
Abstract
Introduction
This is the first comprehensive evaluation of Burnout Syndrome across the UK Intensive Care Unit workforce and in all three Burnout Syndrome domains: Emotional Exhaustion, Depersonalisation and lack of Personal Accomplishment.
Methods
A questionnaire was emailed to UK Intensive Care Society members, incorporating the 22-item Maslach Burnout Inventory Human Services Survey for medical personnel. Burnout Syndrome domain scores were stratified by ‘risk’. Associations with gender, profession and age-group were explored.
Results
In total, 996 multi-disciplinary responses were analysed. For Emotional Exhaustion, females scored higher and nurses scored higher than doctors. For Depersonalisation, males and younger respondents scored higher.
Conclusion
Approximately one-third of Intensive Care Unit team-members are at ‘high-risk’ for Burnout Syndrome, though there are important differences according to domain, gender, age-group and profession. This data may encourage a more nuanced understanding of Burnout Syndrome and more personalised strategies for our heterogeneous workforce.
Keywords
Introduction
Intensive Care Units (ICUs) attract staff who are typically dedicated, driven and invested. These traits should help ICU healthcare professionals (HCPs) deliver patient-care that is safe, expedient and empathic. ICU HCPs may not, however, attend to their own psychological needs or those of colleagues. This workplace also comes with inherent stressors and distractions. Examples include competing demands, interpersonal conflict, complex decision making, 1 moral distress, 2 rapid patient turnover, 3 night and weekend work and patient mortality. There needs to be balance between personality traits, job demands and support systems to achieve employee wellbeing, as described by the Job–Demands–Resources model. 4
Imbalance can impair practitioner wellbeing, increase work-related stress and lead to Burnout Syndrome (BOS). 5 BOS can also include physical symptoms, such as tiredness, insomnia, emotional liability, frustration and anxiety. 6 BOS influences caregiver health both in and out of work. It threatens patient care, given the association with increased absenteeism and staff turnover, less innovation, reduced safety, decreased efficiency and greater costs. 7 While there is an increased interest in BOS, there is a dearth of objective data. This is the first study to interrogate BOS in UK ICU multi-disciplinary HCPs. It was performed on behalf of the UK Intensive Care Society Wellbeing Working Group.
BOS was described as a psychological concept in the 1970s and refined by Maslach and Leiter. 8 It is not a dichotomous clinical diagnosis, but rather one end of a spectrum of reduced workplace wellbeing, and the opposite of workplace engagement. Rather than ascribing a single ‘burnout score’, or suggesting everyone experiences BOS the same way, Maslach outlined three BOS domains: (i) Emotional Exhaustion (a feeling of nothing left to give); (ii) Depersonalisation (whereby caregivers feels disconnected, negative or cynical) and (iii) lack of Personal Accomplishment (whereby caregivers feel inadequate and ineffective in their work). By interrogating all three domains of the Maslach Burnout Inventory (MBI), we aim to examine how different HCPs manifest BOS. Our goal is to encourage a more nuanced, understanding and demonstrate why crude mandatory testing or ‘one-size fits all’ interventions should be avoided.
There is a heightened concern regarding BOS throughout medicine and nursing, but particularly high rates are reported in ICU professionals. 9 For example, approximately 50% of adult ICU doctors,6,10 over 70% of paediatric ICU doctors 11 and over 80% of critical care nurses are reported to be high-risk in at least one domain. 12 However, there have been methodological criticisms, with variation in definitions, measures and interpretation. For example, cut-offs for ‘high-risk’ of BOS differ. Moreover, whereas some groups define BOS based upon ‘high-risk’ scores in individual domains, others require ‘high-risk’ scores in all three. There is also a paucity of data regarding ICU multidisciplinary team (MDT) members other than doctors or nurses, aside from a 2002 postal survey which used a general health questionnaire. 13 Accordingly, a worldwide ‘call to action’ was issued by the Critical Care Societies Collaborative in 2016. 6 This included the need for more data and greater consistency. Given the perceived importance of BOS, insufficient data, the putative benefit from examining three BOS sub-domains and the need to include other HCPs, we conducted the full MBI questionnaire throughout the ICU MDT. We subsequently analysed whether BOS risk in the three domains is associated with profession, gender and age.
