
Abstract
The mechanisms by which closed chest cardiac massage produces and maintains blood flow during cardiopulmonary resuscitation are still debated. To date, two main theories exist: the “cardiac pump”, which assumes that blood flow is driven by direct cardiac compression and the “chest pump”, which hypothesizes that blood flow is caused by changes in intrathoracic pressure. Newer hypotheses including the “atrial pump”, the “lung pump”, and the “respiratory pump” were also proposed. We reviewed studies supporting these different theories as well as the clinical evidences on the utility of mechanical devices proposed to optimize cardiopulmonary resuscitation, in view of their pathophysiological assumptions with regard to the underlying theory. On the basis of current evidence, a single theory is probably not sufficient to explain how cardiac massage produces blood flow. This suggests that different simultaneous mechanism might be involved. The relative importance of these mechanisms depends on several factors, including delay from collapse to starting of resuscitation, compression force and rate, body habitus, airway pressure, and presenting electrocardiogram. The complexity of the physiologic events occurring during cardiopulmonary resuscitation, together with the need of adequate training for a correct and prompt utilization of mechanical devices, might also partially explain the disappointing results of these devices in most clinical studies.
Introduction
Two different competing theories have been classically proposed to explain how precordial compressions produce forward flow during closed-chest cardiopulmonary resuscitation (CPR). 1 The “cardiac pump theory” hypothesizes that blood flows during compression because the heart is directly squeezed between the spine and the sternum. 2 On the other hand, the “thoracic pump” theory postulates that forward blood flow occurs because intrathoracic pressure during compression exceeds extrathoracic vascular pressure, so that the blood is forced to flow from the thoracic to the systemic vessels, with the heart acting as a passive conduit rather than as a pump. 3 More recently, the evidence that the two standard theories cannot fully explain the mechanism of generating flow in all patients led to the development of newer theories, i.e. the “lung pump”, the “left atrial pump”, and the “respiratory pump”.4–7
The efficiency of chest compressions is a key determinant of CPR success, irrespective of the underlying theory. In this regard, the idea of using mechanical devices to improve the efficiency of cardiac massage was tested in both physiologic and clinical studies during the previous decades. In this paper, we reviewed the studies supporting the different theories for blood flow maintenance during manual CPR and those exploring the potential clinical utility of mechanical devices for cardiac massage.
The cardiac pump theory
The first attempt to explain how cardiac massage works during CPR was made more than half a century ago. Kouwenhoven et al.
8
hypothesized that blood flow during cardiac massage is directly produced by the compression of both ventricles and by the resulting rise in intraventricular pressure, whereas ventricular filling is allowed by a passive “diastolic” suction mechanism given by the reduction in the intraventricular pressure during release. As a result, during compression, the atrioventricular valves close, and the aortic and pulmonary valves open when the intraventricular pressures exceed the aortic and pulmonary diastolic pressures. During release, the intraventricular pressures rapidly fall, so that the atrioventricular valves open – allowing blood flow into the ventricular cavities – and the aortic and pulmonary valves close (Figure 1(a)). This theory also requires that significant changes in ventricular sizes occur during CPR, resembling the systolic squeezing and the diastolic relaxation of a normal cardiac cycle.
