
Abstract
Background
Iatrogenic hyperoxaemia is common on critical care units and has been associated with increased mortality. We commenced a quality improvement pilot study to analyse the views and practice of critical care staff regarding oxygen therapy and to change practice to ensure that all patients have a prescribed target oxygen saturation range.
Methods
A baseline measurement of oxygen target range prescribing was undertaken alongside a survey of staff attitudes. We then commenced a programme of change, widely promoting an agreed oxygen target range prescribing policy. The analyses of target range prescribing and staff survey were repeated four to five months later.
Results
Thirty-three staff members completed the baseline survey, compared to 29 in the follow-up survey. There was no discernible change in staff attitudes towards oxygen target range prescribing. Fifty-four patients were included in the baseline survey and 124 patients were assessed post implementation of changes. The proportion of patients with an oxygen prescription with a target range improved from 85% to 95% (χ2 = 5.17, p = 0.02) and the proportion of patients with an appropriate prescribed target saturation range increased from 85% to 91% (χ2 = 1.4, p = 0.24). The improvement in target range prescribing was maintained at 96% 12 months later.
Conclusions
The introduction and promotion of a structured protocol for oxygen prescribing were associated with a sustained increase in the proportion of patients with a prescribed oxygen target range on this unit.
Introduction
Supplemental oxygen is frequently administered to acutely ill patients in an attempt to prevent or treat hypoxaemia. 1 Following admission to a critical care environment, there is a risk that acutely ill patients will be exposed to high concentrations of oxygen for prolonged periods of time.2,3 Guidelines for supplemental oxygen use for the acutely unwell patient vary1,4,5 and there is little evidence to determine what constitutes a safe level of oxygen delivery. 6 However, many of these patients are exposed to hyperoxaemia as a result of excess oxygen administration2,3 and a growing body of evidence highlights the potential dangers of hyperoxaemia.6–8 The only randomised controlled trial completed, to date, of conservative versus liberal oxygen therapy in critical care patients reported mortality of 11.6% with conservative oxygen therapy (target range 94–98%) compared with mortality of 20.2% with liberal oxygen therapy. 9 However, this was a single-centre study. The results of the much larger ICU-ROX multi-centre study have been published very recently.10 This study did not demonstrate any difference in the primary outcome measure (ventilator free days) or any significant difference in 180 day mortality between ventilated ICU patients randomised to conservative oxygen therapy (target saturation range 91-96%) compared with “usual care” (target range ≥91%). However, the mean PaO2 of these patients was not widely different (108mmHg / 14.4 kPa in the usual care group and 90 mmHg / 12.0 kPa in the conservative oxygen group). This compares with mean PaO2 of 152 mmHg (20.3kPa) in 152,680 ventilated ICU patients who were audited in the same countries (Australia and New Zealand) between 2000 and 2009.11 Ferguson advised that critical care clinicians should aim for relative normoxaemia and avoid both hypoxaemia and hyperoxaemia, whilst the results of future trials are awaited. 12 Published studies have used different thresholds to define hyperoxaemia/hyperoxia.6–8 Ferguson suggested that oxygen saturation levels above 98% on supplemental oxygen could be regarded as evidence of hyperoxia. 12
It was established in the 19th century that high fractions of inspired oxygen are directly harmful to lung tissue in animals, and 20th-century research has suggested that this phenomenon is likely mediated by enhanced reactive oxygen species.13–15 More recent evidence in human subjects has shown that excessive oxygen administration leads to absorption atelectasis, coronary and cerebral vasoconstriction, reduced cardiac output, inflammatory cytokine production and central nervous system toxicity.1,6,16,17 Despite this evidence, many healthcare providers continue to view supplemental oxygen as a harmless therapy regardless of the presence or absence of hypoxaemia.18–20 Previous publications have shown high PaO2 levels amongst critical care patients in several countries. 21 This is of concern because of the growing number of studies that have identified increased mortality in association with hyperoxaemia.
Most published audits of oxygen prescribing in hospitals have excluded critical care units (CCUs) and have reported very low levels of formal prescribing. For example, only 18% of patients who were receiving supplementary oxygen in a New Zealand hospital in 2007–2008 had a formal oxygen prescription. 22 Formal prescriptions rose to 40% following the introduction of a dedicated oxygen prescription section on the drug chart and targeted education to medical staff. A review of the literature by Cousins et al. identified 12 papers from 2009 to 2015 relating to oxygen prescribing. Overall, the proportion of accurate oxygen prescriptions was low, with 10 studies reporting baseline of accurate target oxygen prescriptions ≤30%.The authors identified barriers to best practice including staff training, staff attitudes, institutional cultures and practical barriers related to prescribing systems. 23 Cousins' review identified a number of aids to better oxygen prescribing. These included formal prescription changes (electronic admission bundles, oxygen alert stickers, oxygen prescription section on drug charts) and educational measures (formal teaching sessions, information posters, hospital guidelines on oxygen prescribing). We have used several of these identified methods in this present study.
Audits of blood gas samples from the CCU at Salford Royal from 2005 to 2015 and at a district general hospital have demonstrated a gradual decline over that decade in the proportion of patients with oxygen saturations over 98% and the proportion with a PaO2 above the upper limit of normal (15 kPa). 24 This suggests that oxygen use in critical care has become more conservative in recent years, in line with the growing literature suggesting harm from hyperoxaemia, as discussed above.
The aim of this quality improvement pilot study was to implement carefully titrated oxygen therapy and to change staff attitudes and clinical practice to achieve a normal or near-normal target oxygen saturation range for most critical care patients, in line with the recommendations of Ferguson. 11 In addition, we aimed to identify the key factors that will be required to enable the future development of a simple and standardised protocol for oxygen therapy across CCUs in the UK.