Methods
Part one of this two-part questionnaire requested basic demographic data including professional group, age bracket and gender. Part two consisted of the 22-item self-completion Maslach Burnout Inventory Human Services Survey (MBI–HSS), adapted for Medical Personnel (MP). 14 The MBI–HSS is one of the three primary versions of the MBI. It was developed by Maslach et al. 14 and is unchanged since 1981 and has good reliability and validity. The MBI–HSS–MP is worded to reflect its medical context.
Respondents reported, via a seven-point Likert scale, how frequently, in relation to work, they experience the feeling described in each of the 22 items. Each item pertains to one of three sub-scales, namely the three domains of BOS: Emotional Exhaustion (nine items), Depersonalisation (five items) and Personal Accomplishment (eight items). We purchased 1000 MBI–HSS–MP licenses from MindGarden 15 authorising online anonymous survey completion. In compliance with the license, we transcribed the questionnaire into Survey Monkey 16 with subsequent results transferred to SPSS 17 for analysis.
Participant invitation was through an electronic link within an email. This was sent to all delegates attending the Intensive Care Society State of the Art meeting (December 2017, Liverpool, UK) and to all multi-disciplinary members of the UK Intensive Care Society (May 2018), where it was accessible for 30 days. Instructions included our intent to publish anonymous composite results, the voluntary nature of involvement and the MBI–HSS–MP copyright.
Data were interpreted in accordance with the MBI Manual. 14 The seven points on the Likert scale were assigned a score of 0–6, with 0 corresponding to ‘Never’ and 6 being ‘Every Day’. The score for each of the items was summed to give a total domain score. Importantly, the MBI manual recommends that the ‘sum’ scores for each of the three domains be interpreted separately. Accordingly, we have not provided a single burnout score. However, to compare our data against previous studies and to analyse the association with demographic factors, the sub-scale scores were stratified according to level of ‘risk’ of BOS, with the same cut-offs as previously published. 10 ‘High risk’ for each of the three domains was defined as ≥27 for Emotional Exhaustion, ≥10 for Depersonalisation and ≤33 for Personal Accomplishment (an inverse relationship to Burnout).
Statistical analysis
Data were extracted from Survey Monkey and transferred to SPSS. Only complete MBIs were included. Categorical (proportional) data were presented as percentages and continuous data (burnout scores) as medians and IQR. Proportional data were compared using the chi-square test or Fishers exact test as appropriate. Continuous variables were not normally distributed, as assessed by the Shapiro–Wilk test; hence, comparisons were drawn using non-parametric tests such as the Mann–Witney U test or Kruskall–Wallis tests. A univariate linear regression model was constructed to identify the potential predictors of individual BOS scores. The model included age, gender, professional background and the scores from the two other domains. P values of < 0.05 were interpreted as significant.
Results
Characteristics of questionnaire participants.
