
Abstract
Background
The relationship between postoperative intensive care (ICU) admission following emergency general surgery (EGS) and emergency hospital readmission has not been widely investigated.
Methods
Retrospective analysis of registry data for patients undergoing EGS in Scotland, 2005–2007. Exposure of interest was ICU admission status (direct from theatre; indirect after initial care on ward; no ICU admission). The primary outcome was emergency hospital readmission within 30 days of discharge.
Results
Thirty-seven thousand one hundred seventy-three patients were included in the analysis. Overall emergency readmission rate was 8% (n = 2983): 2756 (7.8%) in patients without postoperative ICU admission; 155 (12.1%) with direct ICU admission and 65 (14.7%) with indirect ICU admission. Indirect ICU admission was associated with increased hospital readmission rates (HR 1.24 [1.03, 1.49]; p = 0.024) compared with direct ICU admission. ICU admission was associated with increased three-year readmission rates (p = 0.006) and costs (p < 0.001) compared with initial ward care.
Conclusion
Indirect ICU admission is associated with increased emergency hospital readmission and healthcare costs for patients undergoing EGS.
Introduction
Hospital readmission following surgery is associated with increased long-term mortality, longer hospital length of stay (LOS), and significantly higher cost. An overall readmission rate of 13% following surgery has been quoted for Medicare recipients in the USA 1 ; however, this figure varies according to the nature of surgery, ranging from 5% after major joint arthroplasty, 2 10–15% following colorectal surgery1,3,4 to even higher rates for complex surgery such as pancreaticoduodenectomy 5 or vascular procedures. 1 Costs associated with readmission after surgery are substantial, estimated to cost Medicare in excess of half a billion US dollars each year. 1
The global volume of surgery is expanding and6,7 operative procedures are increasingly offered to patients who may not have previously been considered for surgery due to age or comorbidity. Postoperative complications and hospital readmission place a significant burden on patient quality of life and healthcare resources. Although the overall rate of death following elective surgery is low, 0.5% in recent global data, 8 post-operative complication rates of up to 10 times this figure have been reported 9 and these have been shown to influence long-term survival and quality of life. 10 Variation in the outcome of patients who suffer complications has been reported between hospitals, suggesting that differences in process of care may have a direct effect. 9
Patients undergoing high-risk surgery are often admitted to intensive care units (ICUs) postoperatively to allow the early detection or prevention of postoperative complications. This is considered an important standard of care for patients at highest risk of death and complications although admission patterns are variable and its benefit remains unproven. 8 Although health services research (HSR) suggests that emergency admission to ICU following a period of care on a standard ward is associated with increased mortality rates, 11 the impact of routine ICU admission after high risk surgery on complications and hospital readmission remains largely unknown with some studies suggesting that costs and LOS might be increased with little benefit in some groups. 12
Patients undergoing emergency general surgery (EGS) are a group at greater risk of death and complications. 13 Using high-quality data available for all patients treated in the National Health Service in Scotland, we undertook an observational study to investigate causes for hospital readmission in EGS patients and to explore risk factors associated with readmission and reoperation in this group, including planned and unplanned ICU utilisation. Our aims were as follows: to determine the association between ICU utilisation and hospital readmissions, in particular to determine if indirect ICU admission was associated with increased incidence of subsequent hospital readmission compared with direct ICU admission; to determine the effect of ICU admission on costs associated with unplanned hospital readmission following EGS in the three years following the index procedure.
Methods
Ethics, sponsorship, and indemnity
The Chair of South East Scotland Research Ethics Committees reviewed the study and waived requirement for a full ethics submission. Instead the study underwent review by Information Services Division’s Privacy Advisory Committee, which undertakes the role of Caldicott guardianship (Reference PAC 58/11).
