method
Clinical study
After consultation with the local representative of the National Research Ethics Service, it was advised that ethical review was not required because the ultrasound imaging of the RIJV and anatomical relations formed a routine part of clinical evaluation immediately before a medical intervention and the images were kept anonymous.
Adult patients undergoing elective central venous access procedures, under local anaesthesia, for treatments such as cancer chemotherapy were prepared and consented for the procedure in the standard fashion. Access devices included ports, Hickman lines and apheresis catheters. Patients with previous surgery or pathology on the right side of the neck were excluded from the study.
Prior to cannulation, routine ultrasound imaging was performed with the subjects in a supine position with head turned slightly to the left side, resting on a standard pillow. Ultrasound images were acquired using a high-frequency linear probe 5-13 MHz (S-Nerve™; SonoSite, Hitchin, UK). Using the vascular setting and a field depth of 4 cm, the RIJV was identified in transverse cross-section and images were saved at three levels: the mastoid process, the level of cricoid cartilage and supraclavicular region with the probe as low as the clavicle would allow. The probe was held at approximately vertical and at right angles to the long axis of the neck at each level. Any vessels of interest posterior to the RIJV were imaged further, and Doppler imaging was utilised when appropriate. Images were labelled anonymously.
After reviewing the images, vessels posterior to the RIJV were identified. Due to the clinical nature of this study, with the awake patient positioned on the operating table awaiting a procedure, we could only spend limited time on the examination so could not conduct a detailed study of the course of all vessels and their branches. The distance between the posterior wall of the RIJV and the nearest posterior arterial vessels, other than the carotid artery, was estimated using a calliper measurement feature on a personal computer (GNU image manipulation program).
Anatomical study
Anatomical dissection of the neck was undertaken to further elucidate the relationships between the RIJV and other vessels, and provide anatomical images to complement the ultrasound images used clinically. The cadaveric study complied with the UK Human Tissue Act (2004), the UK Human Tissue Authority Code of Practice on Anatomical Examination and the Leeds Teaching Hospitals Trust/University of Leeds Joint Policy for the Storage and Use of Human Tissue.7–9 This was performed by S.S. as part of an intercalated BSc in anatomy in relation to medicine.
Three cadavers were dissected. Two were perfused with embalming fluid (industrial methylated spirit 75.6%, phenol 12.5%, formaldehyde 4%, glycerol 2.2%, water 5.7%) by gravity feed via the left common carotid artery. The other was embalmed with a phenol-free solution. Dissections were photographed and structures of interest highlighted by applying colour overlays in Adobe Photoshop.
The approximate distances between the posterior wall of the RIJV and vessels lying posterior to the RIJV were measured in these cadavers as well as seven other previously dissected necks using a calliper.
Results
Clinical study
Images were obtained from 24 patients (7 male and 17 female) with a mean age of 58 years (interquartile range 49-67 years). At the level of the mastoid process, six patients had vessels behind the RIJV (four internal or common carotid artery, one carotid bifurcation and one other vessel). At the level of the cricoid cartilage, eight had vessels behind the RIJV (three common carotid artery and five other vessels). In the supraclavicular region, 19 patients had one or more vessels behind the RIJV (19 subclavian artery and 12 other vessels). Figures 1 and 2 show representative examples of arterial vessels.