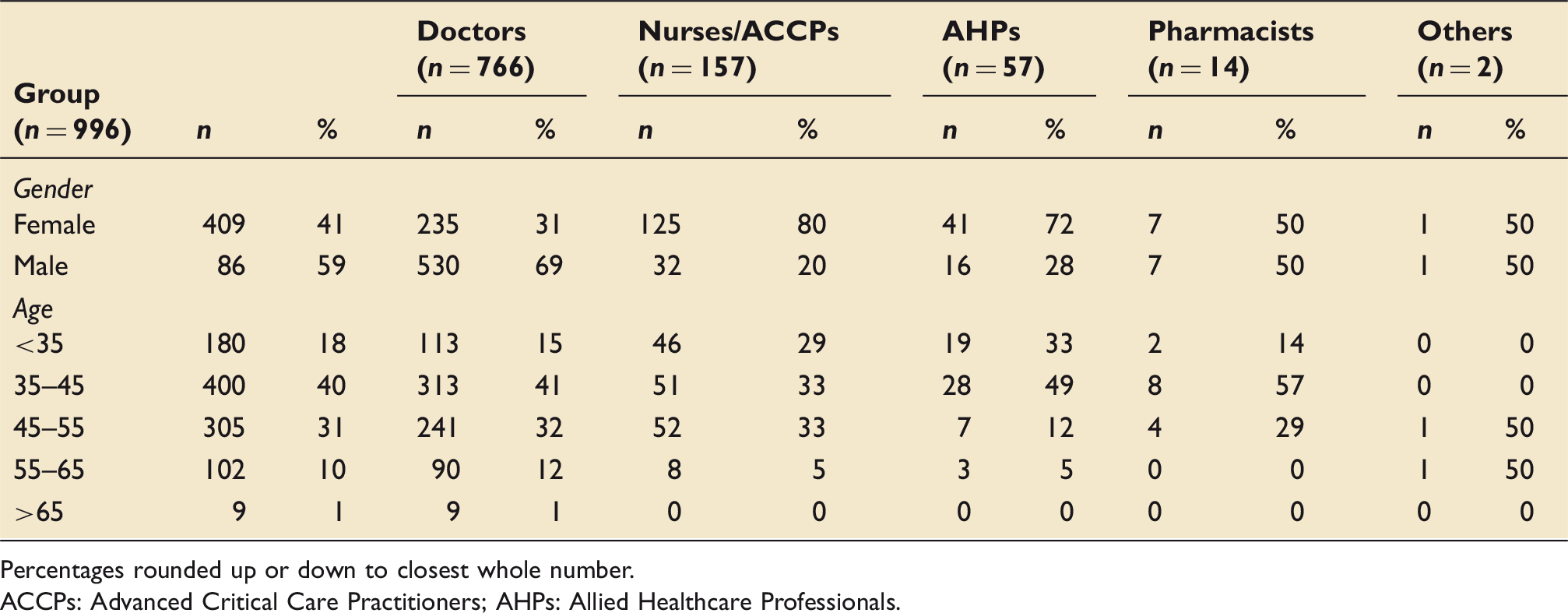
Percentages rounded up or down to closest whole number. ACCPs: Advanced Critical Care Practitioners; AHPs: Allied Healthcare Professionals.
Median scores for each domain of BOS according to gender.

Significance values are shown in bold.
Median scores for each domain of BOS according to professional group.
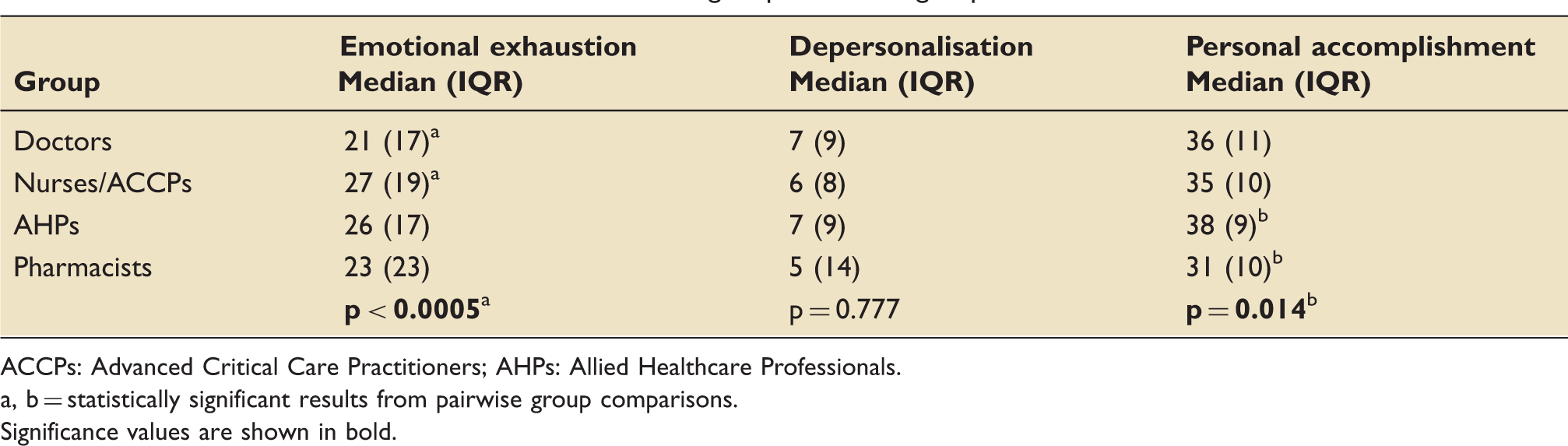
ACCPs: Advanced Critical Care Practitioners; AHPs: Allied Healthcare Professionals.
