
Abstract
Introduction
Across the United Kingdom, physiotherapy for critical care patients is provided 24 h a day, 7 days per week. There is a national drive to standardise the knowledge and skills of physiotherapists which will support training and reduce variability in clinical practice.
Methods
A modified Delphi technique using a questionnaire was used. The questionnaire, originally containing 214 items, was completed over three rounds. Items with no consensus were included in later rounds along with any additional items suggested.
Results
In all, 114 physiotherapists from across the United Kingdom participated in the first round, with 102 and 92 completing rounds 2 and 3, respectively. In total, 224 items were included: 107 were deemed essential as a minimum standard of clinical practice; 83 were not essential and consensus was not reached for 34 items.
Analysis/Conclusion
This study identified 107 items of knowledge and skills that are essential as a minimum standard for clinical practice by physiotherapists working in United Kingdom critical care units.
Introduction
The National Guidelines for the Provision of Intensive Care Services 1 identify physiotherapy as one of the principle and most consistent therapy services for Critical Care. Traditionally, the aim of physiotherapy was to maintain bronchial hygiene for people who are intubated, 2 and while this remains a key area, the focus is now towards early rehabilitation and on physical recovery.3,4
In most hospitals across the United Kingdom (UK), physiotherapy for critical care patients is provided 24 h a day, 7 days per week 1 and is achieved through the provision of out-of-hours or on-call services and weekend working. A recent on-call position statement 5 recognised that to achieve this cover, the service often relies on non-respiratory specialists of varying clinical grade and experience.5–7 Frequently, staff will not have worked within critical care since qualification, and increasingly staff may have not gained any entry-level experiences within critical care. As a result, the quality of the service provided to the patient may become dependent on the skills of the treating physiotherapist and thus clinical assessment, interventions and management may vary significantly in quality or effectiveness. 8
To overcome the challenges of non-respiratory specialists working in critical care to provide 24-h cover, physiotherapists are required to complete in-house/local critical care orientation programs with varying content. Such training may include theory, clinical skills training, and supervised clinical practices although the exact content has not been researched or analysed. Any such programs are commonly delivered and assessed by senior physiotherapy staff; thus, the process is often subjective and informal with variability in the content, requirements, and duration of the education provided.5,8
Based on the above, there is a national5,9 and international8,10 drive to standardise the expected knowledge and skills of physiotherapists assessing and treating patients within the critical care environment. Skinner et al. 8 used a modified Delphi approach to investigate the minimum standards of clinical practice for physiotherapists working in critical care settings in Australia and New Zealand. The study involved a panel of 50 senior or specialist critical care physiotherapists and appropriate academic staff completing three rounds of questionnaires exploring the knowledge and skills required. Items were designated by participants as being ‘Essential/Unsure/Not Essential’. Consensus for inclusion was achieved when items were ranked ‘Essential’ by more than 70% of participants. Consensus was reached on 199 (89%) items. The panel agreed that 132 (58%) items were ‘Essential’ items for inclusion in the final framework. Following its completion, the authors aimed to explore the utility of the framework and how it may be used within clinical education and practice to standardise patient assessment and care, and reduce the current variations. However, this further exploration of the framework is not yet available or published.
More recently, van Aswegen and colleagues 10 explored the minimum standards for physiotherapy in South African ICUs. The study adopted a different approach to that of Skinner et al., 8 and completed three focus group sessions with 25 purposively sampled experienced clinicians (average 10.8 years critical care experience). Rather than determining essential and non-essential characteristics, the results focused around key themes of practice with the aim of answering the fundamental question: ‘What is the minimum standard of clinical practice needed by physiotherapists to ensure safe and independent practice in South African ICUs’. Three themes were identified: (1) Integrated Medical Knowledge, which included sub-themes of anatomy and physiology, presenting conditions, ICU environment, pathophysiology; (2) Multi-disciplinary teamwork, including communication, documentation, ethics, and culture sensitivity; and (3) Physiotherapy practice, which included clinical reasoning, handling skills, and patient care. Despite the variation in methodology to the Australasian study, 8 the conclusions are similar. Both the South African and Australasian studies recognise the need to develop consensus agreement and national standards, and determine their role within clinical practice.
Due to anecdotal international differences in entry-level training (e.g. entry-level curriculum, length of training), clinical experience, and potential physiotherapy roles (e.g. clinical responsibility, job descriptions and roles), it is not possible to generalise international findings within UK practice.
Furthermore, changing demands on oncall services, 5 reductions in workforce capacity, 5 variability in staff entry-level and postgraduate experiences, 9 and perceptions of variability in clinical practice mean that it is necessary to explore the minimum standard of clinical practice for physiotherapists in critical care units across the UK. These minimum standards can then be used to inform entry-level and postgraduate training, support on-call services and standardise the delivery of physiotherapy to critical care patients.
Method
Ethics
Ethical approval was provided by Cardiff University School of Healthcare Science Research Ethics Committee. An information sheet was provided to potential participants and informed consent was assumed by completion of the questionnaires in each round.
Design
A modified Delphi technique was used to obtain a consensus on the minimum standards of physiotherapy clinical practice in critical care units in the UK. The Delphi technique was chosen as it allowed participants from across the UK to participate and could be completed using online surveys making it more accessible.11–14 Additionally, the Delphi technique allows formation of consensus or the exploration of a field beyond existing knowledge.11–14 It can be tailored to the particular requirements of the research question, ranging from open and exploratory questioning to standardised confirmatory approaches. 15 The standard Dephi technique was modified to allow question refinement, addition of new items and ultimate endorsement of the items by the panel of experts.
Participants
Potential participants were recruited via advertisement of the study using existing networks such as the Association of Chartered Physiotherapists in Respiratory Care, UK Physiotherapy Respiratory Leaders Network, Intensive Care Society Nurse and Allied Health Professionals, Critical Care Nurse Lead Network, and the All Wales Physiotherapy Critical Care Network. Posts were also provided via social media and Interactive Chartered Society of Physiotherapy.
A predetermined sample size was not chosen, to allow as many physiotherapists to be involved as possible. The inclusion criteria were (1) experienced critical care physiotherapists with at least 5 years postgraduate experience of which at least 3 years have been in a senior role within critical care and (2) involved in supervision or teaching of physiotherapy staff working oncall or completing emergency duty. Additionally, academic physiotherapy staff involved in the provision of entry-level cardio-respiratory physiotherapy were recruited. An eligibility questionnaire was utilised to allow these data to be collected.
An essential component of the Delphi approach was provision of personalised reports to enable participants to compare their answers with the consensus opinions. 13 As a result, those participants that wished to remain anonymous or did not provide sufficient personal and contact details were excluded from the study. 16
Questionnaire development
The questionnaire used within this study was based on the one piloted and used by Skinner et al. 8 The Australasian questionnaire 8 was designed and intended to be as expansive as possible across the physiotherapy role in critical care, and utilised existing empirical resources, available critical care competency lists, and existing entry-level course materials. Prior to utilisation in this UK study, minor modifications were made to ensure relevance with the UK. The minor alterations consisted solely of alterations of language (e.g. intercostal catheter altered to intercostal drain). The amendments were discussed and approved by Skinner and colleagues. 8 No formal piloting was completed because of its previous usage.
The questionnaire emphasized that the objective was to determine the minimum standard of clinical practice that should be expected from physiotherapists to enable them to work independently and safely with patients in UK critical care settings. This minimum standard must be for all staff no matter of individual’s primary specialist area (e.g. respiratory or non-respiratory specialist) and pre-existing critical care experience, or the specialism of the critical care unit.