Methods
The clinical team agreed on the improvement to be achieved (Spring 2017).
A consensus protocol was developed outlining appropriate target saturations to be prescribed for critical care patients. Target saturations were agreed by a panel of intensive care and respiratory consultants using the current national emergency oxygen guideline, as a guide for the management of non-ventilated patients.
1
As the British Thoracic Society Guideline does not extend to ventilated patients, we used consensus opinion, corroborated by up-to-date research and the Ferguson recommendations, to devise an agreed management strategy for ventilated patients.
11
All consultants in the CCU at Salford Royal approved the new policy that was implemented in this study. Our focus was to avoid hypoxaemia whilst minimising the potential hazards of hyperoxaemia. The following target ranges were agreed:
Ventilated patients: 94–98% target saturation for the majority of patients, with a target of 88–92% for patients at risk of hypercapnia (including severe chronic obstructive pulmonary disease (COPD), morbid obesity and significant musculoskeletal or neuro-muscular problems). Patients with acute respiratory distress syndrome or acute lung injury may have had patient-specific targets as determined by the senior treating clinician. Non-ventilated patients: a target of 94–98% was agreed, with the exception of patients at risk of hypercapnia who had a target of 88–92%. Again, patient-specific targets were determined by the senior clinician, for instance in carbon monoxide poisoning, the appropriate oxygen saturation target was 100%.
Adult patients undergoing active treatment on the CCU at Salford Royal NHS Foundation (SRFT) Trust were included in the study. Only patients aged under 16 years, or those receiving palliative care, were excluded. Salford Royal is a tertiary neurosurgical centre and thus has a significant proportion of patients with central nervous system injuries, commonly requiring ventilation. The standard was for all patients to have appropriate oxygen target saturations prescribed using the hospital's electronic prescribing system. Continuous or regular monitoring and recording of oxygen saturation using pulse oximetry, supplemented by intermittent arterial gases, was determined on an individual patient basis. For the majority of patients, this involved continuous monitoring of oxygen saturation, with hourly recording of observations on a bedside chart.
2. Methods to introduce change were agreed. (Spring 2017)
To promote safe and targeted oxygen prescribing, we focused on staff education to improve awareness and to address previous misperceptions including over-reliance on arterial blood gas readings to titrate FiO2, belief that hyperoxaemia is not potentially harmful, and that oxygen does not need to be prescribed. The lead clinicians of the project (ROD, PD, TF) were responsible for preparing staff for these changes and promoting their implementation. On initiation, the protocol (appendix one) was communicated to all staff on the unit through team meetings, emails and mounting copies at each blood gas analyser. The principles of the study were also regularly emphasised at daily nursing huddles and handovers throughout the duration of the study. Consultant staff were asked to encourage review of target saturation ranges on daily rounds. This was facilitated through their incorporation into the ‘ventilation’ section of the daily clinical review document universally used on the unit. Additionally, ‘Oxygen Champions’ were selected to promote these changes, highlight the underpinning principles and encourage regular checking of electronic oxygen prescriptions and adjustment of FiO2 to meet these targets. Champions recruited included doctors, physiotherapists and nursing staff on the unit who were fully educated on the protocol prior to undertaking the role. Prior to the pilot study, responsibility for oxygen management lay with individual clinicians. In most instances, medical staff decide on treatment plans which include oxygen therapy and they are responsible for prescribing all drugs including oxygen. Nurses at the bedside monitor oxygen use and a target range is usually written on the bedside monitoring documents. 3. Baseline data were collected to monitor evidence for effective change. (March–April 2017) The main measurements were the proportion of patients with targeted oxygen prescriptions and achieving appropriate target ranges (all oxygen prescriptions at this hospital require a specified target saturation range). We also monitored mean population PaO2 and SpO2 as secondary measures. Data were collected using a survey tool (appendix two) developed by the project leads (ROD, PD, TF). We recorded patient demographics, category of admission reason, mode of ventilation (if any), presence/absence and appropriateness of target oxygen prescription, risk factors for hypercapnia, FiO2, SpO2 and PaO2. Data were collected weekly over a period of five weeks in April and early May 2017 to obtain a baseline reference. No details of the study were disclosed to staff prior to the collection of baseline data to avoid risk of study contamination. On days when data collection occurred, all eligible patients on the unit were included. Measures closest to midday were taken to minimise collection bias and ensure patients had been reviewed by a senior clinician that day. As this was a pilot study designed to form the basis of a larger study, we did not perform a power calculation, but we aimed to recruit at least 50 patients for the baseline study. 4. Baseline staff attitudes were assessed through a survey. (April–May 2017) This explored their beliefs about current use of oxygen on the unit and appropriate target saturation ranges for different patient groups. The survey was distributed to all staff pre- and post-implementation of the changes to assess effectiveness of the education methods used during this process. The survey was developed by the lead clinicians on the study. Staff had the option to complete the study on paper (appendix two) or via an online link using SurveyMonkey. We aimed to get a minimum of 30 responses during each round of the survey. The unit employs approximately 180 trained nurses, 42 doctors and 12 physiotherapists. 5. The above changes to practice were implemented and championed on the Unit. (From 15th May 2017) 6. Monitoring of target range prescribing and staff attitudes were repeated in September–October 2017. 7. Target range prescribing was re-assessed July–August 2018.
Statistical method
This was a quality improvement pilot study so it was not possible to estimate the potential effect size prospectively. Data were entered in Graph Pad Prism 6 software and Chi-squared analysis was undertaken for the change in the proportion of patients with an oxygen prescription before and after the intervention.
Results
Summary of responses to staff attitudes surveys at baseline and at five months.