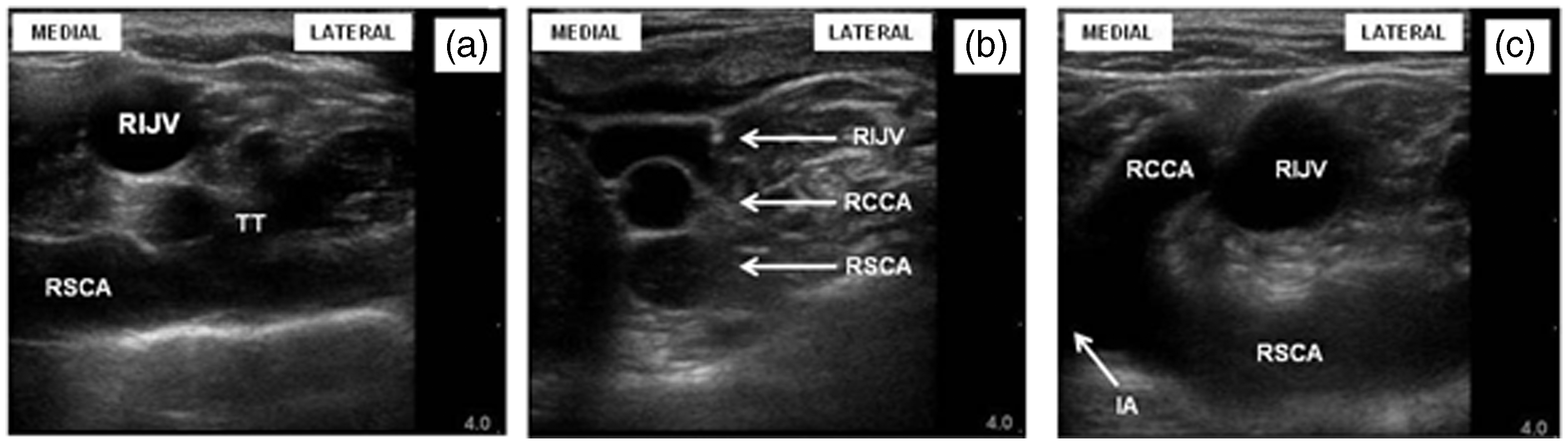
Example ultrasound images obtained at the three different levels showing the presence of arterial vessels behind the RIJV. (A) Level of mastoid with arterial vessel (a) behind vein; (B) level of cricoid with vessel (b) which is likely be an arterial branch of the thyrocervical trunk, veins adjacent to this artery are also seen; (C) level of cricoid (same patient as in B) with colour Doppler confirming pulsatile arterial blood vessel; (D) supraclavicular level with deeper vessels behind the RIJV. These are likely to be vertebral artery (d) and vertebral vein (c); (E) supraclavicular level (same patient as D) with colour Doppler. Variations in sonoanatomy seen in the supraclavicular region showing different configurations of vessels with vulnerable arteries behind the RIJV. (a) Thyrocervical trunk arising from the subclavian artery; (b) carotid and subclavian artery posterior to the RIJV; (c) subclavian artery behind RIJV, bifurcation of IA into RSCA and RCCA was also shown. RIJV: right internal jugular vein; RSCA: right subclavian artery; TT: thyrocervical trunk; RCCA: right common carotid artery; IA: innominate artery.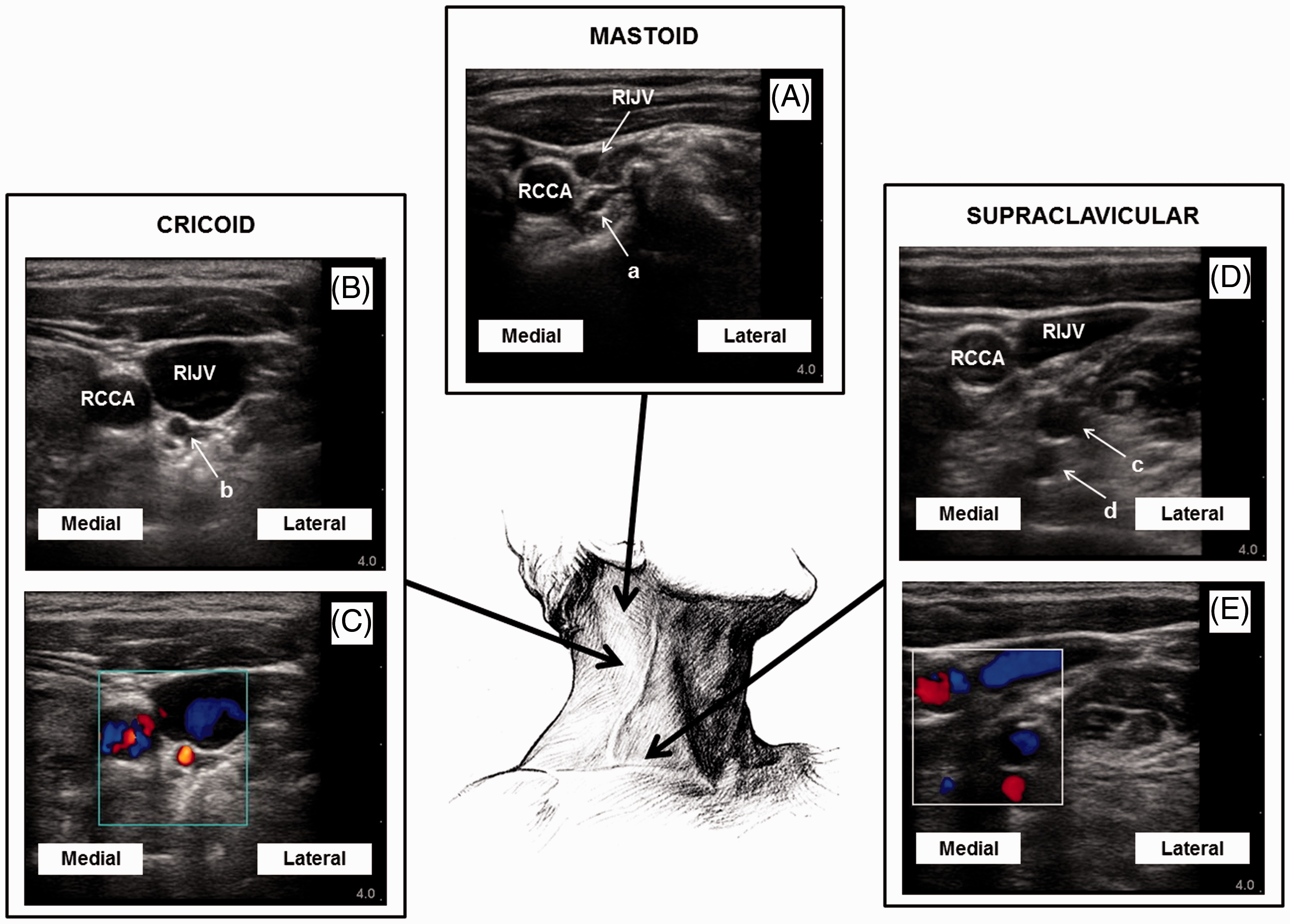
From the images, the distance between the posterior wall of the RIJV and the nearest arterial vessel (excluding the carotid) at the level of the mastoid was 2.3 mm; the mean distance was 1.3 mm (range 0.6-3.4 mm) at the level of the cricoid and 3.1 mm (range 1.0-7.8 mm) in the supraclavicular region.
Cadaveric dissections
In all three cadaveric dissections (one female, two male, age at death 76-89 years), the right subclavian artery and its initial branches were found posterior to the RIJV. There was considerable variation in the anatomy as shown in Figure 3.
