
Abstract
Purpose
Patients with alcohol-related disease constitute an increasing proportion of those admitted to intensive care unit. There is currently limited evidence regarding the impact of alcohol use on levels of agitation, delirium and sedative requirements in intensive care unit. This study aimed to determine whether intensive care unit-admitted alcohol-abuse patients have different sedative requirements, agitation and delirium levels compared to patients with no alcohol issues.
Methods
This retrospective analysis of a prospectively acquired database (June 2012–May 2013) included 257 patients. Subjects were stratified into three risk categories: alcohol dependency (n = 69), at risk (n = 60) and low risk (n = 128) according to Fast Alcohol Screening Test scores and World Health Organisation criteria for alcohol-related disease. Data on agitation and delirium were collected using validated retrospective chart-screening methods and sedation data were extracted and then log-transformed to fit the regression model.
Results
Incidence of agitation (p = 0.034) and delirium (p = 0.041) was significantly higher amongst alcohol-dependent patients compared to low-risk patients as was likelihood of adverse events (p = 0.007). In contrast, at-risk patients were at no higher risk of these outcomes compared to the low-risk group. Alcohol-dependent patients experienced suboptimal sedation levels more frequently and received a wider range of sedatives (p = 0.019) but did not receive higher daily doses of any sedatives.
Conclusions
Our analysis demonstrates that when admitted to intensive care unit, it is those who abuse alcohol most severely, alcohol-dependent patients, rather than at-risk drinkers who have a significantly increased risk of agitation, delirium and suboptimal sedation. These patients may require closer assessment and monitoring for these outcomes whilst admitted.
Keywords
Introduction
There has been a sustained rise in the numbers of high-risk alcohol users requiring admission to intensive care units (ICUs) 1 and alcohol-related disease is implicated in up to 25.4% of all admissions to Scottish ICUs.2,3These patients can be more difficult to maintain in a cooperative state, may develop alcohol withdrawal syndrome (AWS), have higher ICU mortality rates and poorer long-term outcomes.4–6
The ‘ICU triad’ of agitation, pain and delirium is increasingly recognised as being an important factor of a patient’s ICU stay. 7 Traditionally, sedation has been utilised as a means of modulating patients’ awareness of a potentially distressing environment, alleviating anxiety and facilitating interventions. However, if over-sedated, critically ill patients can be predisposed to prolonged time on ventilator support and longer ICU stays.8–10 It is now well recognised that the implementation of sedation protocols which minimise overall sedative use result in reduced hospital stays and mortality.11,12
AWS typically occurs 6–8 h following cessation of alcohol intake in the chronic alcohol user and can present with autonomic hyperactivity, hallucinations, agitation and seizures. There is overlap between AWS and delirium as both can present with hallucination and agitation. However, the aetiology of delirium is much broader and whereas, the treatment of AWS is primarily with benzodiazepines, delirium is treated with a multifactorial approach and drug treatment avoided where possible.
Previous studies have examined the impact of agitation and delirium in the ICU setting. However, studies on how alcohol-abuse patients differ in terms of their agitation, delirium status and sedative management compared to low-risk controls are limited. From previous studies, estimates of the incidence of agitation in alcohol-abuse patients vary considerably from 12 to 72.7% 13 and there is conflicting evidence over sedation requirements in this cohort. As far as we can establish, no study has comprehensively examined how these factors interact in patients with a history of alcohol use disorders (AUDs) admitted to ICU.
We aimed to determine if there is a difference in levels of agitation, delirium and sedative requirements between patients with alcohol-use disorders and those with no alcohol issues admitted to a general ICU.
Methods
Ethics approval requirement was waived by the local ethics committee but Caldicott guardianship was sought and granted. This service evaluation provided a retrospective review of a prospectively acquired database of Level 3 ICU patients admitted to our unit over a 12-month period (June 2012–May 2013). Level 3 ICU care refers to that of patients requiring multiple organ support or advanced respiratory support alone, as defined by the UK Intensive Care Society. This project took place in the Glasgow Royal Infirmary – a 20-bedded general mixed medical–surgical ICU, situated in an area of high socio-economic deprivation where alcohol abuse is a known problem.