Patient involvement
Patients were not involved directly with the design or conduct of this study; however, a recent joint National Institute of Academic Anaesthesia and James Lind Alliance research priority setting exercise identified improvement of emergency surgical care as one of the top 10 research questions. 14
Study population
A cohort study design was used. An analysis plan was developed a priori. We extracted a complete record of surgical inpatients managed in Scotland between 1 January 2005 and 31 December 2007 from the Information Services Division (ISD) of NHS Scotland Scottish Morbidity Record (SMR01) database. The data from ISD Scotland provided complete details of hospital and ICU admissions in Scotland. Data linkage is undertaken centrally using probabilistic matching methods. The fields used to undertake linkage include name, sex, date of birth, post code, date of death, and unique patient identifying numbers such as the Community Health Index number (a unique health care identifier in Scotland allocated to all Scottish residents). A computer algorithm is used to compare each field between two records and generate a score. This score depends on the agreement of the contents of the field and the rarity of the information. From this, the probability that the two records relate to the same person is calculated. This probability is the sum of weighted scores for each field. Records are only considered correct matches if the sum of the weighted scores is greater than a specified threshold value. Manual validation of linkages indicates that the accuracy of this method of data linkage is high. A detailed description of how this cohort was identified and data on the effect of ICU utilization on short and long-term mortality after elective and non-elective surgery have been published elsewhere 11 and a full description of the process is available in the electronic supplementary material (ESM). This cohort was restricted to adult patients undergoing inpatient non-elective general surgery. The Operating Procedure Coding System-4.2 (OPCS) was used to identify general surgical procedures and International Classification of Diseases, 10th Edition (ICD-10) system to determine causes for hospital readmission. General surgery was defined as abdominal or gastrointestinal procedures, or procedures on breast, endocrine or soft tissue. A description of the codes used is also described in the ESM.
We included only the general surgical patients undergoing non-elective surgery who survived to discharge from hospital after the index procedure. This was because only patients who were discharged from hospital could be at risk of subsequent hospital readmission. All other surgical groups were excluded, as well as any patients with diagnostic, non-surgical or missing codes. For patients with more than one included surgical procedure during the three-year study period, we used only the first surgical procedure.
Variables
For each patient, a full data extract was requested, including: age; gender; socio-economic status; surgical OPCS code; International Classification of Diseases, 10th Edition (ICD-10) code; surgical status (elective vs emergency classification); date of index hospital discharge; and number of hospital admissions in the five years before index admission. ICD-10 codes were used to define diagnosis (malignant, trauma/injury, other). In addition, we reported a measure of co-morbidity using a count of co-morbidities that constitute the Charlson co-morbidity index, a measure of co-morbidity derived from 17 chronic conditions. 15 Socio-economic status was assigned using quintiles of the Scottish Index of Multiple Deprivation (SIMD), which is based on area of residence and comprises multiple domains of differentially weighted measures of deprivation, including income, employment, education, crime, and housing. 16 Operative complexity was assigned to each procedure using the classification described in ‘BUPA Schedule of Procedures’. 17 Season was defined by admission date (December to February, March to May, June to August, and September to November). Date of discharge was defined as a binary variable (Monday to Thursday vs. Friday to Sunday).
We ascertained admission to an ICU by linkage to the Scottish Intensive Care Society Audit Group (SICSAG) database. Patients were classified by the main exposure variable as follows: those not admitted to ICU during the first seven days after surgery (‘no ICU admission’); those whose ICU admission occurred immediately after surgery (i.e. transferred directly from theatre or recovery room to ICU, ‘direct ICU admission’); and those who were transferred directly from theatre or recovery room to a non-ICU environment but subsequently admitted to the ICU during the first seven days after surgery (‘indirect ICU admission’). We selected a seven-day period after operation to increase the likelihood that the event precipitating ICU admission was related to post-operative complications. The small number of patients operated on during their ICU stay was recoded as missing for analyses. “Direct ICU admission” was the reference category.
Outcome measures
The primary outcome measure was emergency hospital readmission within 30 days of index hospital discharge. This was identified as a non-elective hospital admission in the SMR01 record. Secondary outcomes were: re-operation within 30 days of index hospital discharge (defined as OPCS code indicating surgical procedure during an emergency hospital readmission); readmission with complication (grouped into broad themes by ICD-10 code, see online data supplement for details); rate of emergency readmission in the three years following discharge after the index procedure, and costs in the three years following discharge after the index procedure. Per diem costs for hospital care were derived from the NHS Scottish Costs Book 2016/7. 18
Statistical analysis
Data were summarised as mean (standard deviation, SD), median (interquartile range, IQR) or number (%). Univariable analyses were carried out to test the association of baseline characteristics and outcomes with ICU admission status using χ2 and Mann–Whitney U tests.