For each questionnaire item, participants were asked to either answer as ‘essential for clinical practice’, ‘not essential for clinical practice’, or ‘unsure’. The questionnaire also allowed for comments and in rounds 1 and 2 participants were invited to submit potential additional items that they deemed essential for clinical practice but not previously included.
Procedure
Three rounds of questionnaires were administered to participants who were given up to 4 weeks to complete 13 each phase. Questionnaires were disseminated electronically via Bristol Online Surveys (Bristol University, UK). The participant information sheet was included in the invitation email. Electronic reminders to submit were issued to non-responders and set time periods (2 weeks and 3 weeks), alongside regular prompting via social media.
At the end of each round, each participant was sent a personalized report containing quantitative group results, qualitative feedback, and the participant’s own responses for comparison purposes.
Analysis
Demographic data were collected in round 1 only. All data analysis was descriptive and open comments were themed for purposes of the personalised report. All data were exported from Bristol Online Survey (Bristol University, UK) and data analysed using Microsoft Excel™.
Items were determined as essential or not essential based on consensus option of >70% (essential or not essential accordingly). The 70% threshold was chosen to correlate with previous research, 8 allowing later comparison of findings. Additionally, items were excluded from future rounds when less than 30% of respondents felt the item was essential for clinical practice.
To ensure that final consensus was not biased by ‘unsure’ responses, consensus was calculated using three potential denominators. For example, consensus of 70% was required when considering (1) total number responses (e.g. the total number of participants completing the survey) including missing answers; (2) total number of responses excluding missing answers; and (3) total number of definitive essential and not essential responses (excludes ‘unsure’ responses). To be included as essential or not essential, 70% consensus was required for all three calculations.
Comments received throughout each round were themed based on response. For all items the comments were themed by one investigator and checked for accuracy by at least one of the other investigators.
Results
The eligibility questionnaire was completed by 197 physiotherapists, with 142 being invited to participate in round 1. Of these, 114 completed round 1 (80%) with 92 participants completing all three rounds (65%) (see Figure 1). Participants (n = 114) represented all UK nations (England (96), Wales (8), Scotland (7), Northern Ireland (1) and Jersey (1)), and had an average of 16.6 years postgraduate experience, of which 15.0 years was in a senior critical care role. All participants (except the ten England and one Wales based academics) were working in a Physiotherapy Team Lead role or above, with 54.9% having postgraduate training at Masters level or above.
Participant involvement.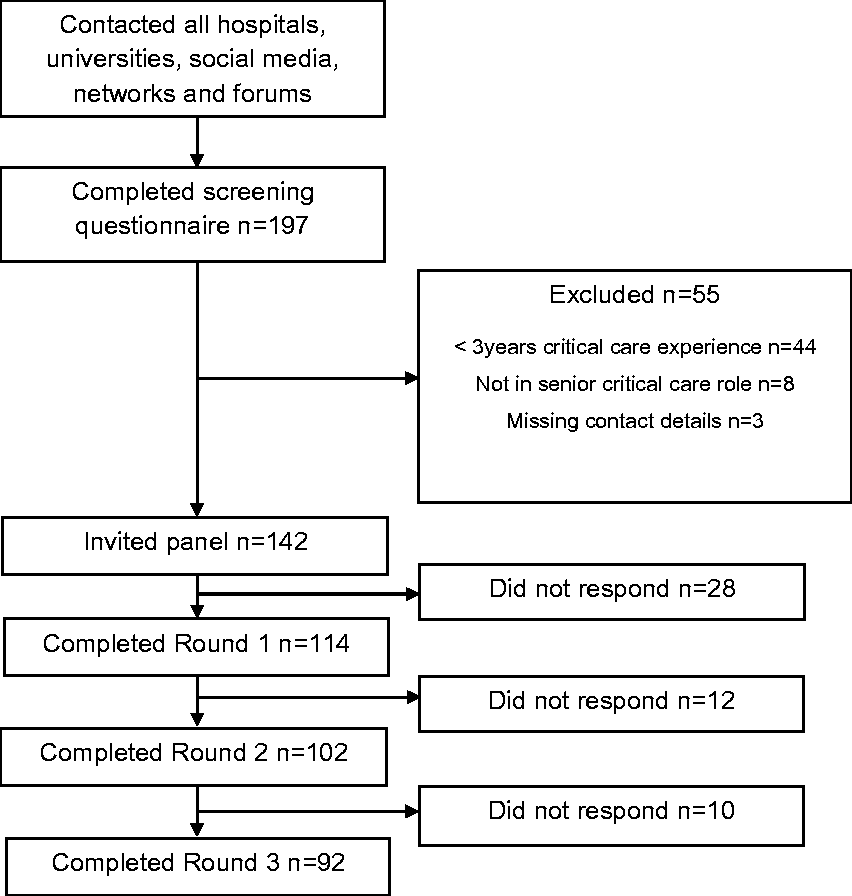
Round 1 consisted of 214 items of which 91 were deemed as essential. Based on responses, an additional eight questions were added to round 2, during which a further 11 items were deemed as essential. One additional item was added to round 3, and five items were determined as essential. Across all three rounds, 107 items reached consensus to be classified as essential, 73 not essential and consensus agreements was not reached in 33 (see Figure 2).
Inclusion and exclusion of items.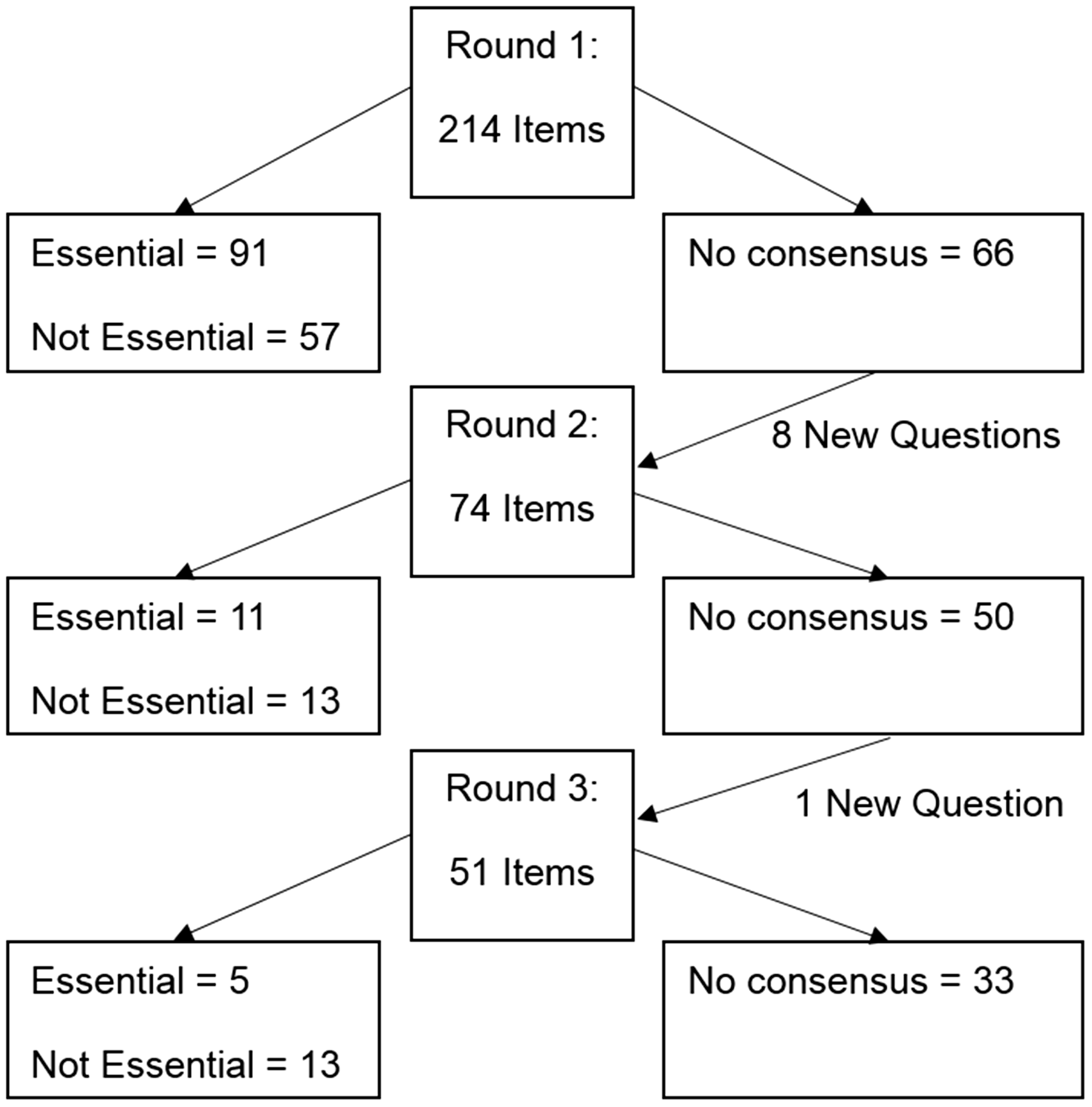
Assessment items determined as essential (consensus >70% ‘essential’).