Patients and group allocation
Patients were included who were ≥ 18 years of age requiring Level 3 care. Patients were stratified into three risk categories based upon a composite scoring system on admission to the ICU: Low risk, at risk and alcohol dependency (Appendix). Fast Alcohol Screening Test scores were used if recorded prior to ICU admission during the present admission to hospital, or alternatively, by World Health Organisation ICD-10 classification for AUDs.14–16 Patients’ deemed ‘at risk’ included those where identifiable physical or psychological harm resulted from alcohol use within the last 12 months, whereas ‘Alcohol Dependency’ describes addictive behaviour to alcohol intake associated with tolerance, withdrawal and persistence despite harm. Presence of liver disease was determined according to either positive liver biopsy or imaging-proven cirrhosis. These were recorded prospectively, on admission to hospital. For the purposes of this project only the sentinel admission was recorded. All data were extracted via the electronic patient records, CareVue (Philips Medical Systems, Eindhoven, the Netherlands) and WardWatcher (Critical Care Audit Ltd, Ilkley, UK).
Matching
Patients in the alcohol dependency and at-risk cohorts were matched to patients in the low-risk cohort according to their Acute Physiology and Chronic Health Evaluation II (APACHE-II) score and a diagnosis of sepsis during admission. This accounted for patients with higher disease severities potentially requiring greater sedation and both sepsis and high disease severity having been identified as significant independent risk factors for delirium and therefore, potential confounders. 17
Clinical and demographic data were collected of patient’s length of stay (LOS), age, gender, APACHE-II score, presence of liver disease and ICU survival status.
Agitation
Agitation scores were recorded by nursing staff according to the Bloomsbury Sedation Scale (Appendix). This scale varies from −3 (unrousable) to 3 (agitated and restless). These data were extracted retrospectively and recorded for each day of admission. Agitation was defined as either a Bloomsbury sedation score of 3 or identification of a descriptor within the patient notes indicative of agitation using methodology previously described in the literature. 18 Adverse events, defined as either attempted or actual self-extubation, attempting to get out of bed or pulling at nasogastric, nasojejunal tubes or other lines, were recorded retrospectively using the chart-screening method.
Delirium
A validated chart-review method was undertaken to retrospectively screen for delirium, utilising detailed daily ward round and nursing notes. This method has a sensitivity of 74% when compared to the confusion assessment method (CAM) and is validated for use in the ICU setting, with a positive predictor accuracy of 87%.19,20 Onset and duration of delirium in days and evidence of reversibility (defined as delirium improving within one nursing shift equivalent to 12 h) were recorded. Patients with a diagnosis of a chronic cognitive impairment such as dementia were excluded from the analysis of delirium.
Sedation
The total cumulative dosages each subject received of sedatives (propofol, dexmedetomidine and clonidine), opioids (morphine, alfentanil, fentanyl and methadone), benzodiazepines (lorazepam, diazepam and temazepam) and haloperidol were collected and the average daily dose for each drug calculated. This included scheduled, stat and PRN doses and continuous IV infusions received. Benzodiazepines were converted into lorazepam equivalents and opioids into morphine equivalents.21,22 Total number of individual sedative drugs and the administration of third-line drugs (clonidine or dexmedetomidine) were recorded.
Statistical approach and analysis
Descriptive statistics were used to evaluate characteristics of agitation, delirium and aspects of sedative practice. Chi-squared and Fisher’s exact test were used for comparisons of categorical data. The two-sample T-test and Mann–Whitney U test were used for comparisons of continuous data. Logistic regression was used for univariate analysis to calculate odds ratios for agitation, delirium and adverse events, with adjustment for age and sex in multivariate analysis. Differences in sedative dosages were modelled using ANOVA. Univariate linear regression analysis was then used to compare the alcohol subgroups to the low-risk group, with adjustment for age and sex. Mean daily doses of all drugs were log transformed prior to fitting the regression model and coefficient estimates and 95% confidence intervals exponentiated to give the ratio of means. Alcohol subgroups were compared to the low-risk cohort for analyses unless indicated.
All analyses considered an alpha value of 0.05 as statistically significant and confidence intervals were calculated at the 95% level. All analyses were performed using statistical software SPPS Version 21.0® (SPSS Inc., Chicago, Illinois, USA).
Results
Characteristics of the study patients.