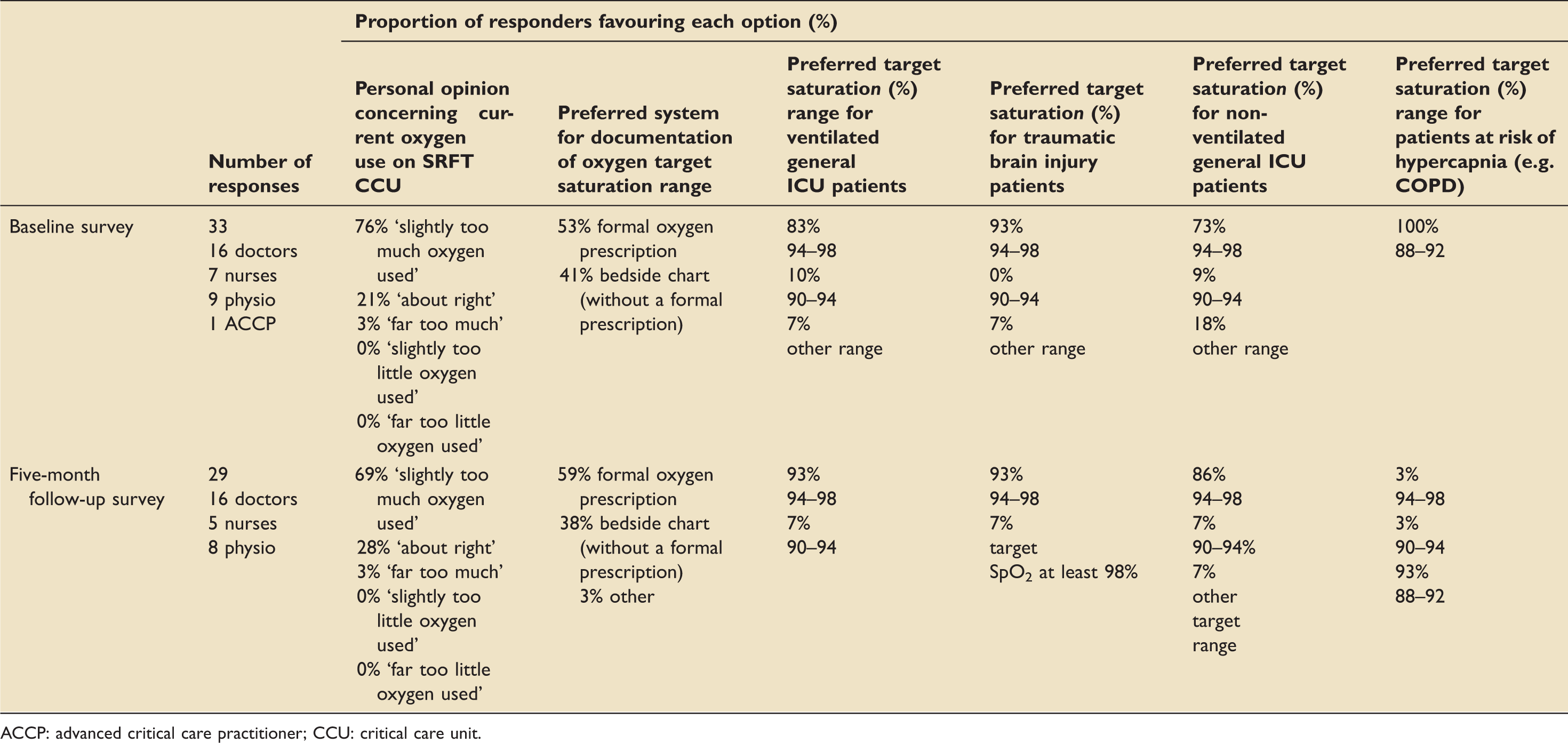
ACCP: advanced critical care practitioner; CCU: critical care unit.
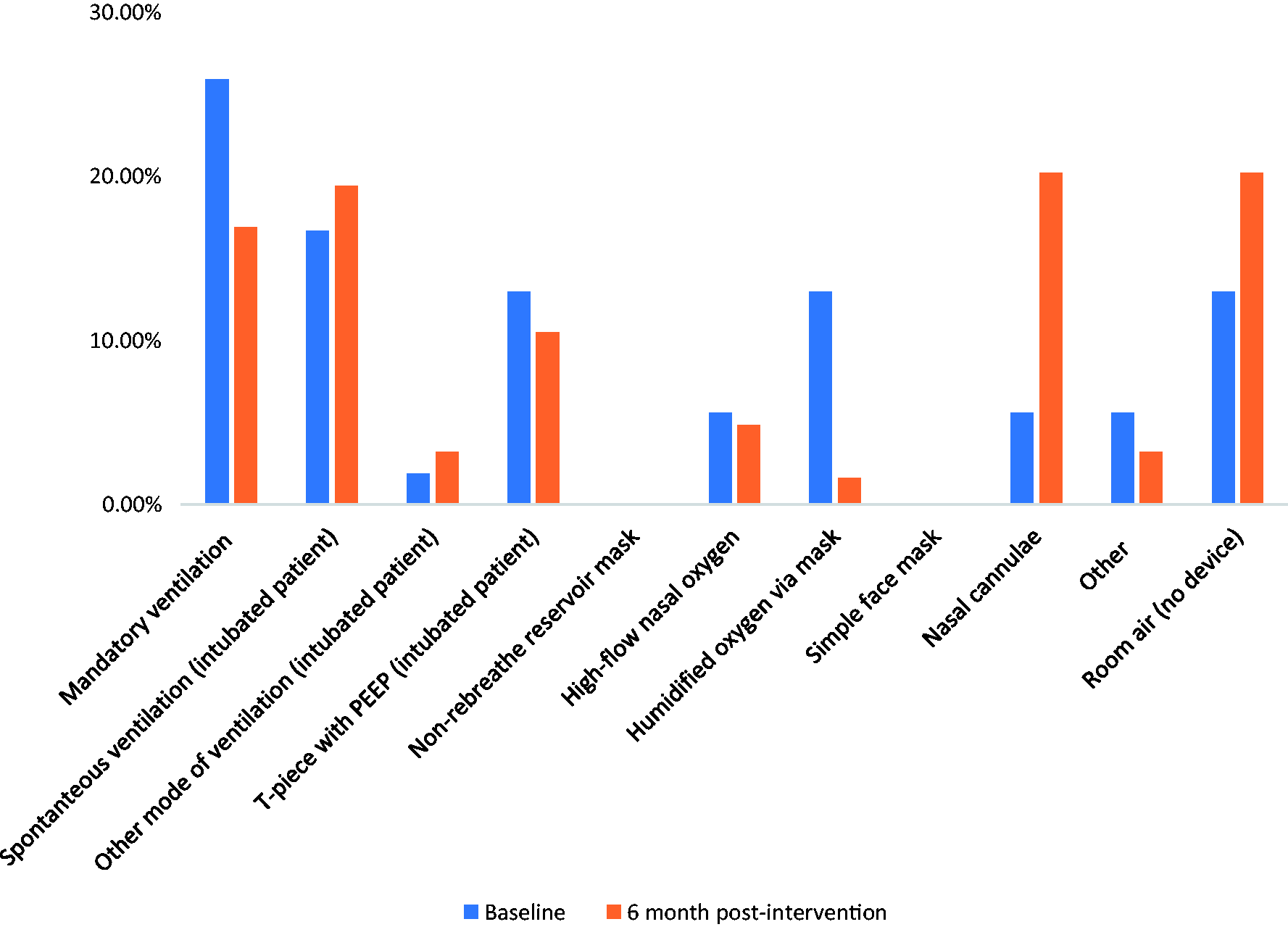
The demographics of the patients in the pre- and post-implementation of changes groups were broadly similar (Table 2), but considerably more patients were assessed at follow-up because the project team was larger at that time. Whilst the spread of admission category did differ between the two groups, the mode of ventilation remained relatively similar. The high proportion of traumatic brain injury (TBI) patients in both groups reflects the tertiary