Three separate colour-enhanced cadaveric images showing variations in anatomy and vessel calibre. (Not all structures are labelled) (a) Cadaver 39/10 – RIJV reflected downwards to show underlying anatomy; (b) Cadaver 11/11 – RIJV in situ showing vessels in proximity posteriorly; (c) Cadaver 29/11 – SCM reflected superiorly and RIJV removed to show further anatomical variation.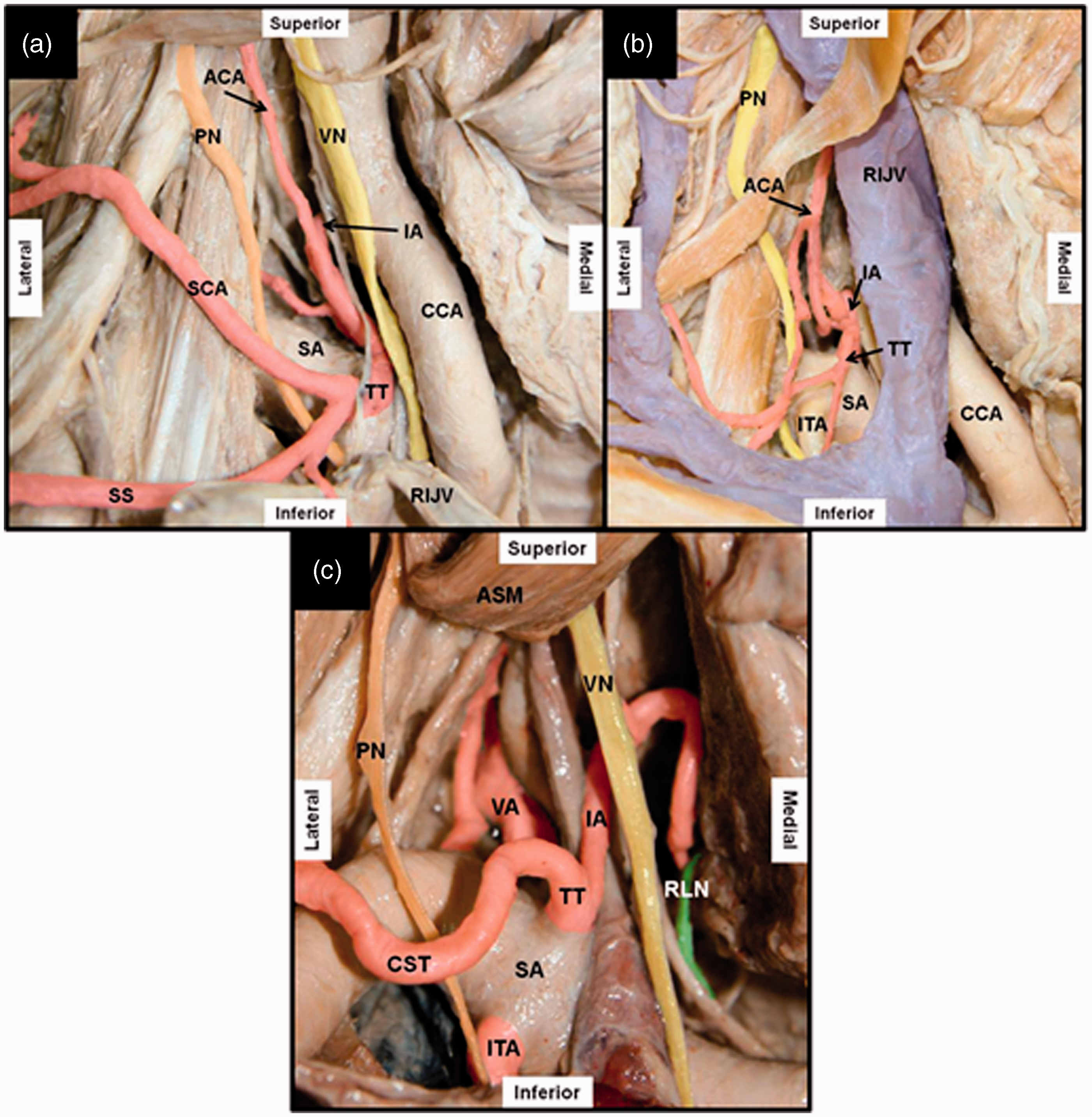
Measurements taken from the three cadaveric dissections and seven other previously dissected cadavers.

Note: In some cases, certain arteries did not appear posterior to the RIJV and were therefore not included in the calculation of the mean.
SA: subclavian artery; TT: thyrocervical trunk; ITA: internal thoracic artery; VA: vertebral artery; CCA: common carotid artery.
Figure 4 demonstrates vulnerable vessels in both the cadaver study and clinical study.
Comparable images (common carotid artery medial and not seen in any image). (a) Cadaveric dissection with RIJV cut and reflected downwards (viewed from front of the neck). The dashed line corresponds approximately to the US probe position in image 4b obtained from a live patient. (b) Ultrasound image (viewed from the patients head end). (c) Doppler to demonstrate arterial vessels. TT: thyrocervical trunk; SA: subclavian artery.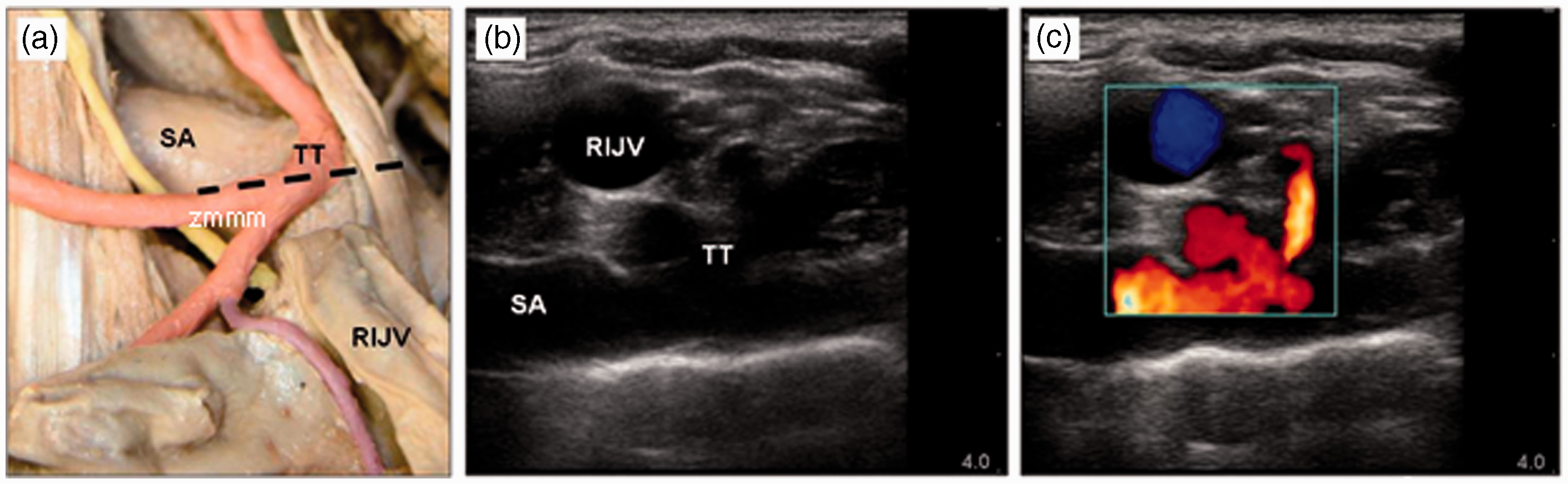
Discussion
Both the ultrasonic and cadaveric studies show the repeated presence of arterial structures behind the RIJV other than the carotid artery. These are potentially vulnerable during RIJV cannulation. While the proximity and danger of carotid artery puncture are well known, the anatomical considerations of the subclavian artery and its branches are, we believe, less well appreciated. This study shows