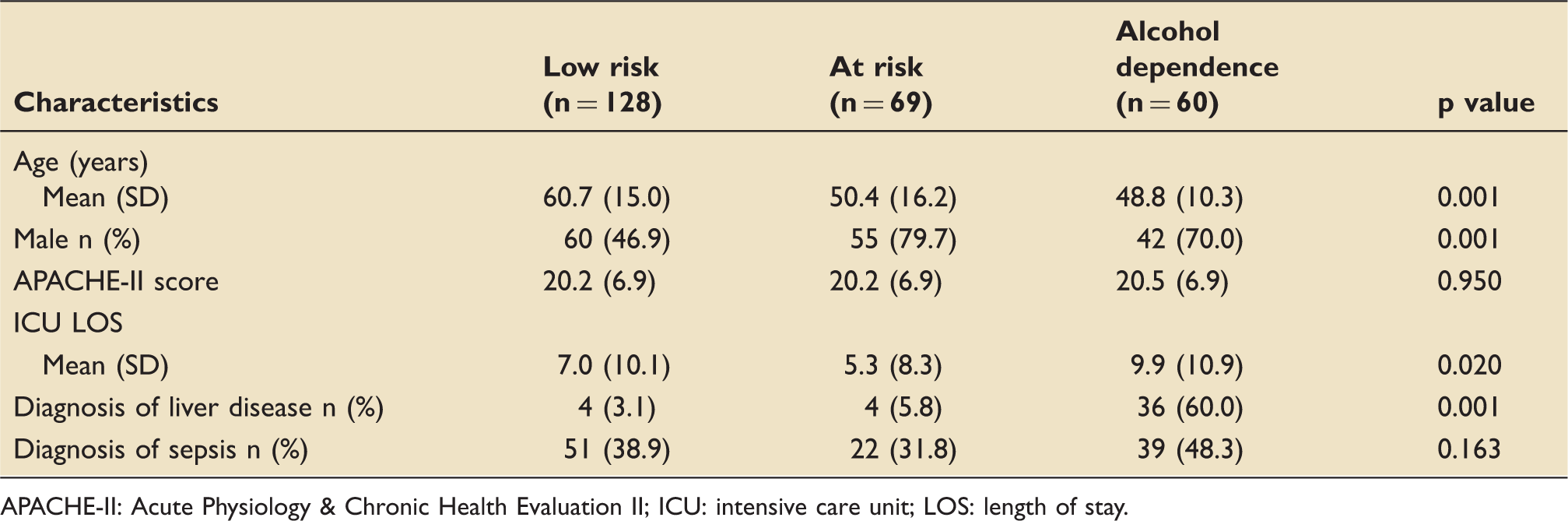
APACHE-II: Acute Physiology & Chronic Health Evaluation II; ICU: intensive care unit; LOS: length of stay.
Agitation and adverse events
Adjusted odds ratios for the risk of developing agitation, delirium and adverse events for alcohol cohort subgroups compared to low-risk cohort (models adjusted for age and sex).

Adverse events defined as attempted/actual self-extubation, attempting to get out of bed and pulling at NG/NJ or other lines.
Compared to the low-risk cohort, the incidence of adverse events was significantly higher in the alcohol-dependence cohort (48.3% versus 28.1%, p=0.007) but similar in at-risk patients (27.5%, p = 0.970). After adjustment for age and gender, the odds of an adverse event occurring were 2.65 greater (CI 1.29–5.46, p = 0.008) in an alcohol-dependent patient compared to low-risk patient (Table 2).
Agitation and sedation scores
A total of 7731 Bloomsbury sedation scores were collected over 2203 patient study days (mean 3.5 scores per patient day) with no significant differences in number of scores collected between cohorts (p = 0.320). Patients in the low-risk group were ‘optimally sedated’ (scores 0–2 or ‘natural sleep’) 74.9% of the time, compared to 65.2% in the at-risk cohort (p < 0.001) and 62.8% in the alcohol-dependent cohort (p < 0.001) (Figure 1). Compared to the low-risk group, alcohol-dependent patients showed a predisposition to lower conscious levels, with sedation scores of −3 to −1 (19.2% versus 13.3%, p < 0.001). Overall, patients in the at-risk cohort (21.6% of scores) and alcohol-dependence cohort (17.8%) were more frequently ‘agitated and restless’ than low-risk patients (11.4%, p < 0.001). It should be noted, however, that 38.7% (n = 128) of all ‘agitated and restless’ scores for the at-risk cohort came from one patient (representing 39.4% of their scores).