nature of the unit (Figure 1). The mode of oxygen delivery was similar in both groups, with intubated patients representing 58% and 49% of the numbers in the baseline and follow-up numbers, respectively (Figure 2). A higher proportion of patients at five months were on nasal cannulae or room air.
Proportion of patients in each category for CCU admission pre- and post-intervention. Proportion of patients by mode of oxygen delivery in the pre- and post-intervention groups. Demographics and clinical summary of patients assessed at baseline and five months later. CI: confidence interval.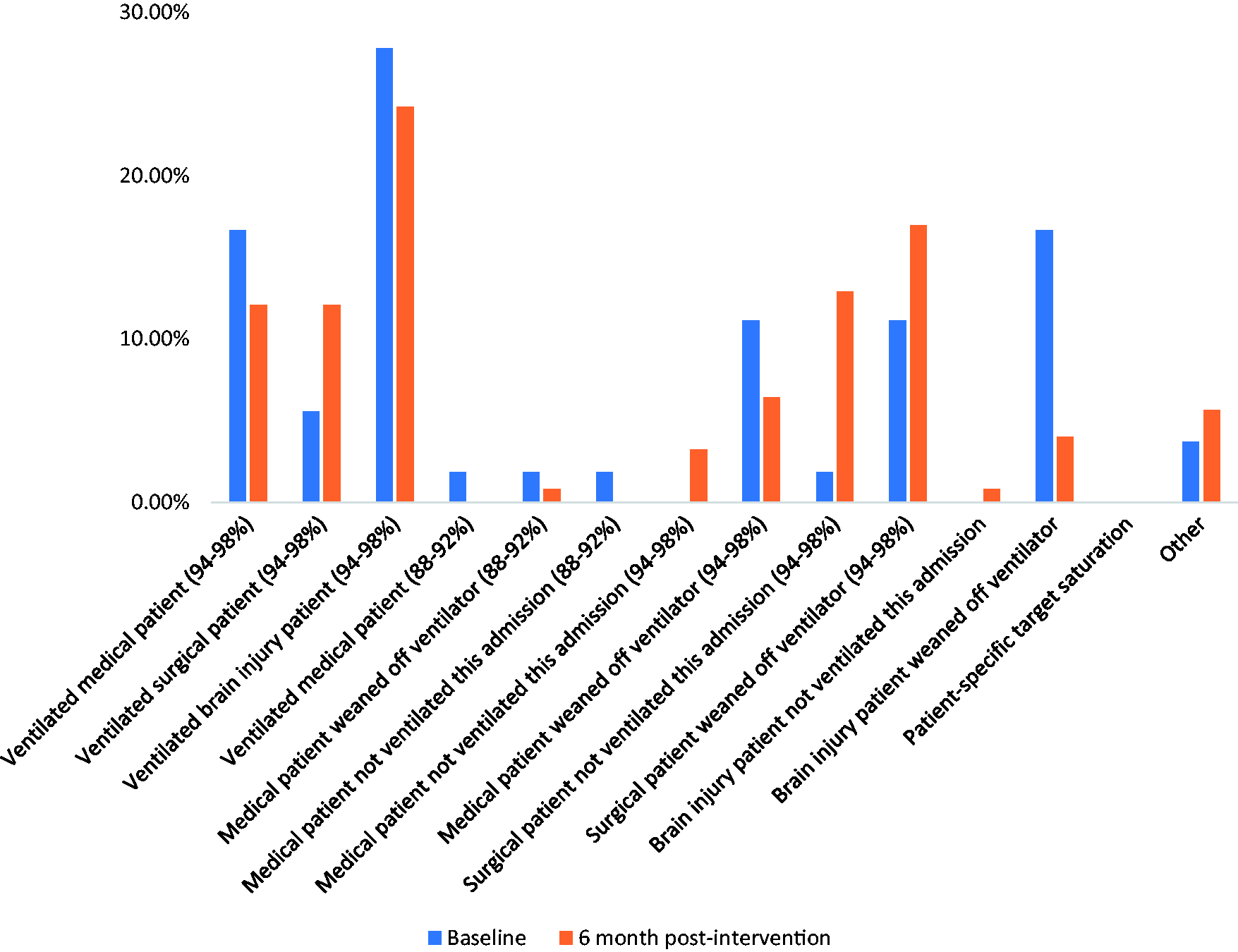