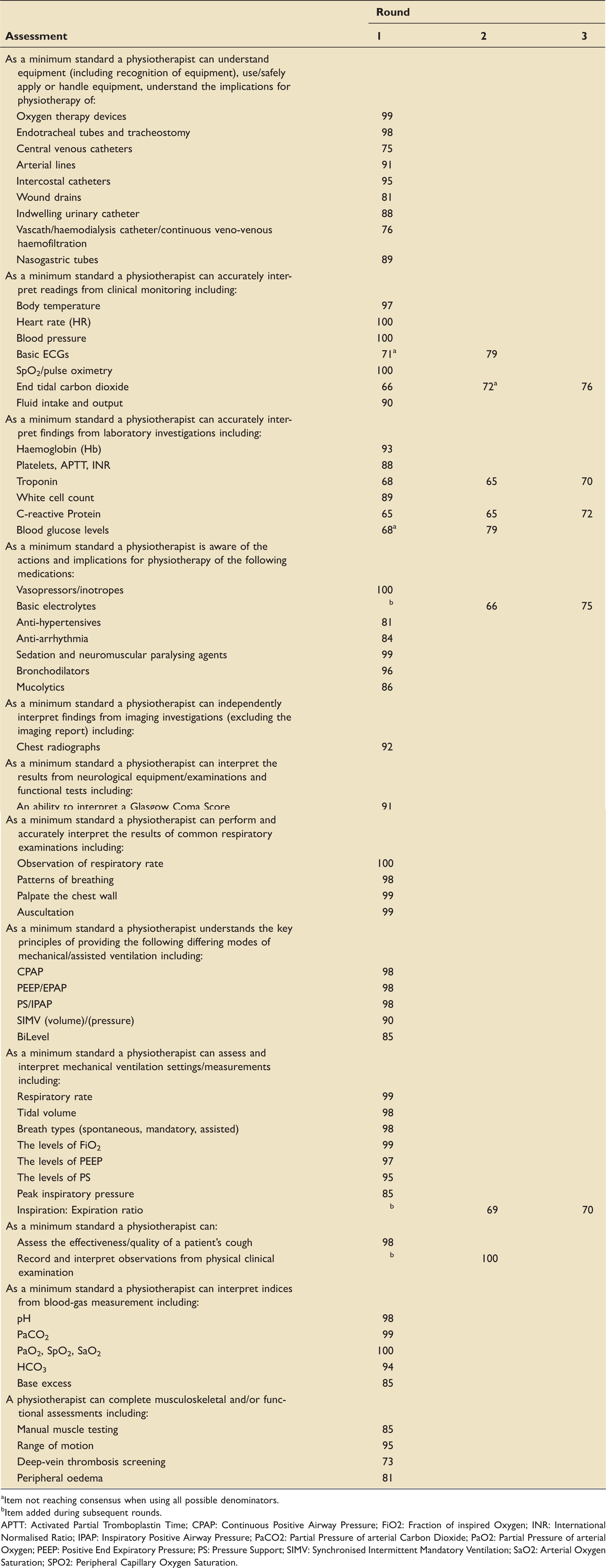
Item not reaching consensus when using all possible denominators.
Item added during subsequent rounds. APTT: Activated Partial Tromboplastin Time; CPAP: Continuous Positive Airway Pressure; FiO2: Fraction of inspired Oxygen; INR: International Normalised Ratio; IPAP: Inspiratory Positive Airway Pressure; PaCO2: Partial Pressure of arterial Carbon Dioxide; PaO2: Partial Pressure of arterial Oxygen; PEEP: Positive End Expiratory Pressure; PS: Pressure Support; SIMV: Synchronised Intermittent Mandatory Ventilation; SaO2: Arterial Oxygen Saturation; SPO2: Peripheral Capillary Oxygen Saturation.
Condition items determined as essential (consensus >70% ‘essential’).