Average quality of sedation achieved for each cohort according to sedation scores collected (excludes when patients were paralysed – 0.2–0.7% of scores).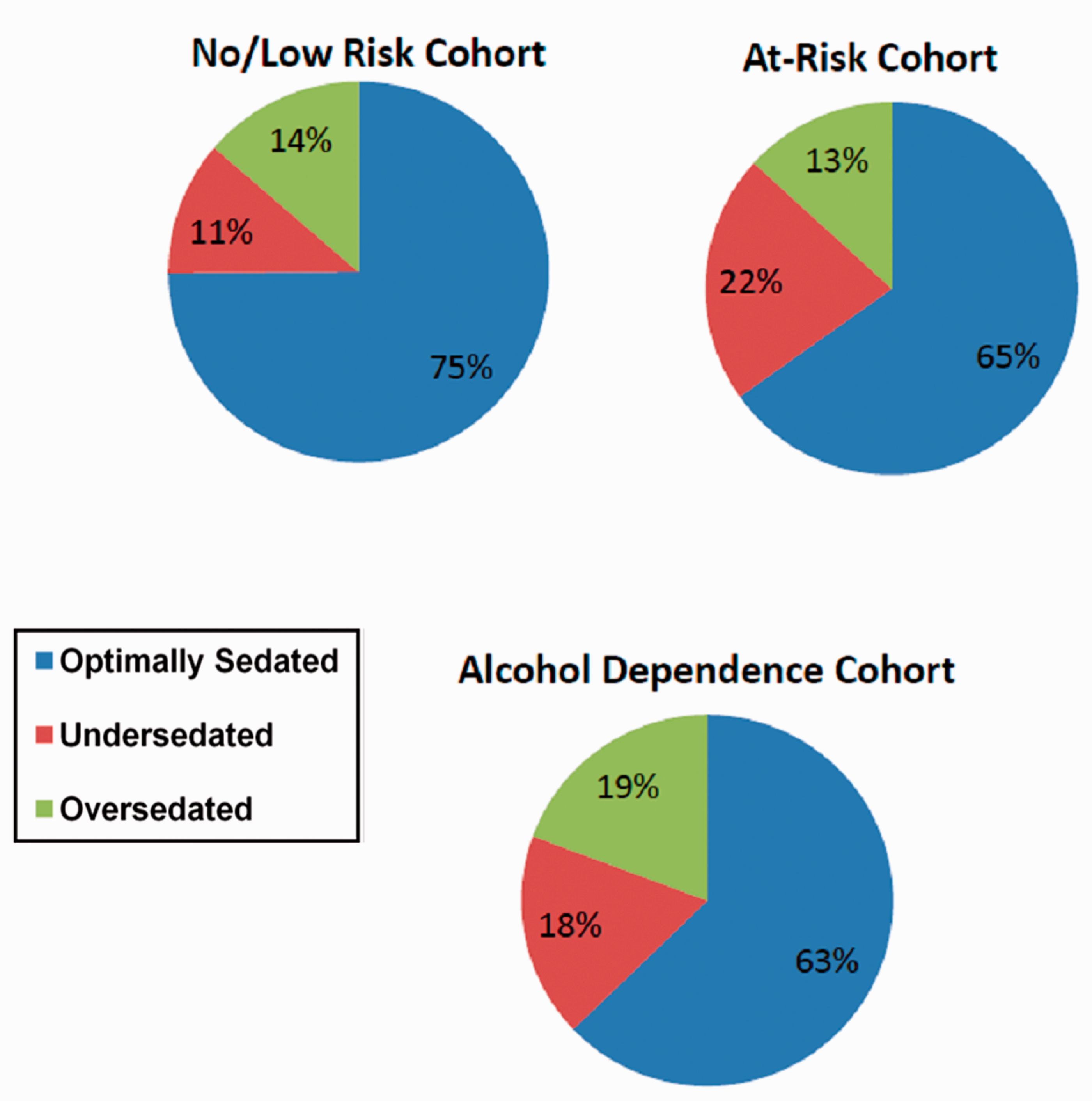
Delirium
Analysis of the incidence and characteristics of agitation and delirium.