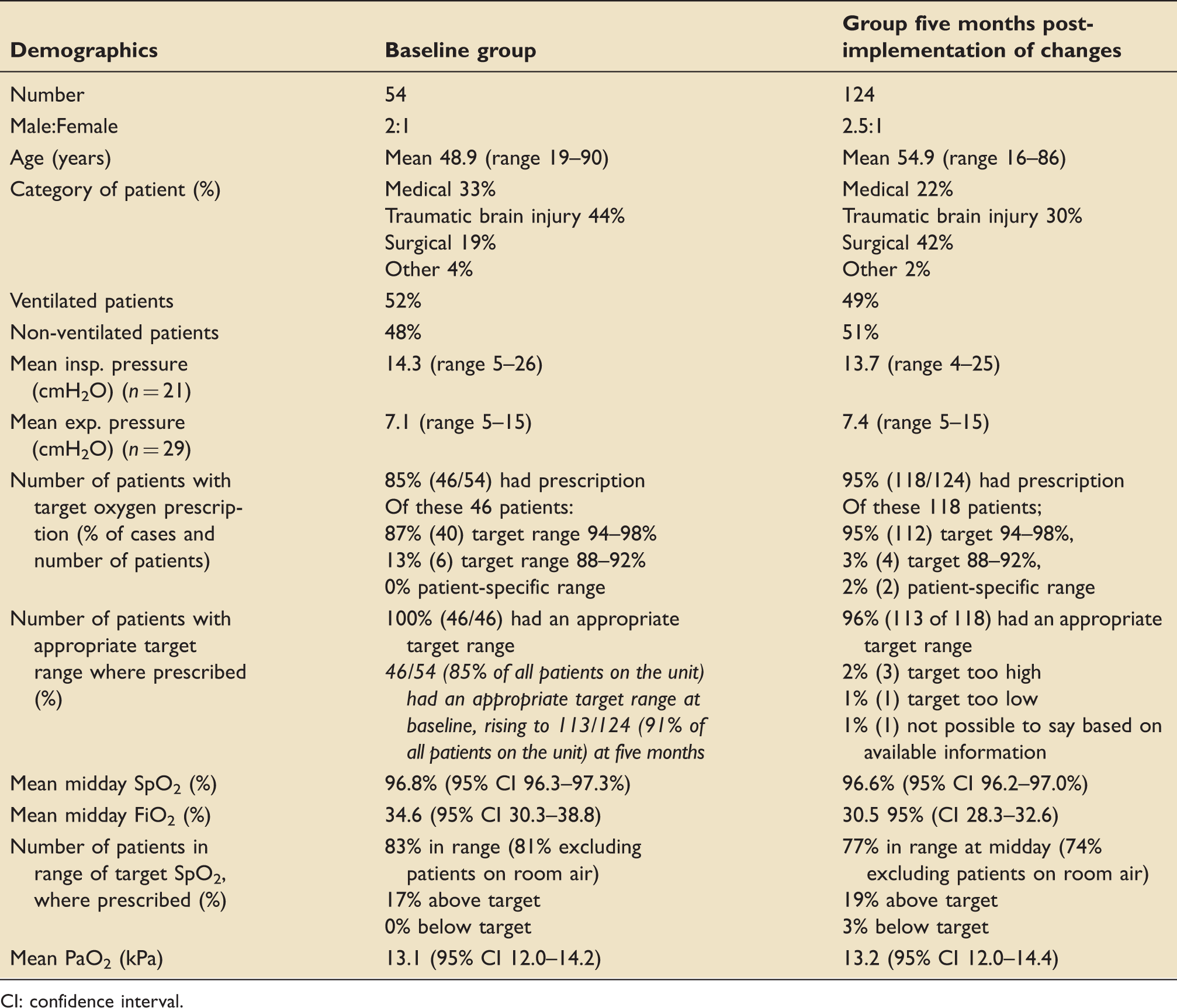
The proportion of patients with an oxygen prescription with a target range improved from a baseline of 85% to 95% at five months, thus achieving the intended improvement that was the goal of this study. This change was statistically significant (χ2 = 5.17, p = 0.023).
Arterial blood gas readings pre- and post-implementation of changes (where performed).

CI: confidence interval.
Number of patients with SpO2 within, above and below target range (within the cohort of patients who had a prescription with a target range).