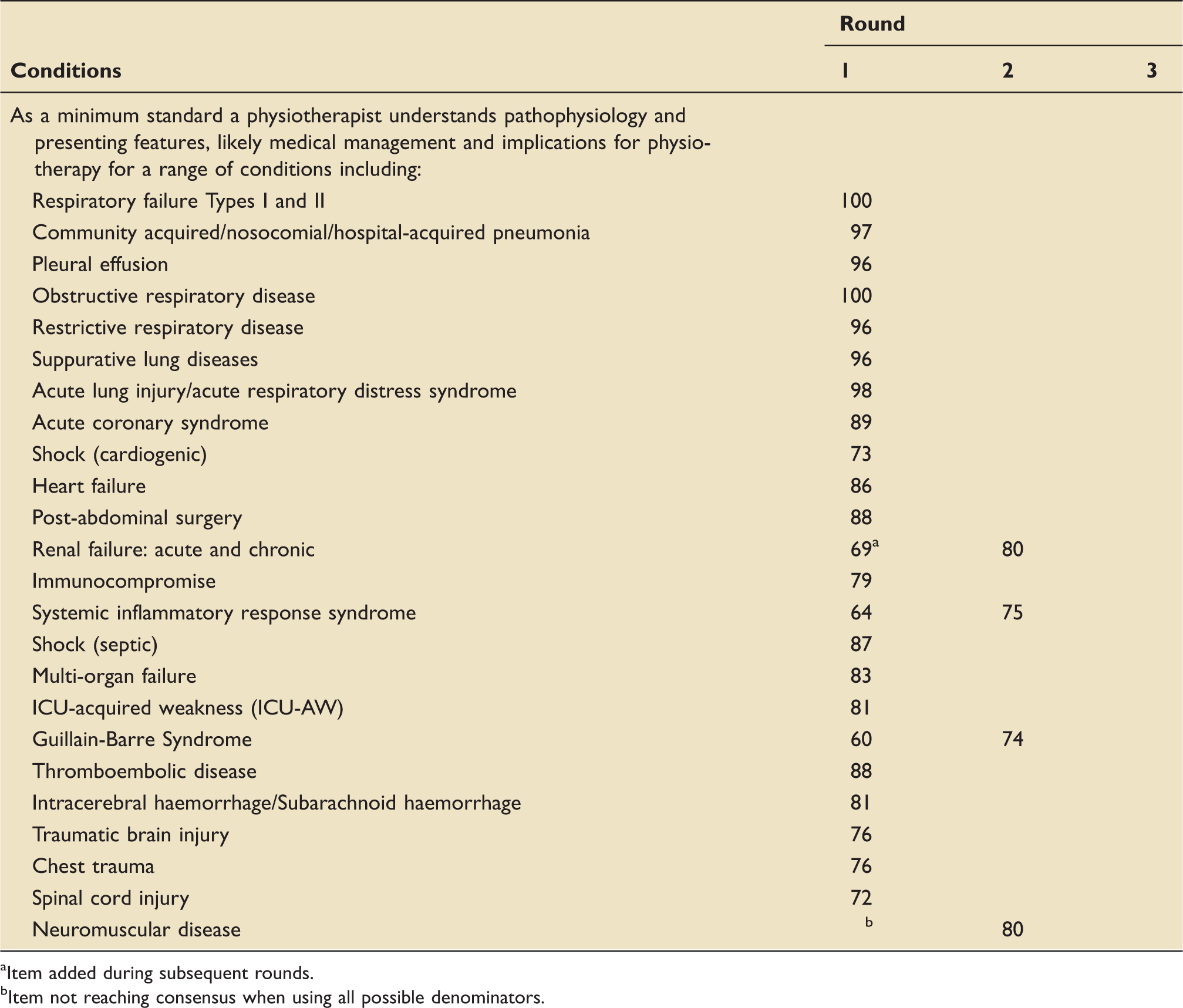
Item added during subsequent rounds.
Item not reaching consensus when using all possible denominators.
Treatment items determined as essential (consensus >70% ‘essential’).
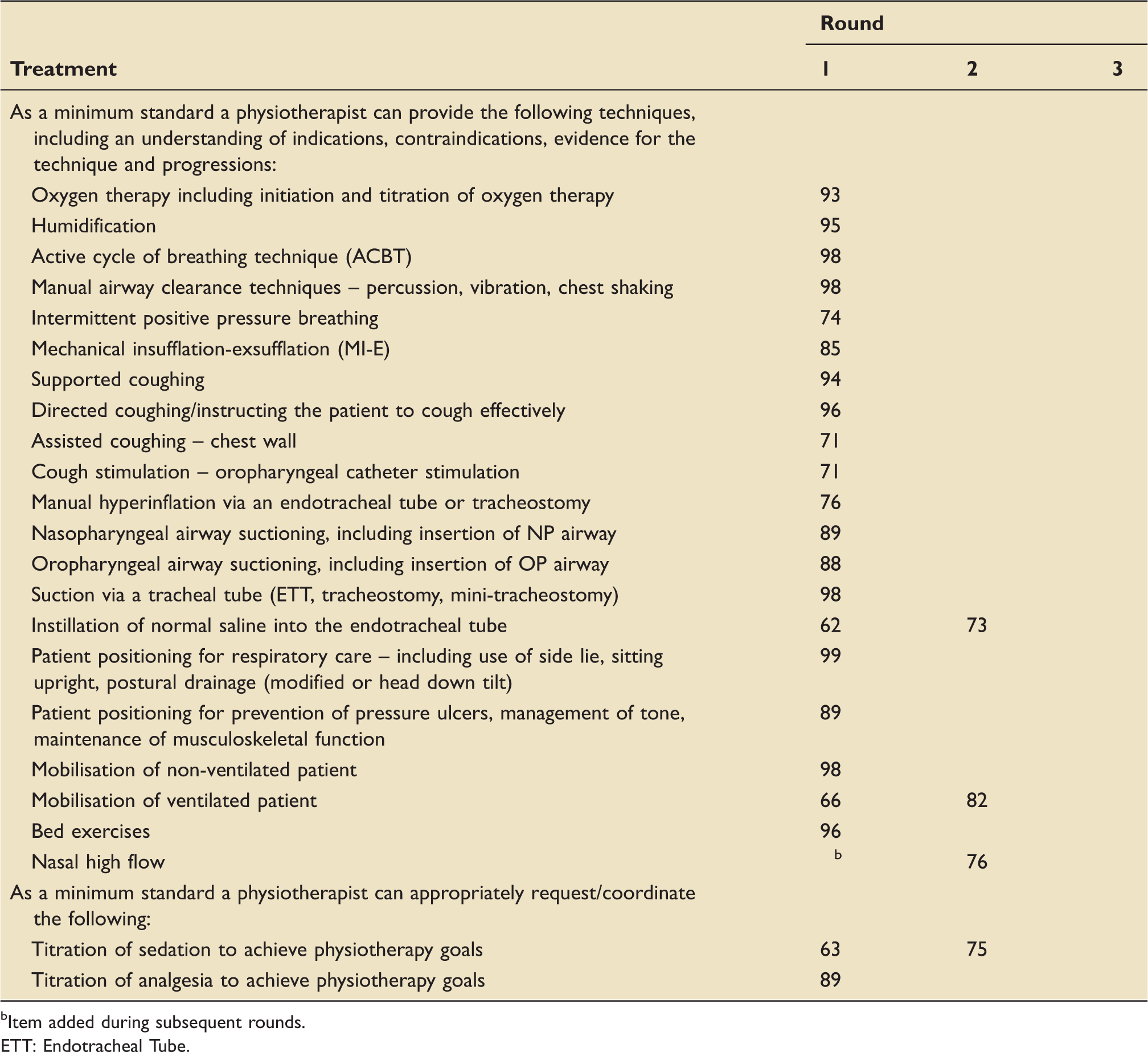
Item added during subsequent rounds. ETT: Endotracheal Tube.
Assessment items determined as not essential (consensus >70% ‘not essential’).