a, b = statistically significant results from pairwise group comparisons. Significance values are shown in bold.
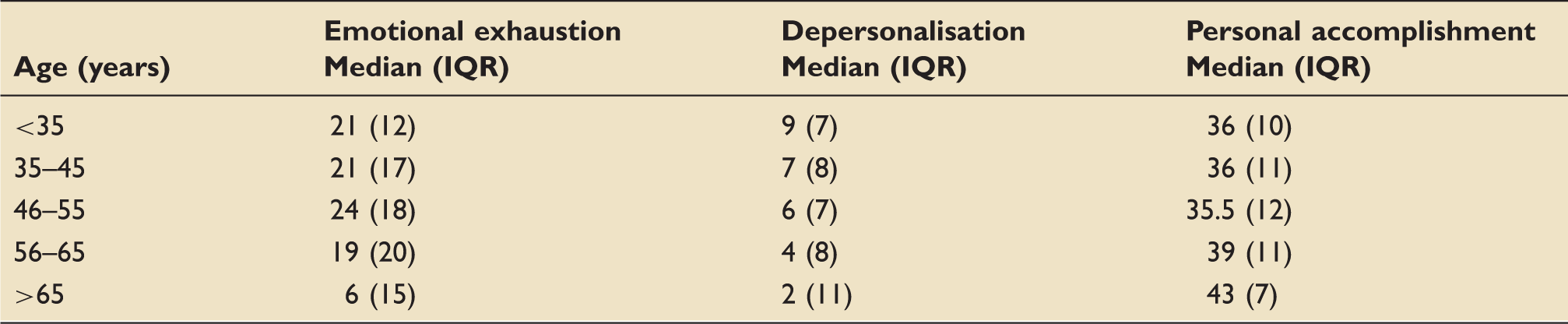
Median scores for each domain of burnout according to age.
Proportion of participants in ‘High Risk’ bracket for each domain of Burnout Syndrome according to gender, professional group and age (rounded to closest %).