Main theories on blood flow production and maintenance during cardiac massage. (a) In the cardiac pump theory, during compression, the mitral valve closes (white arrows), whereas the aortic valve opens (red arrows) when the intraventricular pressure exceeds aortic diastolic pressure. During release, the aortic valve closes and the mitral valve opens, allowing “diastolic” filling. Similar changes can be seen in right-sided cardiac valves. (b) In the thoracic pump theory, during compression the intrathoracic pressure increases and forces blood from the thoracic vessels into the systemic circulation, with the heart acting as a conduit and not as a pump. Thus, a venous-arterial pressure gradient develops, leading to antegrade blood flow through the atrioventricular valves and the aortic and pulmonary valves during compression. This theory requires the mitral valve to be open throughout the whole cardiac cycle (white arrows) and implies minimal changes in ventricular volumes. (c–e) Main principles of newer theories, based on the heart as part of a larger pumping system (lung theory), or on pathophysiological variants of the thoracic pump (left atrial and respiratory theories).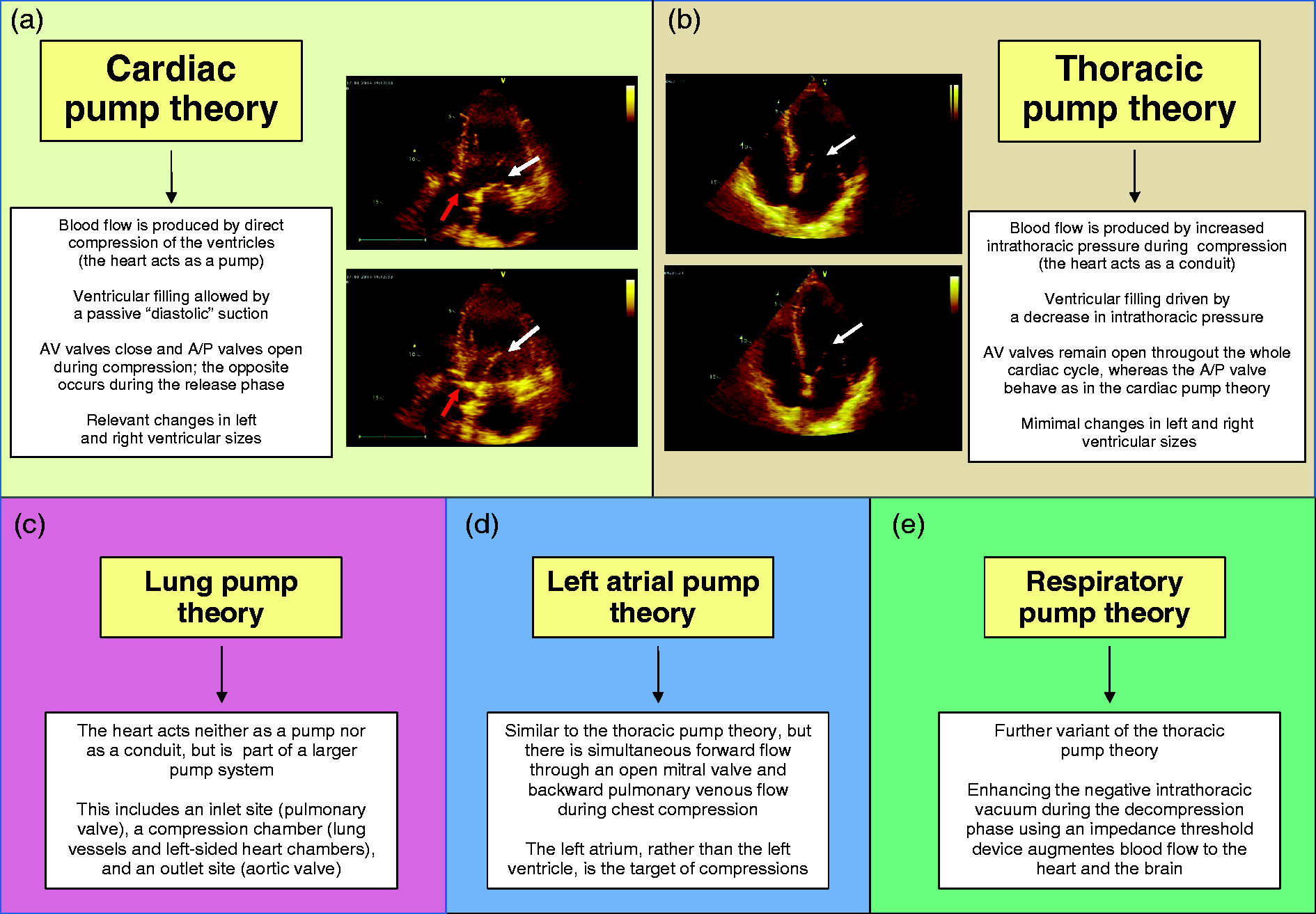
Subsequent observations have supported this theory (Table 1). In a dog model, Maier et al. found that increasing compression rate – but not compression force – at constant stroke volume led to an increase in cardiac output and coronary blood flow, suggesting that direct cardiac compression was the major determinant of stroke volume. 9 In another study carried out in dogs, the mitral valve was found to be closed during the compression phase and open during the release phase. 10 It must be considered that the relevance of animal studies, and especially dogs, about chest compression is poor and questionable because of the different anatomy and pathophysiology from humans. Further studies performed using transesophageal echocardiography observed mitral valve closure with ventricular cavity size reduction during chest compression and mitral valve opening during the release phase, supporting the cardiac pump theory.11–13 More recently, Kim et al. 14 performed contrast transesophageal echocardiography in 10 patients with non-traumatic cardiac arrest. After injection of agitated saline into the left ventricle by a pigtail catheter, retrograde blood flow toward the left atrium and antegrade blood flow toward the aorta from the left ventricle during the compression phase of CPR was observed in all cases. After injection of agitated saline into the aortic root, there was progressive anterograde clearance of contrast bubbles with successive chest compressions, and only a small amount of contrast entered the left ventricle when compressions were interrupted. In each CPR cycle, the mitral valve closed during compression and opened during relaxation. Moreover, the aortic valve opened during compression and closed during relaxation, in accordance with the hypothesis that the left ventricle acted like a pump during external chest compressions. However, there were significant inter-individual variations in the degree of retrograde blood flow, suggesting that other mechanisms might have significantly contributed to blood flow.