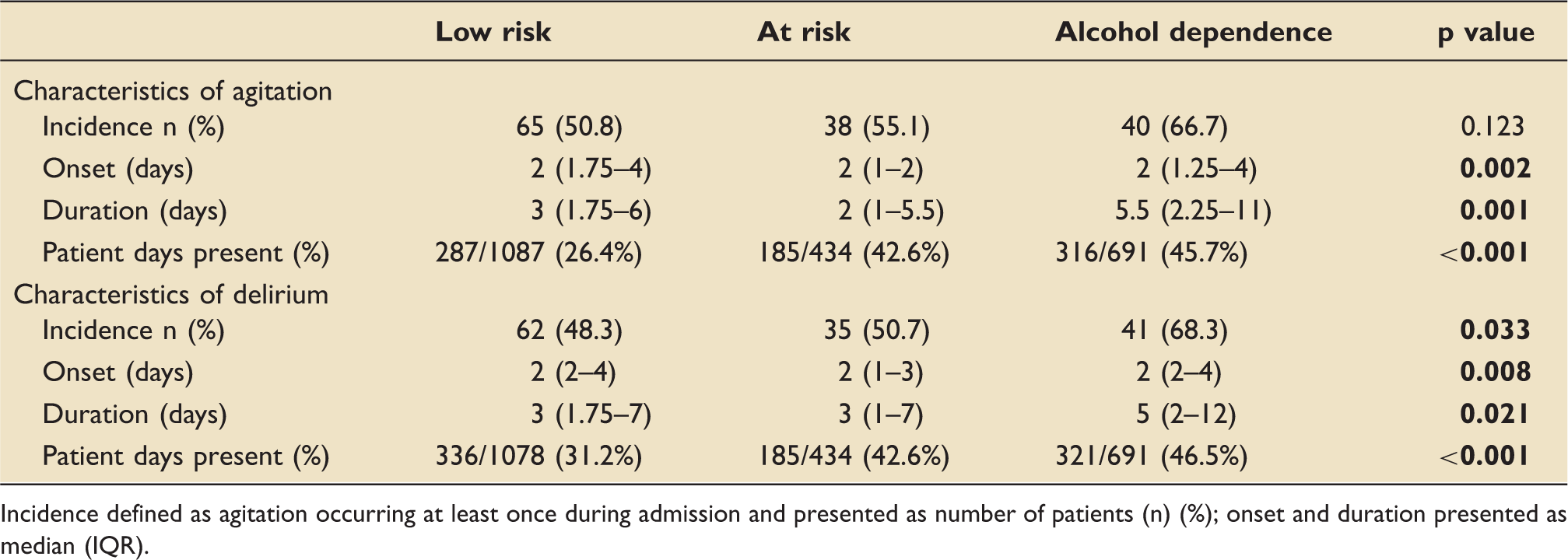
Incidence defined as agitation occurring at least once during admission and presented as number of patients (n) (%); onset and duration presented as median (IQR).
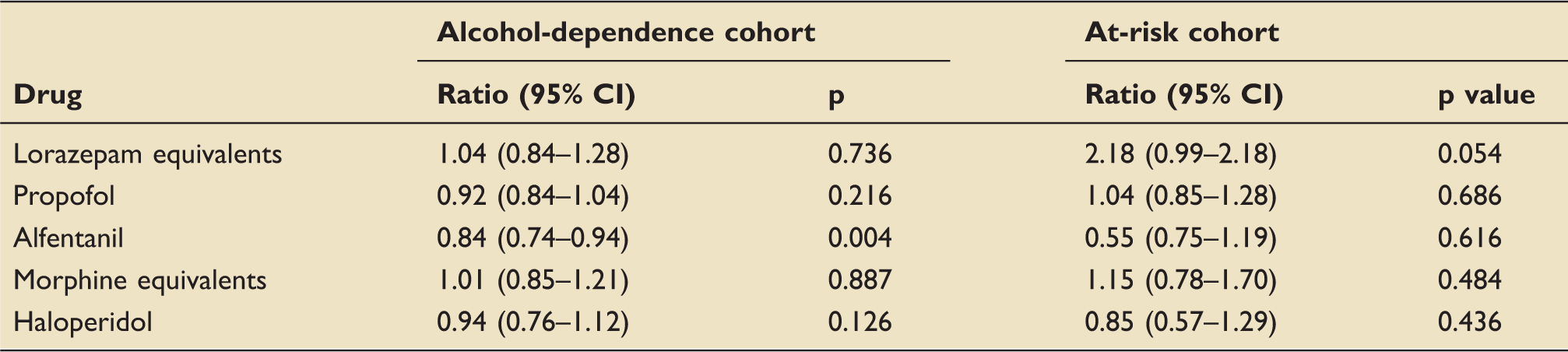
Mean daily dosages of sedatives for alcohol-dependence and at-risk cohorts compared to low-risk cohort (models adjusted for age and sex).