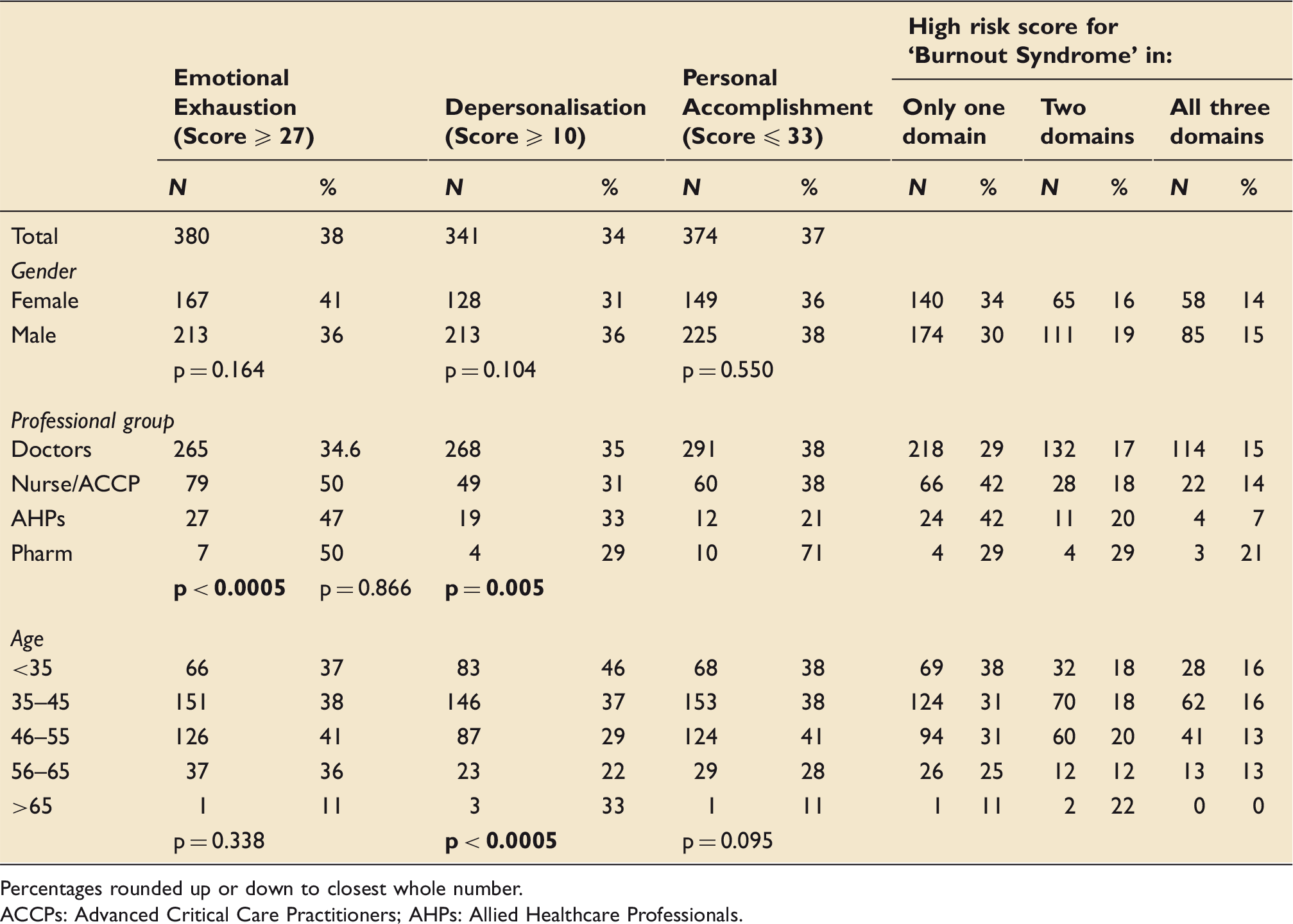
Percentages rounded up or down to closest whole number. ACCPs: Advanced Critical Care Practitioners; AHPs: Allied Healthcare Professionals.
Table 5 summarises the proportion of participants in the ‘high-risk’ bracket for each domain of BOS according to gender, professional group and age, as described above. More than one-third of the total cohort was in the high-risk bracket for at least one of the three BOS domains. Table 5 also lists the proportion of people in each gender group, professional group or age group who are in the high-risk bracket for one domain, any two domains or all three domains. Fourteen percentage of both male and female respondents were in the high-risk bracket for all three domains. There was a higher proportion of women than men in the high-risk group for just one domain, whereas the number of men in the high-risk bracket for any two domains was higher than for women. When grouped by profession, 21% pharmacists were in the high-risk group for all three domains, compared to 15% doctors, 14% nurses and 7% other AHPs. A similar pattern was seen for the proportion of respondents in the high-risk bracket for two domains, which was also highest in pharmacists. About 42% nurses and AHPs were in the high-risk bracket for just one domain, compared to 29% doctors and pharmacists. With respect to age brackets, a greater proportion of respondents in the < 35 and 35–45-year age groups were in the high-risk bracket for all three domains than in the other age groups. The proportion of respondents in the high-risk group for two domains was similarly distributed across the age groups. For those in the high-risk bracket for just one domain, there was a notably higher proportion of respondents in the < 35-year group than in other age groups.