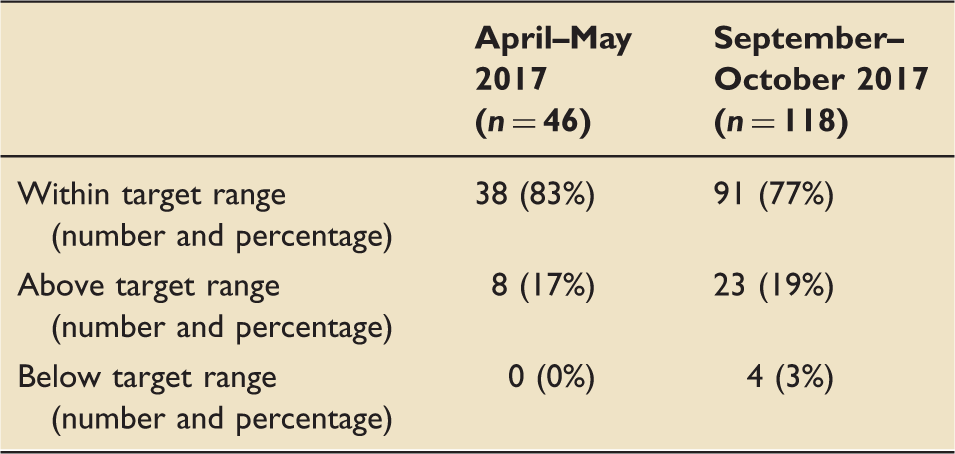
Figure 3 demonstrates the trend in hyperoxaemia (proportion of blood gas samples with SaO2 > 98%) on the unit from 2005 up to the end of this study in Autumn 2017. The respiratory and critical care teams at this hospital have been increasingly supportive of controlled oxygen therapy over this period of time and there has been a gradual fall in the proportion of patients with high oxygen saturation with a suggestion of an accelerated trend in response to the present intervention.
Trend of hyperoxaemia in patients on critical care (2005–2017).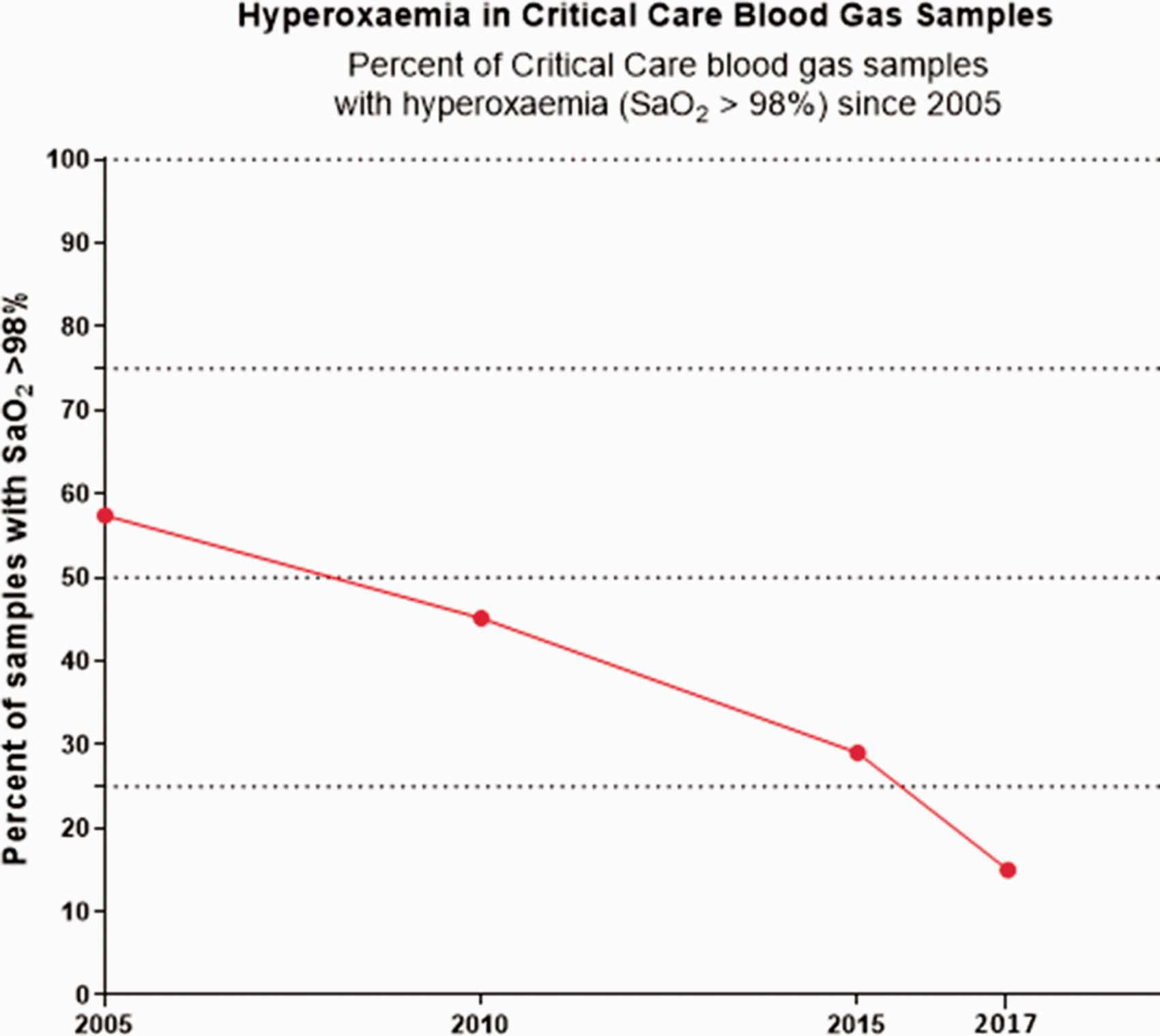
To ensure that the improvement in oxygen-prescribing was not a short-term success, target range oxygen prescribing of 124 patients was evaluated in July–August 2018. The proportion of patients with an oxygen prescription in 2018 was stable at 96% (Figure 4).