As patients with alcohol dependency were found to be at a significantly increased risk of delirium, possible factors related to delirium were entered into univariate and multivariate analysis to identify possible risk factors for this population (Appendix). Cumulative dose of morphine equivalents, lorazepam equivalents and number of sedative drugs was associated with an increased risk of delirium on univariate analysis, with total LOS (OR 1.13 CI 1.00–1.27, p = 0.043) and a diagnosis of sepsis (OR 5.07 CI 1.12–23.01, p = 0.036) remaining as significant risk factors on multivariate analysis.
Sedation
Characteristics of sedation
Patients with alcohol dependence received a mean of 3.2 different sedatives during their stay, significantly more than the low-risk cohort (3.2 versus 2.6, p = 0.019). However, the at-risk cohort received a similar variety of sedation compared to the low-risk cohort (2.3 versus 2.6, p = 0.178). Alcohol-dependent patients did not require third-line sedatives more often than low-risk patients.
Alcohol-dependent patients were significantly more likely to receive benzodiazepines (OR 1.67 CI 1.16–2.39, p = 0.005) and haloperidol (OR 1.51 CI 1.02–2.24, p = 0.040), but were no more likely to receive propofol or opioids. Patients in the at-risk cohort were significantly less likely to receive opioids than low-risk patients (OR 0.29 CI 0.14–0.58, p = 0.001), but were no more likely to receive benzodiazepines, propofol or haloperidol.
Dosages of sedatives
Adjusting for age and gender, alcohol-dependent patients received similar mean daily dosages for all drugs except alfentanil, where these patients used less (OR 0.84, CI 0.74–0.94, p = 0.004), compared to low-risk patients. Despite receiving significantly more propofol and benzodiazepines on univariate analysis, adjusting for age and gender, patients in the at-risk cohort received similar doses for all sedatives compared to low-risk patients (Table 4).
Discussion
Agitation
Our 55.6% estimate of the incidence of agitation in ICU patients resembles previous findings. 18 However, across the literature agitation varies considerably, likely due to varying definitions.13,23 Our population is at increased risk. Agitation has previously been identified as an independent risk factor for self-extubation, and this is reflected in our finding that alcohol-dependent patients are significantly more likely to experience an adverse event in ICU compared to patients with no alcohol issues. Hence, modulating agitation in these higher risk patients could reduce rates of adverse events such as self-extubation and falls. 24 Our findings also indicate that although the incidence of agitation is not significantly elevated in ‘at-risk’ patients, in those who do exhibit agitation, it occupies a substantial proportion of patient days.
In our population, whilst patients had favourable levels of sedation for the majority of the time, both alcohol subgroups exhibited substantially more time ‘agitated and restless’. We also found that alcohol-dependent patients are more difficult to maintain in an aroused and cooperative state and hence, are more likely to become over-sedated. There is greater tendency to suboptimal sedation, with scores indicating over-sedation and agitation both more frequent than in low-risk patients. These results are consistent with a similar analysis of much smaller study by de Wit et al. 25
Delirium
As for agitation, estimates for the incidence of delirium in critically ill patients show considerable variability depending upon the population studied and the diagnostic criteria utilised. Our estimate of 53.7% is consistent within these parameters. With regards to delirium in AUD patients, only two studies have previously evaluated the role of alcohol in the development of delirium in ICU patients, with both identifying it as a significant risk factor.26,27 Both previous studies had extremely conservative definitions of alcohol intake. Our study goes further in suggesting that alcohol-dependent patients are at greatest risk, whilst at-risk drinkers have a similar risk to baseline.