Linear regression analysis examined the influence of age, gender and professional group for the three BOS domains. Depersonalisation score was positively associated with male gender (p < 0.0005). Depersonalisation score was negatively associated with increasing age and being a nurse (p < 0.0005 for both), i.e. older age and being a nurse rather than a doctor were associated with less negative or cynical feelings towards patients and colleagues.
Emotional Exhaustion score was positively associated with increasing age (p < 0.0005) (i.e. older practitioners were more likely to feel emotionally exhausted) and being a nurse, AHP or pharmacist compared to being a doctor (p < 0.0005, p = 0.003 and p = 0.05, respectively). Emotional Exhaustion score was negatively associated with male gender (p = 0.031).
Depersonalisation and Emotional Exhaustion scores were strongly positively associated (p < 0.0005) and were both strongly inversely associated with Personal Accomplishment (p < 0.0005) (i.e. suffering from Emotional Exhaustion or Depersonalisation is associated with a lower sense of accomplishment).
Discussion
Despite limitations (outlined below), our study provides substantial objective data regarding the risk of ICU BOS and how it manifests across domain, gender, profession and age group. We have shown that over a third of UK ICU HCPs are in the high-risk bracket for Emotional Exhaustion (38%), Depersonalisation (34%) and Personal Accomplishment (37%). Our data demonstrate risk across the whole MDT, including doctors, nurses, AHPs and pharmacists.
Whilst cautious about over-generalisation, the gender differences are intriguing. Our conclusion is not that one gender suffers more; but rather, by interrogating all three BOS domains, we offer a more personalised appreciation of workplace dissatisfaction. Understanding the range of emotions experienced by HCPs is particularly important as professions such as medicine and nursing transition away from male or female domination. There were significantly higher Emotional Exhaustion scores for females, along with more females in the high-risk group. In contrast, males had higher Depersonalisation scores and a higher proportion in the high-risk group for this domain. This reinforces the need to dissect what people mean when they report ‘burnout’. Furthermore, we should tailor support for ICU staff, rather than assume ‘one size fits all’.
Regarding the association between profession and BOS scores, our data offer similar opportunity for reflection and individualisation. Nurses had higher scores than doctors for Emotional Exhaustion, and more nurses scored ‘high-risk’. In contrast, while Depersonalisation was more associated with doctors than nurses, there was little separation between professional groups. Results for Personal Accomplishment were markedly different. It is important to emphasize that our study included only a small number of pharmacists (n = 14). However, their findings suggest that further focused study regarding this profession group could be warranted. While we caution against making sweeping assumptions from such a small cohort, the 14 pharmacists scored significantly lower (i.e. were higher risk) in the Personal Accomplishment domain, with twice the respondents in the high-risk group compared to doctors or nurses and three times more than AHPs. Regardless, these findings highlight the relative lack of attention given to HCPs other than doctors and nurses. Different findings from different specialties may be reflective of the different duties, exposures and hence, stressors of different ICU MDT members (such as nurses having 12-h constant contact with patients and their families) and the features of BOS that consequently predominate. Regardless, we owe it to all staff to provide individualised relevant support. What is helpful for one doctor or nurse may not be what another HCP needs.
Intensive Care Medicine was previously considered a young person’s pursuit, but is increasingly a life-long occupation. Accordingly, it is important to examine BOS across age groups. This even includes the relatively recent phenomenon of practitioners continuing to work in ICU beyond 65 years of age, albeit in numbers too small in our sample to generate meaningful conclusions. Regardless, we need to support HCPs throughout their career, and their concerns may differ as a function of age. Accordingly, we found a strong association between younger age and higher scores in the Depersonalisation domain, and as age increases, a decrease in the proportion of high-risk respondents. Broadly, we infer that BOS is experienced differently at different career stages and/or by different generations. Optimistically, this highlights that BOS can wax and wane: it needs not be final. Pessimistically, we are at continued risk. Regardless, the predominance of different BOS domains at different career stages may inform strategies that keep practitioners in the profession or ease their career transition.