Targeted oxygen prescribing in the critical care unit, before and after the pilot study.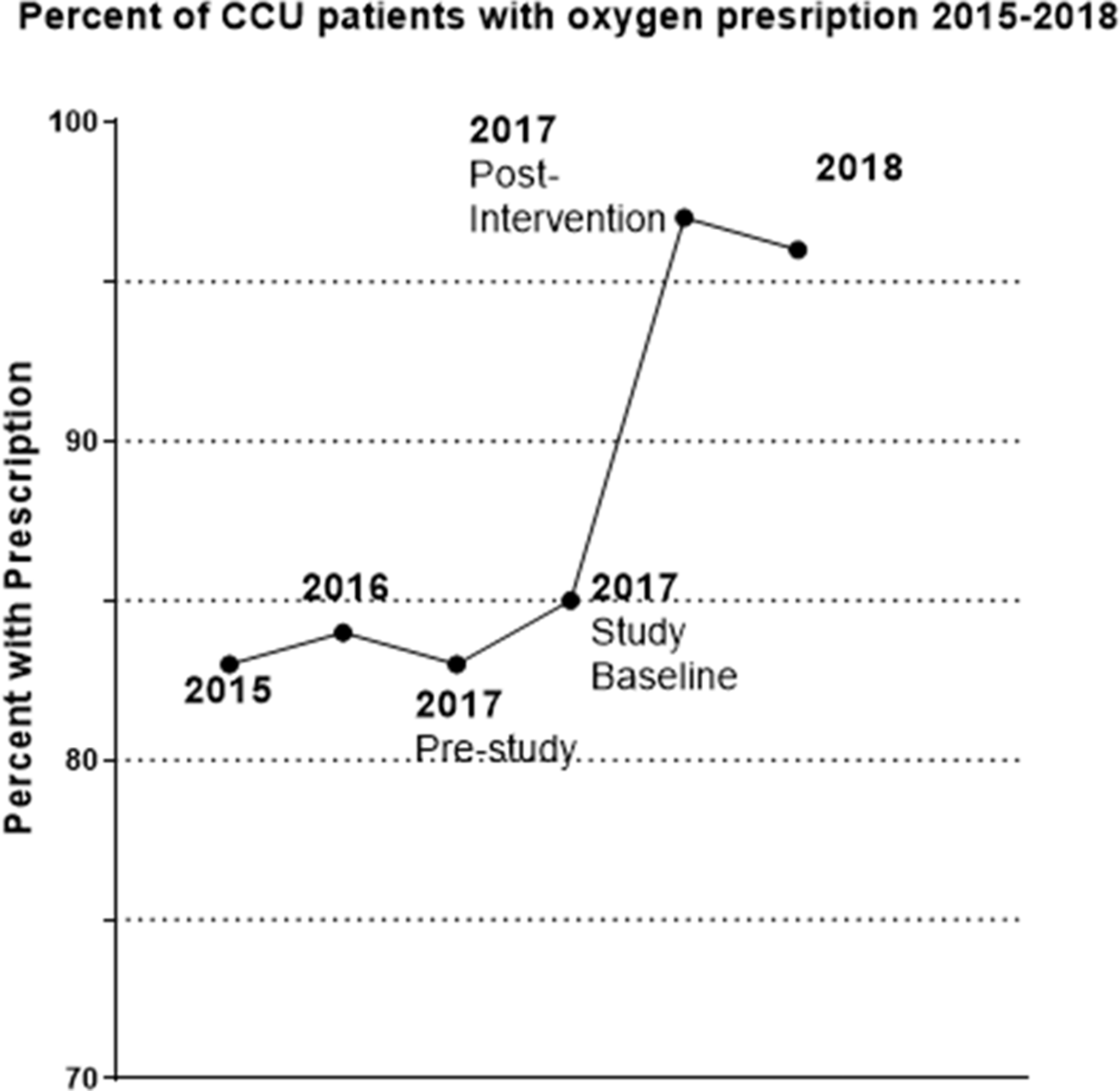
Discussion
This quality improvement pilot study has demonstrated that the introduction of a structured protocol for oxygen prescribing on a CCU was associated with an increase in the proportion of patients with a targeted oxygen prescription from 85% to 95%. Furthermore, the proportion of patients with what was judged to be an appropriate target saturation range increased by 6%. Because of the increased number of patients with a targeted prescription, there was a modest increase from 70% to 73% in the proportion of critical care patients who had their oxygen saturation within a pre-defined target saturation range. A repeat assessment in July–August 2018 (a year after the intervention) found that the rate of targeted oxygen prescribing remained high at 96%. This confirms that practice in the unit changed rapidly immediately after the intervention, and that the benefit was sustained. It is noteworthy that this increase was achieved despite a relatively high baseline compliance with targeted oxygen prescribing in this unit at 85%. This is compared to previous studies where the majority reported a baseline compliance of ≤30%. 23 A similar study in a unit with a lower baseline level of oxygen prescribing would probably show bigger changes. However, a much larger study would be required to show a difference in patient outcomes, such as length of CCU stay or mortality.
Our study did not demonstrate any detectable change in staff attitudes towards target saturation prescriptions over the course of the study. There may have been an above-average level of staff awareness of this issue due to previous educational initiatives on this unit. The majority of the staff reported that they felt that oxygen was ‘over-used’. In this setting, the implementation protocol facilitated change that most of the clinical staff already believed in. Introducing this protocol on a different unit with a lower level of oxygen prescribing and more ambivalent attitudes to hyperoxaemia might produce a greater change in the level of oxygen prescribing, but it may first be necessary to overcome resistance due to entrenched attitudes. We identified ambiguity in some of the questions and this will be addressed when we commission a multi-unit implementation plan. For example, we offered a choice of preferring formal prescriptions or bedside charts and we should have had an option of ‘both of the above’.