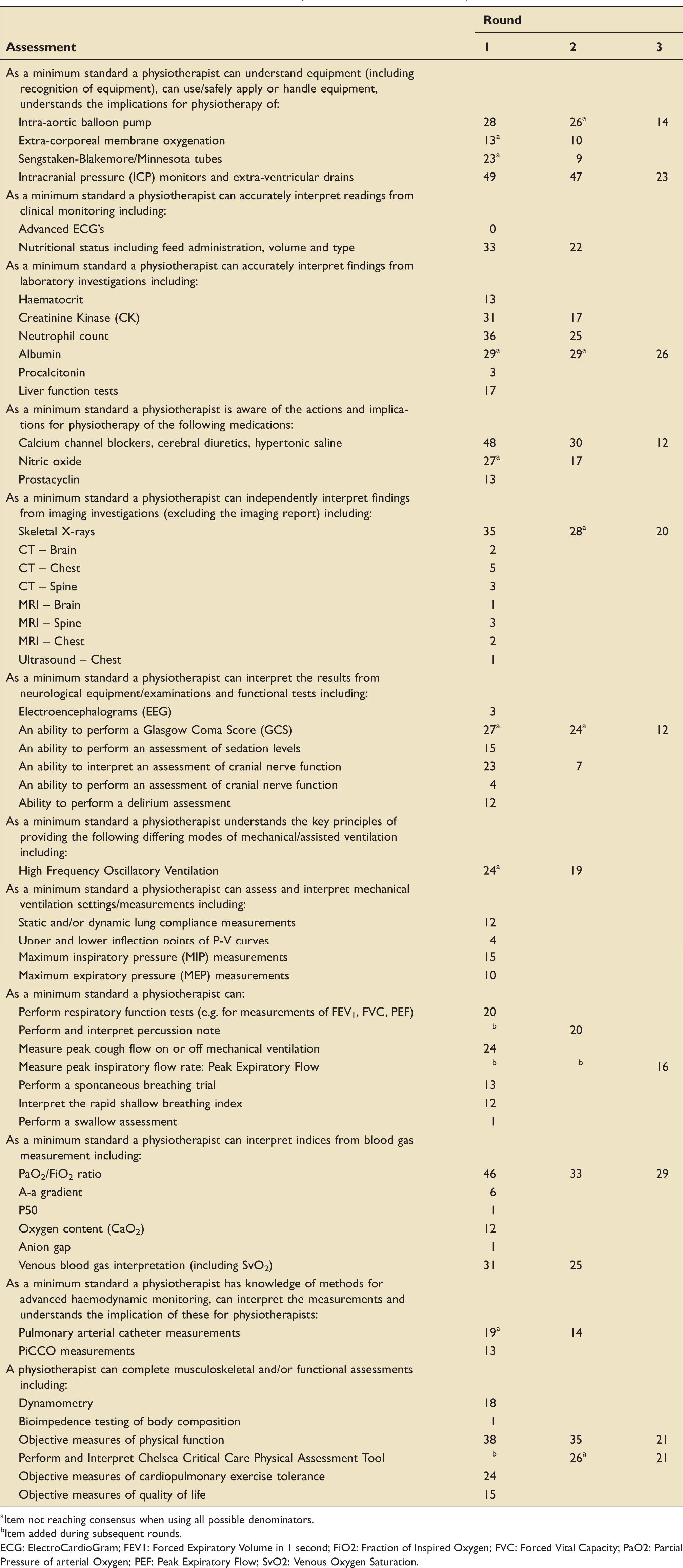
Item not reaching consensus when using all possible denominators.
Item added during subsequent rounds. ECG: ElectroCardioGram; FEV1: Forced Expiratory Volume in 1 second; FiO2: Fraction of Inspired Oxygen; FVC: Forced Vital Capacity; PaO2: Partial Pressure of arterial Oxygen; PEF: Peak Expiratory Flow; SvO2: Venous Oxygen Saturation.
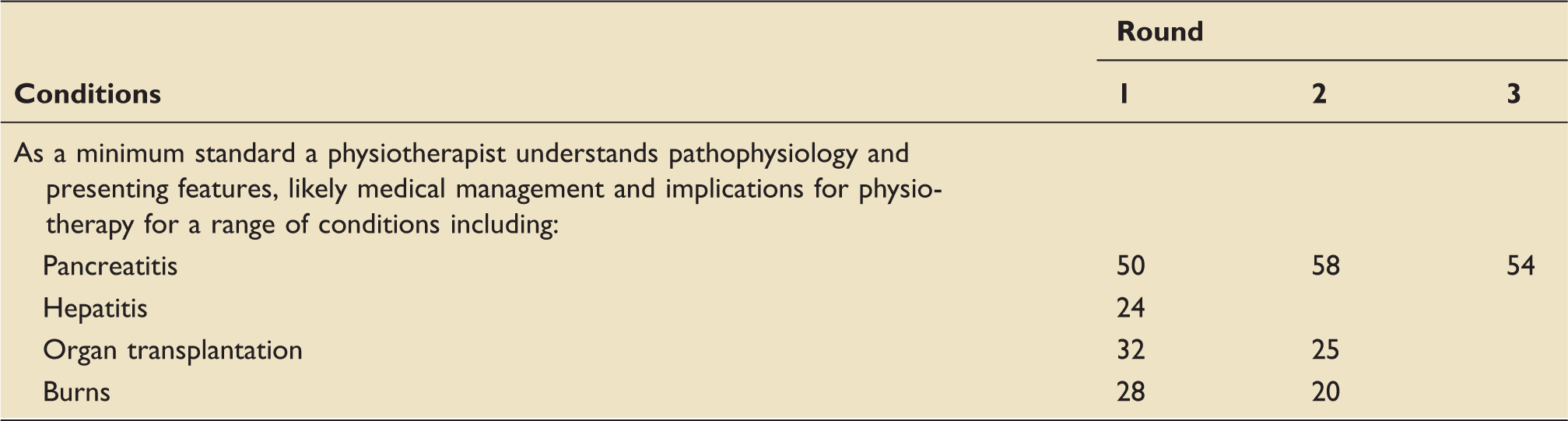
Condition items determined as not essential (consensus >70% ‘not essential’).
Treatment items determined as not essential (consensus >70% ‘not essential’).
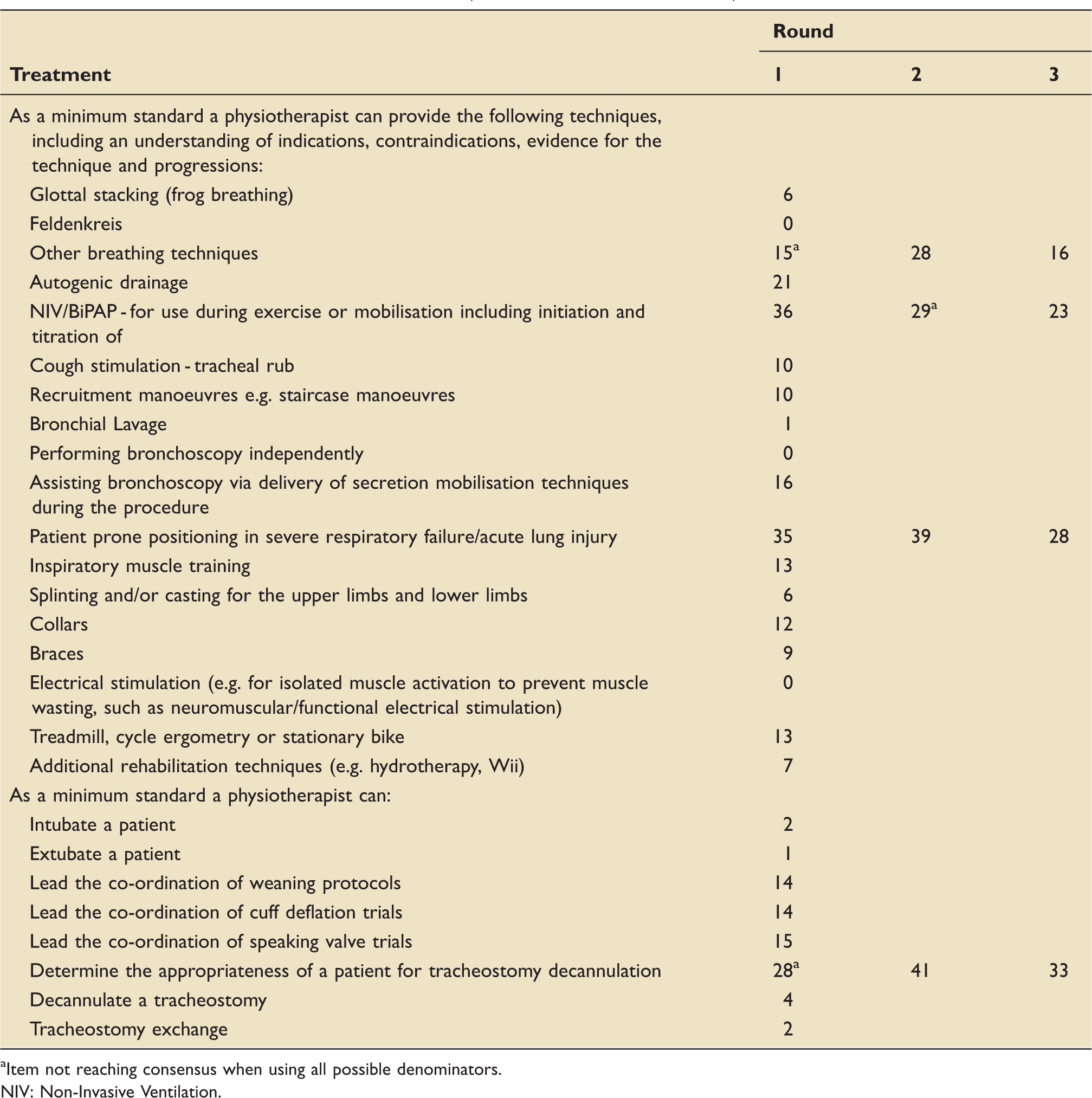
Item not reaching consensus when using all possible denominators. NIV: Non-Invasive Ventilation.