A complete case analysis was undertaken. Patient demographics, rate and cause of readmission were reported. Factors associated with outcomes and confounder-adjusted associations of ICU status with outcomes were identified using univariable and multivariable competing risks regression (Fine and Gray) models for 30-day outcomes and negative binomial regression models for three-year readmission rates. Fine and Gray models allow for the competing risk of death by modelling an estimate of cumulative incidence of first emergency hospital admission with early deaths remaining in the denominator. Exponentiated regression coefficients can be interpreted as subdistribution hazard ratios (HRs). Negative binomial multivariable regression models total number of emergency hospital admissions during the three-year follow-up period as the dependent variable. Coefficients produced from this regression model—once exponentiated—can be interpreted as an admission rate ratio. Clustering by health board health board administrative region in which the operation was performed (hospital or group of hospitals which provide health services to a geographical area) was accommodated by using robust cluster variance estimators for standard errors for regression coefficients and modelling health board as a fixed effect.
All analyses were undertaken using Stata 13 (StataCorp, College Station, TX, USA) and R (R Foundation, Vienna, Austria). The study was reported using the “Strengthening reporting in observational studies in epidemiology (STROBE)” methodology. 19
Results
Study cohort characteristics
The selection process for the final study cohort is outlined in Figure 1. The initial cohort included 1014,796 patients who had undergone surgery during the study period, with the exclusion of cardiac surgery, neurosurgery, obstetrics, transplantation and the surgical management of burns. Following exclusion of records relating to: second or subsequent admissions, patients aged under 16 years, patients with non-surgical or diagnostic procedural codes, patients with discordant operative or death dates or patients who died during the hospital admission related to the index procedure, 567,293 patients remained. Following further restriction to patients having emergency “general” surgical procedures, 37,173 patients remained in the final cohort. Records and dates of death ranged from 3 January 2005 to 30 September 2012. Three-year follow-up was available for all patients.
Study cohort derivation.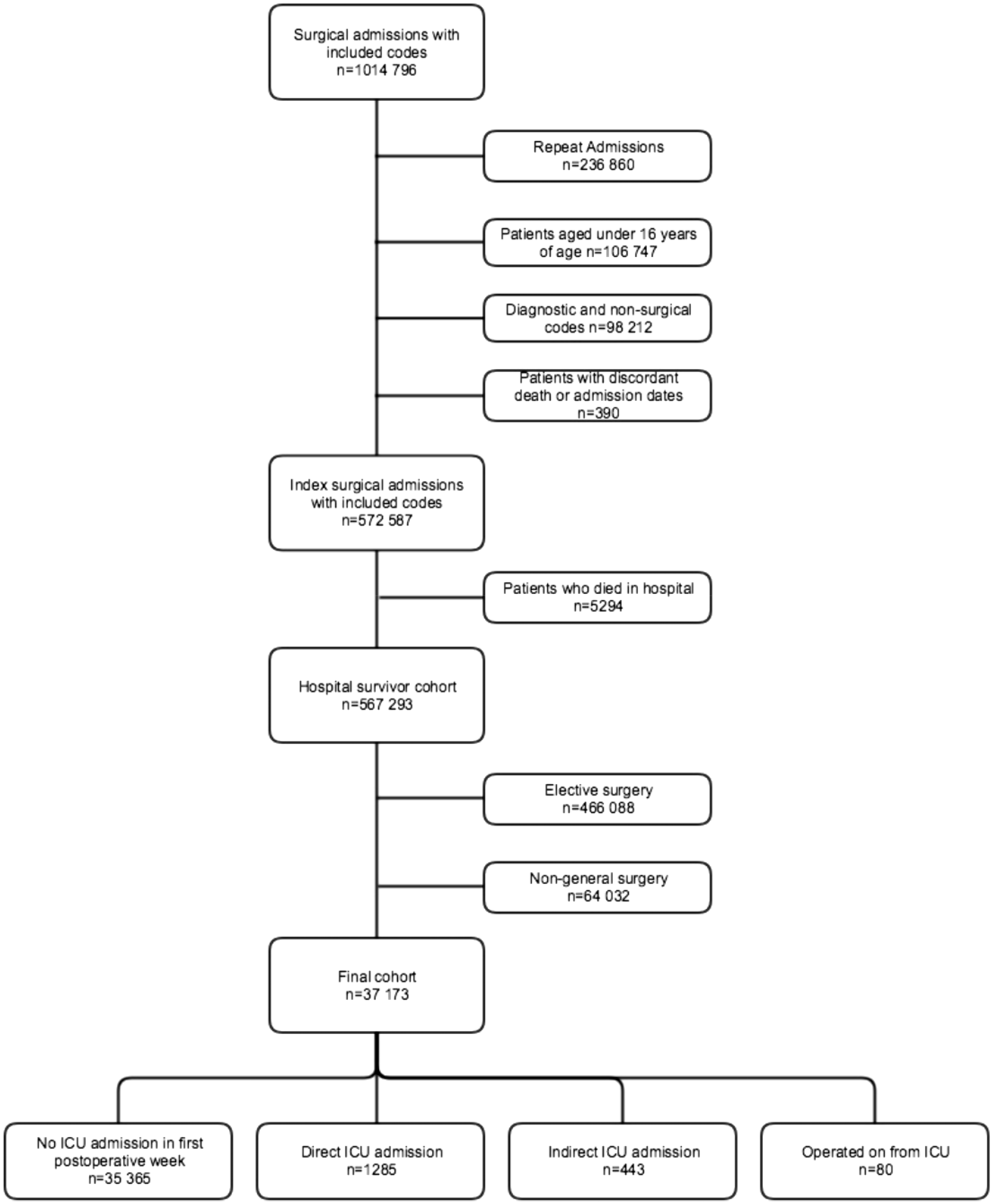
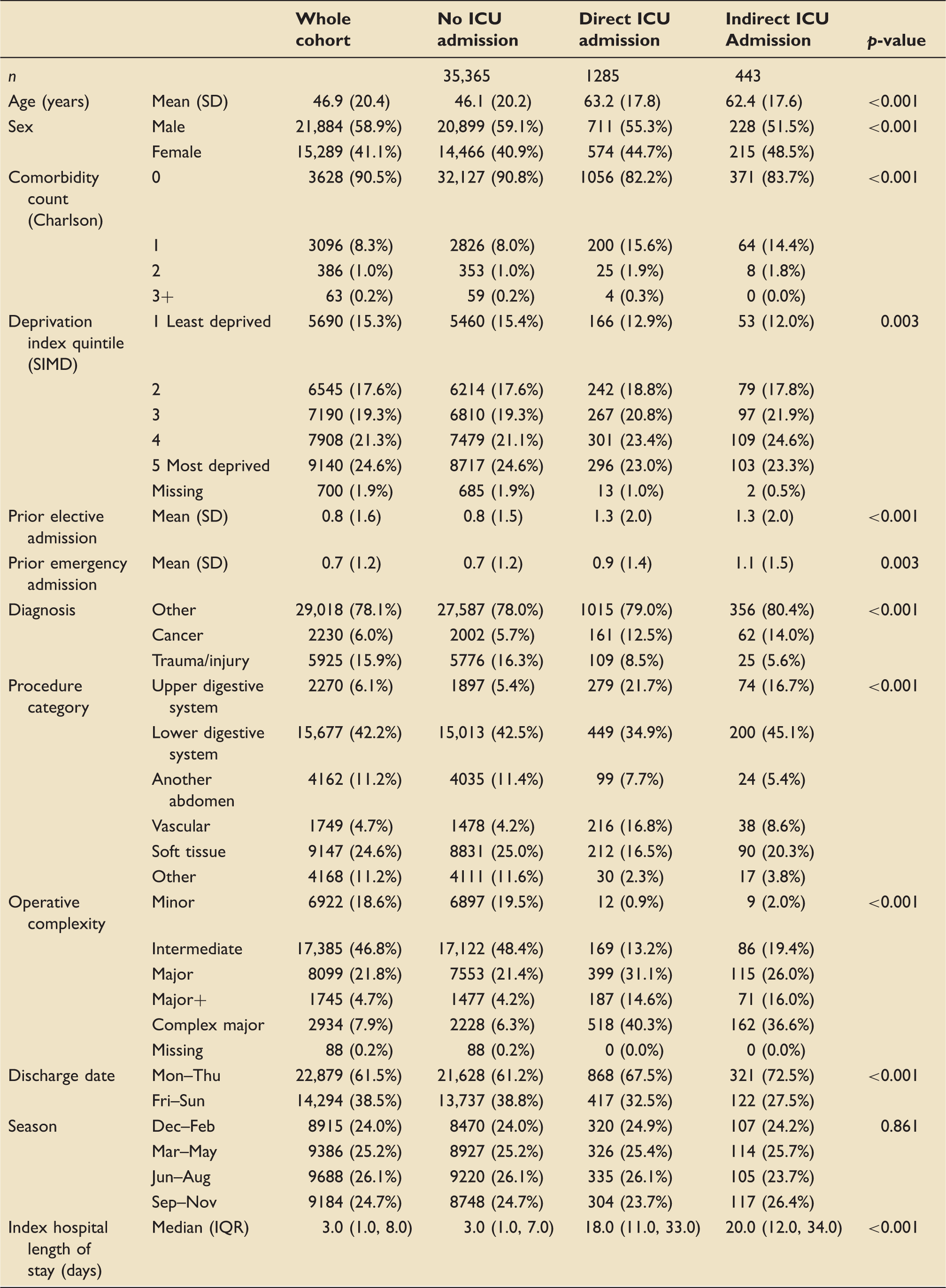
Demographic details of study cohort.