It is known from a UK national audit of 55,000 hospital patients that only 53% of patients using oxygen in UK hospitals in 2015 had a formal prescription with target range (compared with 94% at this hospital within that audit). 25 CCUs were not audited separately in the UK national audits but only 66% of patients receiving oxygen in level two care (Medical High Dependency Units) had a prescription in the 2015 UK national audit. An audit of 178 non-intubated CCU patients in Australia and New Zealand in 2013 reported that only 24% had a prescription for oxygen. 26
There was a slight improvement in staff understanding of our recommended target saturations in general ventilated CCU patients (83% at baseline, rising to 93% at five months) and general non-ventilated CCU patients without risk factors for hypercapnia. All responders in the group post-implementation of changes, who did not suggest a target range of 94–98% for these patients answered either ‘90–94%’ or ‘other’ with additional comments including ‘depends on co-morbidities’. This suggests a greater change in attitudes than reflected in the numbers and demonstrates high appreciation of the potential harms of hyperoxaemia following the intervention.
Interestingly, the proportion of staff selecting the ‘appropriate’ target saturation range for patients at risk of hypercapnia decreased from 100% to 93%, despite targets of 88–92% being clearly outlined in the protocol. However, this does not necessarily suggest poorer understanding as the phrasing of the question may have caused confusion. Indeed, many respondents suggested alternative target ranges for the ‘at risk of hypercapnia group’ or made qualifying comments such as ‘unless known CO2 retainer’. It will be necessary to rephrase this question in future studies to prevent ambiguity.
Although results of this study are encouraging, the number of survey responders was relatively small. Ensuring a larger number of responders in future studies would allow us to detect if attitudes differ across members of the multi-disciplinary team. This would enable a more tailored approach to education and improvement. Nursing staff were under-represented in the survey responses. It is important that this is addressed in future, because nursing staff are principally responsible for oxygen titration. Furthermore, staff turnaround on the unit may have contaminated the pool of responders in the post-implementation of changes group.
This study implemented multiple changes making it difficult to determine what the most effective aspects were. Nevertheless, these changes were all simple and a multi-faceted approach is indicated when implementing culture change. We implemented many of the changes that were reviewed by Cousins who acknowledged that it is not yet known which of these interventions has most effect. 23 The results demonstrate the success of this pilot study in increasing the proportion of CCU patients with a targeted oxygen prescription. Although there was a secular drift towards better oxygen prescribing on this unit over many years, Figures 3 and 4 demonstrate that there was a step change in response to the interventions introduced in May 2017. There was also a general improvement in understanding of appropriate target saturations and awareness of the potential harms of hyperoxaemia. However, no difference was seen in the proportion of staff favouring a formal oxygen prescription and this issue will need to be addressed going forward.
Whilst the changes implemented in this study led to an increase in the number of formal target oxygen prescriptions, we acknowledge that this did not impact oxygenation. However, the mean SpO2 and PaO2 were both within normal range in our baseline data. We therefore hypothesise that a unit with lower baseline proportions of target oxygen prescriptions would also have higher levels of hyperoxaemia. Indeed, other CCUs audited internationally have shown an above normal mean PaO2.20,21 The results of this quality improvement pilot study are aligned with longer term trends on this unit which have shown a declining prevalence of hyperoxaemia. We have designed an effective protocol to implement national guidelines on oxygen prescribing. It is likely that implementation of our protocol across other CCUs with a greater baseline prevalence of hyperoxaemia, and lower proportions of target oxygen prescriptions, would lead to larger changes in oxygen prescribing practice and a demonstrated reduction in hyperoxaemia. We are presently in the process of designing a step-wedge cluster designed multi-centre study of promoting oxygen prescribing by target range in CCUs.
Supplemental Material
INC892784 Supplemental Material1 - Supplemental material for Implementing target range oxygen in critical care: A quality improvement pilot study
Supplemental material, INC892784 Supplemental Material1 for Implementing target range oxygen in critical care: A quality improvement pilot study by Rosie Heartshorne, Jenna Cardell, Ronan O'Driscoll, Tim Fudge and Paul Dark in Journal of the Intensive Care Society
Supplemental Material
INC892784 Supplemental Material2 - Supplemental material for Implementing target range oxygen in critical care: A quality improvement pilot study
Supplemental material, INC892784 Supplemental Material2 for Implementing target range oxygen in critical care: A quality improvement pilot study by Rosie Heartshorne, Jenna Cardell, Ronan O'Driscoll, Tim Fudge and Paul Dark in Journal of the Intensive Care Society
Supplemental Material
INC892784 Supplemental Material3 - Supplemental material for Implementing target range oxygen in critical care: A quality improvement pilot study
Supplemental material, INC892784 Supplemental Material3 for Implementing target range oxygen in critical care: A quality improvement pilot study by Rosie Heartshorne, Jenna Cardell, Ronan O'Driscoll, Tim Fudge and Paul Dark in Journal of the Intensive Care Society
Footnotes
Acknowledgements
We would like to thank the following for their assistance in the conduct of this study.
Dr Hayley Millar and Lisa Porritt (physiotherapy) for assistance with the study design and implementation, Jill Bentley (ACCP), Dr Martha Pearson and Dr Diana Chiu for assistance with data collection and all staff members on the Salford Royal Critical Care Unit who helped with this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.