that not only is the subclavian artery vulnerable, but branches such as the thyrocervical trunk (and its branches) and vertebral arteries are also in danger of transfixion. Similar findings are seen clinically in the left neck so it is likely our findings can be extrapolated to include right and left cannulation sites.10,11 In the paediatric population branches such as the vertebral artery have also been shown to be at high risk during mid-neck approaches. 12
Veins behind the RIJV are considered less of a risk due to less potential for bleeding but could be catheterised in error, with then the risk of guidewire or catheter malposition or more central vein damage as devices are attempted to be deployed via a blind-ended route. Vein puncture, if near to a simultaneous arterial puncture site, may result in an arteriovenous fistula which is a recognised complication in this area.13,14
With higher resolution ultrasound images available, it is important that such vessels are identified prior to the cannulation of the RIJV. 2 If these structures are identified, then careful consideration should be given to needle positioning and trajectory to avoid possible transfixion and align the needle tip away from such structures. Higher punctures may be safer in this respect but this may be difficult in adults or children with a short neck. Manoeuvres such as increased positive end expiratory pressure in ventilated patients or the Valsalva manoeuvre in conscious patients can also be utilised to increase the calibre of the vein, thus decreasing the likelihood of breaching the posterior wall.
Whilst we demonstrated the presence of vessels at the mastoid level, this is not so relevant clinically as such high approaches to cannulation are rare. Our results suggest that a lower approach to RIJV cannulation is likely to put more arterial branches at risk since more branches were demonstrated in both the ultrasound and cadaveric studies. It is important for operators to be aware of such variations in vessel anatomy and identify them during ultrasound guidance.
Our study had various limitations. Ultrasound is very user-dependant; small changes in probe angulation and position cause variation in images meaning that small vessels may be missed. The apparent posterior relations of the RIJV will vary with the angle of the probe. Nevertheless such anatomical relations are well described in standard texts and were consistently seen with ultrasound and cadaver dissections in this study. Due to the limited time for ultrasound examinations, it was not possible to perform complete Doppler imaging on all subjects, so some smaller identified vessels may have been veins rather than arteries. In the cadaveric study, postmortem measurements can differ from those in living subjects due to the dissection and shrinkage of fascia and other tissues.
Conclusion
During RIJV cannulation, the dangers of carotid artery puncture are well appreciated but damage to other vessels in close proximity behind the RIJV is also relevant. With improvements in ultrasound image resolution, these arterial vessels can be identified prior to venous cannulation in order to avoid transfixion and further complications. The subclavian artery and its branches including the vertebral artery and thyrocervical trunk are likely to be most at risk during lower approaches to RIJV cannulation.
Footnotes
Acknowledgement
We are grateful to the donors who bequeathed their bodies for anatomical examination.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.