Rate and cause of readmission
Outcome data for study cohort.

Leading causes of 30-day readmission with complications were surgical complications (e.g. wound infection, haematoma) (43.2%), gastrointestinal complications (17.1%) and cardiovascular complications (10.8%) (Table 2). Patients who were admitted to ICU postoperatively had higher rates of readmission for infectious, thromboembolic and respiratory complications (p = 0.006). The overall rate of readmission with reoperation was 2.8% and this increased in patients directly and indirectly admitted to ICU to rates of 4.2% and 3.6%, respectively (p < 0.001).
ICU admission status was associated with three-year emergency readmission rates (p < 0.001) (Table 2). In patients not admitted to ICU following surgery, the crude incidence rate of emergency readmission over three years (per person per year) was 0.29 (95% confidence interval [CI] 0.29, 0.30) compared with 0.53 (CI 0.51, 0.56) for those admitted directly to ICU and 0.55 (CI 0.51, 0.60) for those indirectly admitted to ICU. Healthcare costs of emergency readmission over the 3 years following the index admission were similarly associated with ICU admission status (p < 0.001) (Table 2). Mean per patient cost (95%CI) was lowest for those not admitted to ICU (£4649 (4471, 4828)) compared with £9976 (8829, 11,123) for those directly admitted to ICU and £11,082 (9060, 13,105) for those admitted indirectly.
Primary outcome
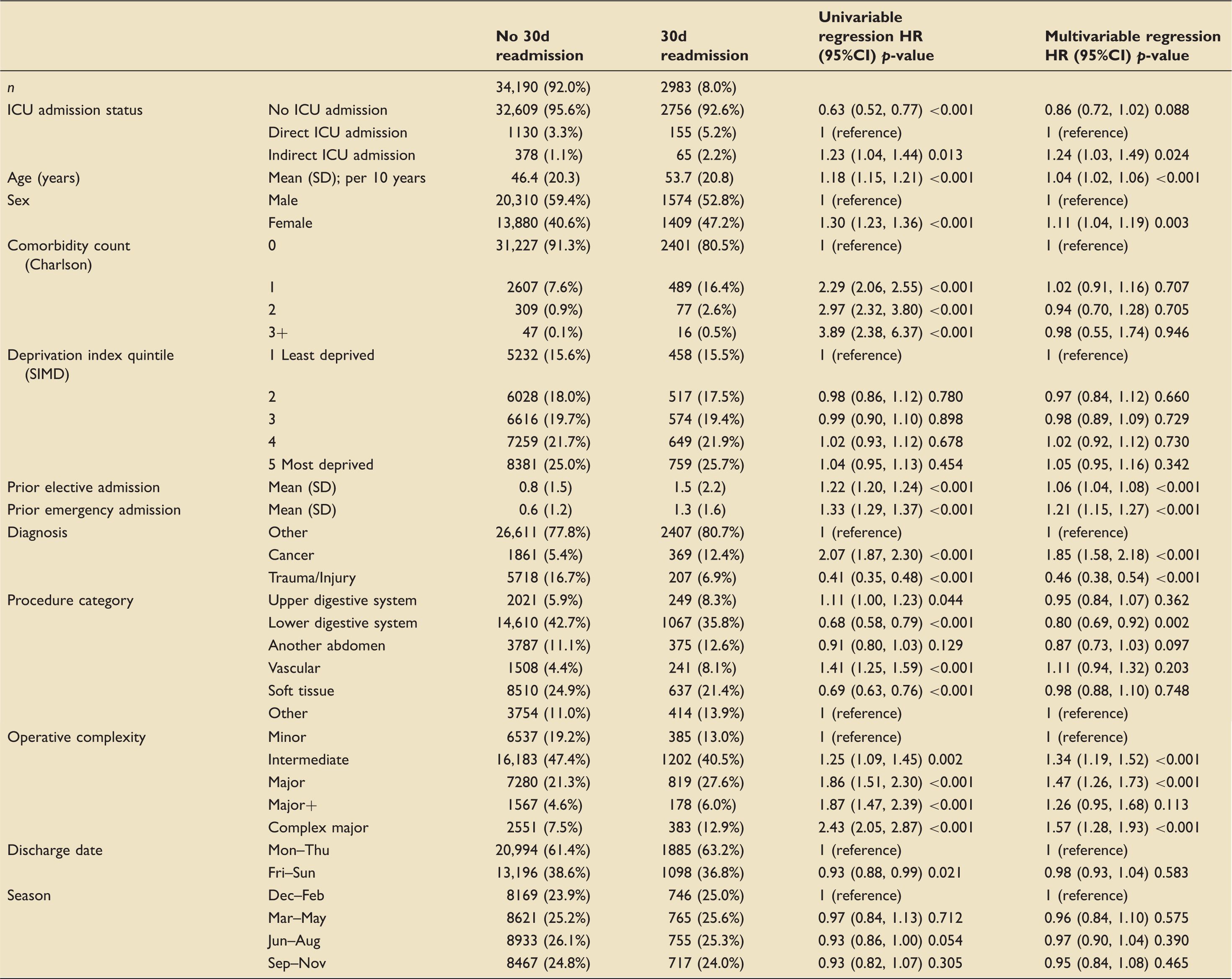
Factors associated with 30-day emergency readmission.
Secondary outcomes