Assessment items not reaching any consensus.
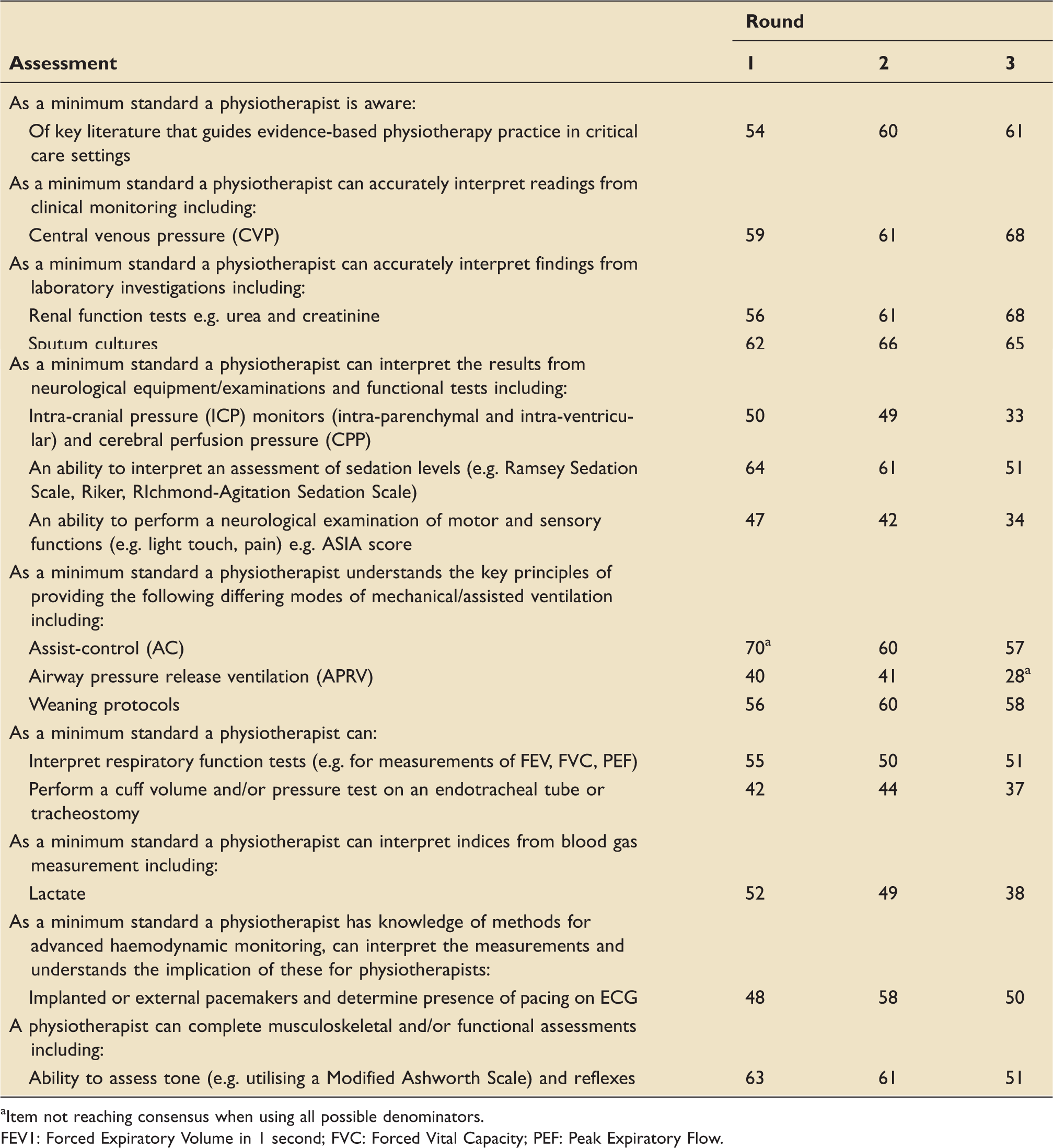
Item not reaching consensus when using all possible denominators. FEV1: Forced Expiratory Volume in 1 second; FVC: Forced Vital Capacity; PEF: Peak Expiratory Flow.
Condition items not reaching any consensus.
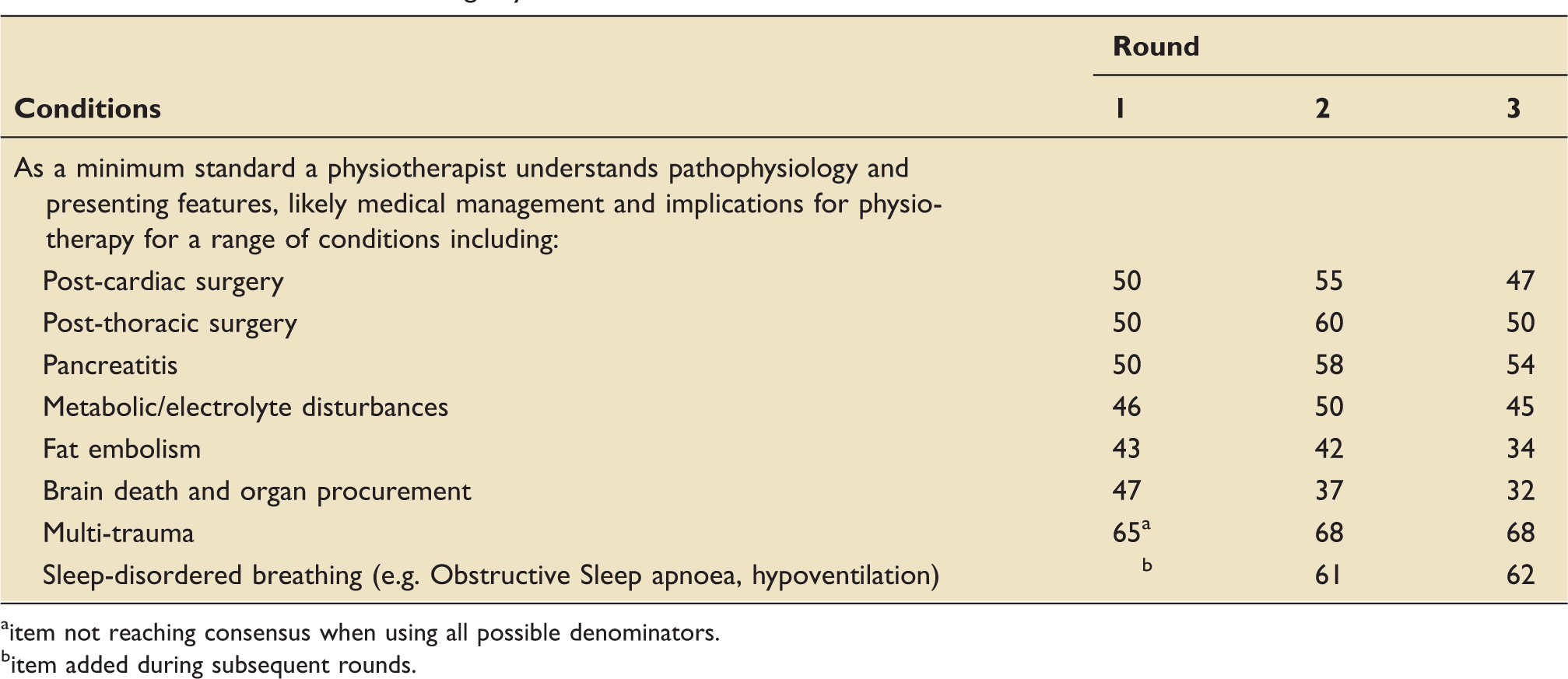
item not reaching consensus when using all possible denominators.