Sedation
Our findings show that alcohol-dependent patients were significantly more likely to receive benzodiazepines and haloperidol than patients with no alcohol issue but were no more likely to receive opioids or propofol. The increased prescription of benzodiazepines in this cohort is potentially attributable to its use in the treatment of AWS. However, benzodiazepines have deliriogenic properties and particularly in AUD patients with liver cirrhosis the effects of diazepam can be perpetuated due to its long half-life. 28 Consequently, lorazepam may be preferable in this situation due to its more rapid hepatic metabolism to inactive lorazepam glucuronide. Daily dose of haloperidol was similar across all cohorts, most probably due to standardised protocols governing its prescription in our unit.
Patients in the alcohol-dependent cohort required significantly lower dosages of alfentanil. Similar findings were documented by Karir et al. 29 who found that ICU patients with alcohol dependency required significantly less opioids but similar propofol doses, compared to patients with no alcohol issues. The physiological basis for this may be due to altered clearance of the drug in alcohol dependency or hepatic encephalopathy with altered drug metabolism. The liver is the main site of metabolism for most opioids via the CYP and glucuronidation pathways which can both become impaired in liver disease, resulting in a reduction in dose of opioid required for equivalent effect.30,31
Indeed, 60% of patients in the alcohol-dependence cohort had liver disease compared to 5.8 and 3.1%, respectively, in the at-risk and low-risk cohorts. The greater variance in daily dosing of propofol and benzodiazepines amongst alcohol dependents could be attributed to the potential for diverse presentations of encephalopathy.
Strengths and limitations
This service evaluation had a number of strengths. Identification of patients and stratification into risk categories were prospectively defined and the sample size was sufficiently large enough to identify differences between cohorts. This project also had limitations. We utilised a retrospective design, with definitions of agitation and delirium applied to a prospectively collected database. Our sample was limited to a single-centre ICU, which serves a relatively deprived area of Glasgow. Therefore, our population may differ from others which may limit its external validity. It would have been preferable to match for age and sex in addition to APACHE-II and sepsis, although due to the constraints of the pool of low-risk patients available for matching, this was not possible. Due to the incidence of CAM-ICU scoring in our unit at the time of data extraction being low, the chart-screening method was used as the primary source. Although it has been shown that this method has reasonable research efficacy in the ICU setting, it has reduced accuracy compared to prospective collection of CAM-ICU scores and as such, this method is associated with a degree of subjectivity. Additionally, it was also more difficult to accurately identify patients with hypoactive delirium using this method, so we may have underestimated the incidence of delirium in our cohort, as hyperactive delirium would be more readily recognised.
Conclusions
Our analysis demonstrates that alcohol-dependent patients, rather than at-risk drinkers have a significantly increased risk of agitation, delirium and suboptimal sedation in ICU. These findings highlight the need for concerted efforts to diagnose and actively manage agitation and delirium particularly in those with alcohol dependency.
Supplemental Material
Supplemental material for The influence of alcohol abuse on agitation, delirium and sedative requirements of patients admitted to a general intensive care unit
Supplemental material for The influence of alcohol abuse on agitation, delirium and sedative requirements of patients admitted to a general intensive care unit by Donald Stewart, John Kinsella, Joanne McPeake, Tara Quasim and Alex Puxty in Journal of the Intensive Care Society
Footnotes
Author’s contributions
All authors were involved in the design of the study. DS collected and analysed the patient data and was a major contributor in writing the manuscript. JK, JMP, AP and TQ provided advice on the analysis of the data and manuscript and were heavily involved in its critical revision. All authors were involved in the drafting and editing of the final manuscript. All authors read and approved the final manuscript and accept accountability for the work.
Acknowledgements
The study was performed at the Intensive Care Unit of Glasgow Royal Infirmary, Glasgow, UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The lead author, Donald Stewart, received funding for the project from the Wolfson Foundation (Intercalated Award). The Wolfson Foundation were not, however, involved in the design, collection, analysis or interpretation of data in this study.
Ethics approval and consent to participate
The local ethics committee for NHS Greater Glasgow and Clyde (West of Scotland Research Ethics Committee) were approached and confirmed that approval was not required. Caldicott Guardian approval was sought and granted.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.