When the analysis was repeated for reoperation within 30 days, indirect ICU admission was not associated with increased reoperation rate, compared with direct admission to ICU (HR 0.85 [95% CI 0.57, 1.28] p = 0.445) (Supplementary Table 2). No ICU admission was associated with a reduced reoperation rate compared with direct ICU admission (HR 0.75 [95% CI 0.58, 0.96] p = 0.025).
Compared with direct ICU admission, indirect ICU admission was associated with increased readmission with a medical complication (HR 1.38 [95% CI 1.04, 1.83], p = 0.026) (Supplementary Table 3) but not overall three-year readmission rate (HR 1.05 [95% CI 0.80, 1.24], p = 0.530) (Supplementary Table 4). No ICU admission was associated with a reduction in both readmission with medical complication (HR 0.78 [95% CI 0.66, 0.92], p = 0.003) and three-year readmission rate: HR 0.83 [95% CI 0.73, 095], p = 0.006).
Discussion
The principal finding of this study was that for patients undergoing EGS, indirect ICU admission (i.e. ICU admission after initial care on a standard ward) was associated with an increased rate and duration of emergency hospital readmission even after controlling for potential confounders. Indirect admission to ICU was associated with increased readmission with medical complications, rather than readmission with reoperation. Risk factors for readmission within 30 days of hospital discharge in this cohort included surgical complexity, surgery on the lower digestive system, admission diagnosis of trauma or malignancy and previous hospital admission. Healthcare costs and three-year readmission rate were increased for patients admitted directly to ICU when compared to no ICU admission but this was not increased for indirect ICU admission.