item added during subsequent rounds.
Treatment items not reaching any consensus.
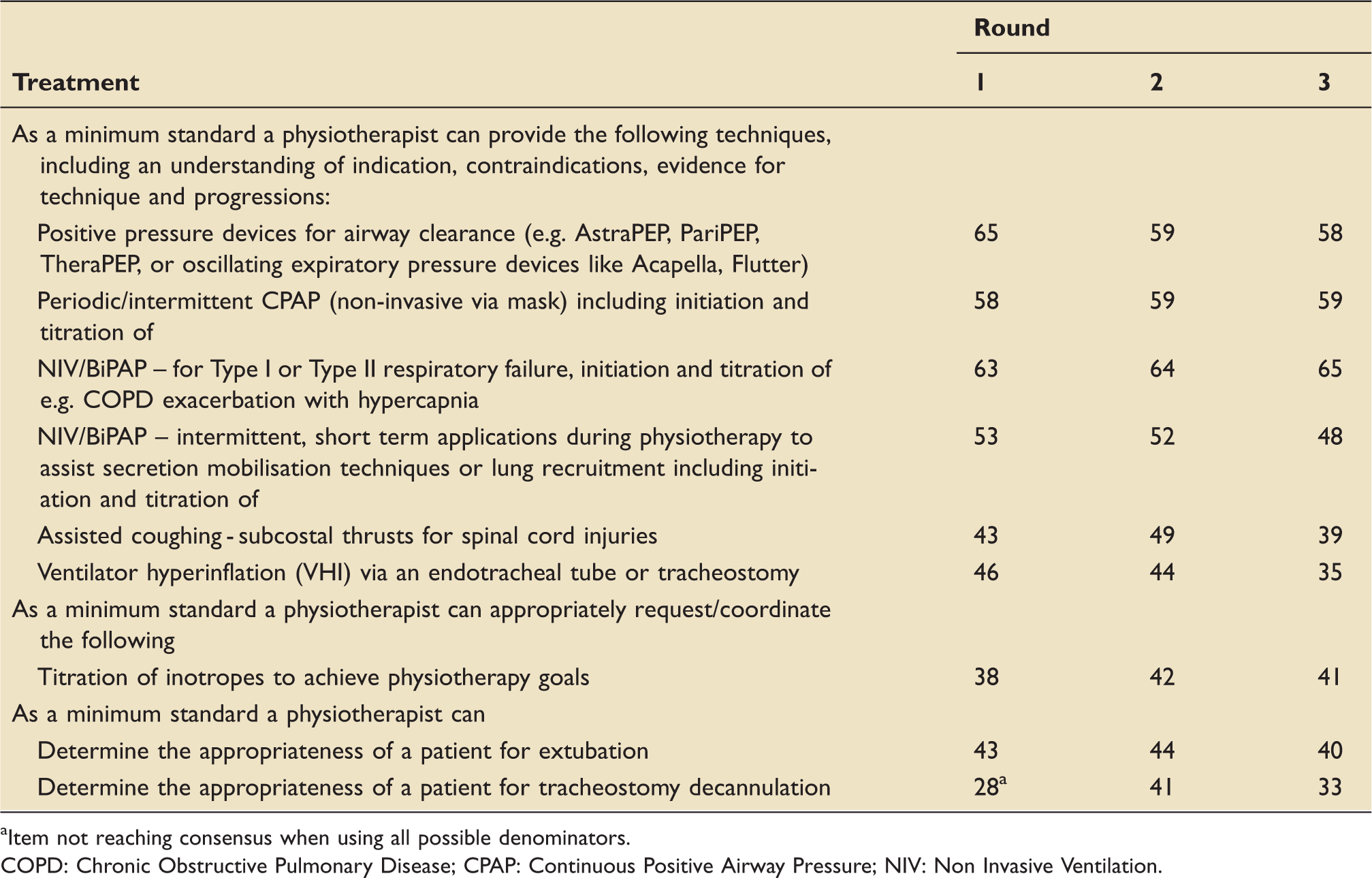
Item not reaching consensus when using all possible denominators. COPD: Chronic Obstructive Pulmonary Disease; CPAP: Continuous Positive Airway Pressure; NIV: Non Invasive Ventilation.
No consensus
Five highest ranked themes across all three rounds.
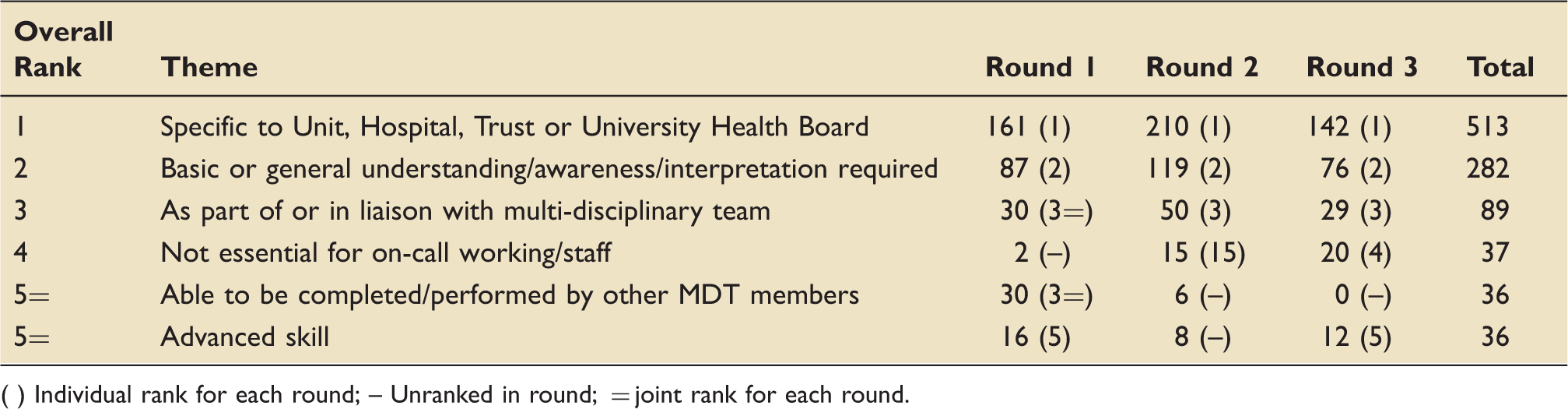
( ) Individual rank for each round; – Unranked in round; = joint rank for each round.