Our study has limitations that reduce generalisability. These include its UK focus, inherent biases with self-reporting and surveys and difficulty quantifying emotional states. There are also myriad shortcomings with the MBI, which are expanded upon in a review article by Brindley et al. in this same journal edition. Speculatively, there might be under-reporting if there are concerns about anonymity, over-reporting if respondents are desperate to be heard or random inaccuracy if resentful about ‘another survey’. Although the MBI has good test–re-test reliability, because the survey represents ‘snap shot’ data, answers may be biased by recent experiences: fatigue, workload (both volume and emotional burden), distressing interpersonal interactions or one’s personal (rather than professional) life. The MBI is not a balanced emotional summary. Answers may even differ according to physical whereabouts during survey completion or enrollment. For example, some of our respondents filled out the MBI while at a conference or away from work (a presumably lower stress environment) whereas others would have done so in the midst of busy clinical days. The quantitative MBI also dictates a priori what can be reported, thereby missing the rich narrative of personal experience. It probes negative emotions rather than seeking evidence of joy, engagement or how HCPs find meaning from work. The MBI also does not capture resilience, i.e. one’s ability to protect against or recover from BOS. It may be the balance between risk factors for BOS and personal resilience that matters more.
The relative proportions of professional groups in our survey reflect the ICS membership but not the ICU workforce. Accordingly, if the entire workforce was surveyed, we would expect findings more representative of our nursing cohort. This should temper conclusions about the aggregated data, since a more representative sample would likely have scored higher for burnout if it included more nurses. Moreover, a majority of respondents were recruited via attendance at an annual meeting or voluntary membership of a society. Accordingly, this sample may be a particularly motivated and engaged group. If so, then our data may represent a best-case scenario and may be an underrepresentation of burnout in the wider profession.
There is also likely some collinearity between the three domains. Because the questionnaire was distributed electronically, there is the possibility that the sampled population was greater than intended (i.e. extending outside the UK Intensive Care Society membership). We also did not enquire whether staff work solely in adult ICU or include paediatric practice. As stated, there is no single score which defines ‘burnt out’ versus ‘not burnt out’. Instead, the sub-scale scores allow us to monitor the components of BOS over time and against others. Unfortunately, this makes it more difficult to compare our work against previous studies. It is also unclear what is an ‘acceptable’ BOS score in each domain. Furthermore, when considering the three BOS domains, there is no combination of scores from two or more domains which best diagnoses ‘burnout’, though this does appear to have association with other indices of psychological dysfunction. 18
There are aspects of working in Intensive Care Medicine, that are not ideal, and therefore BOS may be difficult to mitigate. Accordingly, we cannot always make things better. Patient numbers, patient age and patient complexity are increasing, alongside public (and professional) expectations. Regarding personality traits, as with all specialties, ICU HCPs self-select. Importantly, despite good intentions, we could also make things worse. This includes the idea of ‘burnout contagion’, 19 whereby influential members vocalise feelings and impressionable colleagues absorb and repeat these sentiments, but nothing useful is done. We strongly support the ‘call to action’, but believe data such as ours should encourage reflection and empathy at a personal and organisational level, alongside a culture of shared responsibility for all staff throughout their careers. A nuanced objective understanding of BOS is an important first step.
Footnotes
Acknowledgements
This study was undertaken on behalf of the UK Intensive Care Society Wellbeing Working Group: Peter Brindley, Daniele Bryden, Gareth Cornell, Jonathan Goodall, John Elmore, Julie Highfield, Richard Innes, Ganesh Suntharalingam, Linda-Jayne Mottram, Segun Olusanya, Steve Mathieu, Jamie Strachan, Laura Vincent, Dorothy Wade and Fiona Wallace.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.