Emergency hospital readmission following surgery is associated with increased long-term morbidity and mortality, healthcare resource use and cost. 10 As yet few studies have examined patterns of ICU use on post discharge complications or emergency hospital readmission (the rates of which are much higher than death) or longer term costs following surgery. Many studies have identified operative and infectious complications as being the commonest reasons for readmission, in particular surgical site infections (SSI) and pneumonia; however, thromboembolic, cardiac and renal complications also feature prominently, in common with our findings.20–22 We found that some patient-level risk factors were also associated with readmission following surgery and these included: increased age, presence and degree of co-morbidity, socioeconomic status, type and duration of surgery and presence of malignant disease.20,23
In this cohort, indirect ICU admission was associated with increased emergency hospital readmission with medical complications, particularly infectious, thromboembolic and respiratory complications. In these patients, indirect ICU admission may represent the occurrence of a serious and unexpected postoperative complication, of which the longer term detriment to patients has been well described. Several studies have identified postoperative complications occurring prior to hospital discharge as the strongest predictor of emergency hospital readmission.20,23,24
Complication rates and the proportion of patients who die from postoperative complications, known as the failure to rescue [FtR] rate, are being used increasingly as metrics to guide HSR and quality improvement; however, postoperative complications are not reliably captured using administrative data such as ours. Indirect ICU admission has been strongly associated with mortality in previous studies.11,25 and in this study, it is strongly linked with emergency hospital readmission. FtR is difficult to measure in administrative data, particularly in the UK where there detailed data on postoperative complications prior to hospital discharge are not reliably collected. However, reoperation, indirect or unplanned ICU admission following surgery and death are more easily identified from administrative data and correspond with Clavien-Dindo classification grades III–V. 26 Thus, they could be used as an estimate of life-threatening postoperative complications following surgery and as a surrogate or modified FtR in this setting.
The association between indirect ICU admission and mortality is often used to justify elective ICU admission after high-risk surgery, in order to allow early detection and treatment of major complications. However, some studies and commentators have suggested routine ICU admission after certain elective major surgical procedures may increase costs and LOS without improvement in survival.11,12,27,28 As yet few studies have examined patterns of ICU use on post discharge complications or emergency hospital readmission (the rates of which are much higher than death) or longer term costs following surgery.
This study has several strengths. Firstly, to our knowledge, this study is the first direct-linkage cohort study to assess the association between ICU admission and post discharge readmission and reoperation after high-risk surgery at a national level. Secondly, we have studied a cohort of patients undergoing EGS, known to be at high risk of postoperative complications. Finally, ISD data are of high quality with linkage to ICU registry and low rates of missing data. Limitations are common to other HSR using administrative data: the possibility of bias and residual confounding cannot be excluded. Only first admissions in the three-year period were included to allow long-term follow-up. The cohort is relatively dated, with follow-up ending in 2012; however, this was in part necessary to allow long-term follow-up for all patients. As readmissions are often sicker and have more comorbidities, and a small number of these patients may die shortly after discharge, selection bias is possible. Despite extensive adjustment for known confounders, patients admitted to ICU have an increased risk of death and complication which likely represents residual confounding, and this has been described in other similar investigations. 12 We were unable to reliably identify patients admitted to high-dependency units in our data extract. Finally, bed availability and increased risk identified by the treating clinician are not reliably captured in data such as ours.
In conclusion, our study demonstrates that indirect ICU admission is associated with increased rate of 30-day emergency hospital readmission and this was more likely to be for medical, non-operative reasons in patients undergoing EGS. Compared with patients who did not require ICU care, direct ICU admission was not associated with reduced rate of 30-day emergency hospital readmission rate but was associated with increased cost over the three years after the index procedure. Further work is required to reliably capture the incidence and severity of postoperative complications in administrative data and whether this can be replicated with more contemporaneous data. Future studies should define the groups most likely to benefit from postoperative admission to critical care, and to identify robust mechanisms for identifying those at risk postoperative complications.
Authors’ contributions
Conceived the project and secured the funding: MAG, NIL, TSW, RWP, RMP. Study design, interpretation of results and preparation of the manuscript: all authors. MAG, NIL, CH, LS, SG, EMH. designed and performed the data extraction, cleaned and recoded the data, and performed aspects of the analysis. Overall responsibility for the integrity of the manuscript: MAG, NIL.
Supplemental Material
Supplemental material for The association between ICU admission and emergency hospital readmission following emergency general surgery
Supplemental Material for The association between ICU admission and emergency hospital readmission following emergency general surgery by Michael A Gillies, Sadia Ghaffar, Ewen Harrison, Catriona Haddow, Lorraine Smyth, Timothy S Walsh, Rupert M Pearse and Nazir I Lone in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MAG is a Chief Scientist’s Office (CSO) NHS Research Scheme Clinician. RMP lectures and performed consultancy work for Nestle Health Sciences, Medtronic, Edwards Lifesciences, and Massimo Inc. All other authors report no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Chief Scientist’s Office Scotland (grant no. CHZ/821/4).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.