Discussion
The aim of this study was to explore the minimum standard of clinical practice for physiotherapists in critical care units across the UK. The rationale for the study was based on changing demands on oncall services, reductions in workforce capacity, variability in staff entry-level and postgraduate experiences and perceptions of variability in clinical practice.
In this three-round Delphi study of highly experienced critical care physiotherapists, 107 items of knowledge and skill have been deemed essential as a minimum standard of clinical practice in critical care in the UK. Furthermore, 73 such items have been determined as not essential for clinical practice. The challenge now is to consider how this clarification of requirements needs to be integrated into entry-level and postgraduate training, and within competency standards for on-call working.
The study had significant interest within the UK with a far higher than anticipated response to advertisement. In total, 142 physiotherapists were deemed eligible for inclusion and invited to participate with 114 completing round 1, of which 80.7% completed all three rounds. Whilst lower than the retention rate in the Australasian equivalent (90%), it is still above that accepted for Delphi-based studies. 17
The high response and retention rate were likely a result of targeted advertisement, use of personalised reports and regular electronic emails, as well as social media prompting. Similarly, the response rate may reflect the significant interest in the research topic and its current importance within supporting and standardising on-call working.5,8,10 Across the UK, on-call services are being placed under increasing pressure and regularly require non-respiratory specialist physiotherapists to contribute to rotas. 5 Standardising the role of the physiotherapist in critical care will help to support training, education, and competencies to support these staff, and to also ensure the ongoing delivery of high-quality assessment and treatment to the service user.
The participants had significant critical care experience (15 years in a senior role) and were all involved in the delivery of on-call teaching within their local organisation. This degree of experience is above that observed in similar studies8,10 and further enhances the validity of the results recorded.
In comparison to the findings of the Australasian Delphi, 8 the UK study had fewer items considered to be essential (107 vs 132) with similar numbers of non-essential items (73 vs 67 for UK and Australasia respectively).
A number of these items may be considered generic physiotherapy skills rather than specific to critical care, with some being deemed essential whilst others not or with no consensus. Within clinical monitoring, interpretation of temperature, heart rate, and blood pressure were determined as essential whereas advanced echocardiograms (ECGs) and nutritional status were not-essential. Similarly, in interpretation of laboratory investigations haemoglobin, platelets, and white cell count were determined as essential, yet haematocrit and neutrophil count were non-essential, see Tables 1 and 5. The authors suggest this reflects current clinical practice, with basic cardiovascular monitoring and interpretation of blood results being used to guide physiotherapy assessment and treatment, whereas more detailed understanding would not be required in an on-call scenario. These findings were common across both the UK and Australasian studies. 8 Of particular interest in relation to generic skills was the UK finding that completion of objective measures of physical function was not essential, which the Australasian study determined essential. 8 The reason for this difference is unclear, although is likely a reflection of the role of the physiotherapist in an on-call/emergency duty scenario within the UK, where physical function would not be deemed a priority.
Equally as concerning is the finding from the UK study that skills taught at entry level, i.e. performing and interpreting respiratory function tests, was deemed non-essential; however, these skills were both seen as essential in the Australasian study. 8 Reasons for this are unclear and would require further investigation.
This Delphi study, like that completed in Australia and New Zealand, 8 focussed purely on skill and knowledge requirements, and did not consider non-technical components. van Aswegen and colleagues 10 identified the following requirements for minimum practice in South Africa: (1) Integrated Medical Knowledge; (2) Multi-disciplinary teamwork; and (3) Physiotherapy practice. It is likely that the skill and knowledge items recorded in the UK are like those that would be encapsulated in integrated medical knowledge and physiotherapy practice, but not multi-disciplinary team working. Therefore, if multi-disciplinary team working were added, the number of items required for essential practice could be higher than the 107 recorded, with additional focus tasks such as communication, team discussion, and documentation needing to be considered.
As identified by Skinner et al., 8 each critical care unit has different caseloads, patient specialities, and complexity. Additionally, some centres deliver tertiary services such as major trauma, neurosurgery, and extracorpeal membrane oxygenation (ECMO). As a result, the knowledge and skills that the physiotherapist requires to work independently on critical care will vary. Throughout this Delphi project it was emphasised that items should only be considered a minimum standard if required to work on general critical care units. Therefore, it was assumed that items such as knowledge of ECMO would not be essential (e.g. not needed for most of UK critical care units). However, by the comments received in each round, this was still challenging. The theme of ‘Trust or University Health Board Specific’ occurred over 500 times during the three rounds emphasising that some still felt that items may need to be included if present at that critical care unit. However, most of these comments occurred when respondent replied ‘unsure’ to whether it was essential or not and therefore is unlikely to have influenced the final consensus result.
As with similar previous Delphi studies, there were a number of limitations to this study. Primarily, the length of each questionnaire may have resulted in response fatigue. 18 It was noted that fewer comments were received for later questions and there may have been a tendency to select answers more rapidly with less prior thought. To avoid this, participants were able to complete the survey over 4 weeks, with the option to regularly save progress. However, the authors are aware of intermittent technical issues that resulted in some answers not being completed.
In accordance with Skinner et al., 8 three methods for consensus agreement were completed. This was to reduce the potential impact of ‘unsure’ responses or non-completion of questions. The result was that some items neared essential or non-essential consensus but due to different calculations were unable to be included and therefore were classified as not reaching consensus. Additionally, the decision to use 70% as the cut-off criteria was based on the previous Delphi. 8 As commented by previous authors, changing this threshold will have resulted in more or less items being considered as essential and non-essential, respectively.
Much consideration is now required as to how these results can be used to standardise both physiotherapy education (entry-level and postgraduate) and clinical practice, and how the results may be used to reduce variation in practice especially during ‘on-call’ working. There is a need to determine who is responsible for delivering the training and education required to ensure physiotherapists have the necessary knowledge and skills to practice autonomously. The results of the study need to be discussed with both higher education establishments (delivering entry-level physiotherapy degree programmes) and National Health Service (NHS) organisations. Additionally, the results of the Delphi will be disseminated to the study participants with a plan for further discussion of findings and onward studies.
It is aimed that this project will allow organisations to standardise training and competencies, to reduce both single-site variations (e.g. service being delivered in a single critical care) and across-site variations. One proposed method would be to develop a model of competency framework similar to the critical care nursing framework (Critical Care Network Nurse Leads). 19 By using such a framework, it may also be possible to generate a tiered system (e.g. foundation; specialist; advanced) to further recognise the role of the physiotherapist within critical care. Through this process, it may be possible to improve the quality of the service provided to the patient by reducing the impact of the variances in physiotherapy practice and standardise clinical assessment, interventions, and management.
Conclusions
This study identified 107 items of knowledge and skills that are essential as a minimum standard for clinical practice by physiotherapists working in UK critical care units.
The findings of this study require dissemination, which may support training programmes in both higher education and the health service, to reduce variability in clinical practice.
Footnotes
Acknowledgements
The authors thank Elizabeth H Skinner, Peter Thomas, Julie C Reeve and Shane Patman for sharing all research design and supporting documents and all staff who completed the questionnaire surveys.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.