The thoracic pump theory
In the early 1980s, some studies proposed a different explanation for the mechanism leading to blood flow during CPR.15,16 According to this alternative theory, blood flow does not occur by direct cardiac compression, but rather by a thoracic pump mechanism. Increased intrathoracic pressure during compression forces blood from the thoracic vessels into the systemic circulation, with the heart acting as a conduit and not as a pump. The compression leads to a uniform pressure rise within the whole intrathoracic compartment, and retrograde venous flow is inhibited by the collapse of veins at the thoracic inlet and by venous valvular closure as well. This theory requires the mitral valve to remain open throughout the whole cardiac cycle, and ventricular sizes to show minimal changes during CPR (Figure 1(b)).
Several observations provided support to this theory. A case report described that repetitive coughing of a patient experiencing ventricular fibrillation in the catheterization laboratory maintained blood flow and consciousness for as long as 40 s without any external compression. 17 In another case series, 18 conventional CPR was performed in two patients who had flail chests secondary to trauma which led to cardiac arrest. Although CPR could not generate any measurable arterial blood pressure fluctuations, as the sternum continuity was repaired – thus preventing any abnormal expansion of the chest – a measurable arterial blood pressure rise occurred, synchronous with each compression. Porter et al. 19 reported two distinct patient groups during closed-chest CPR, one matching the cardiac pump theory and the other group showing mitral valve opening by transesophageal echocardiography during chest compression, further supporting the thoracic pump theory. Interestingly, this study found that the patients whose mitral valves were open during chest compression showed lower forward trans-mitral flow and worse clinical outcome compared to the group where mitral valve closed during chest compression.
Newer hypotheses
The lung pump theory
More recently, other observations suggested that the cardiac and thoracic pump hypotheses alone cannot fully explain the mechanism of generating blood flow. Shaw et al. 4 introduced the concept of “lung pump” (Figure 1(c)). In this model, the heart is part of a pump that is composed of three components: an inlet valve, a compression chamber, and an outlet valve. The inlet valve is represented by the pulmonary valve, the compression chamber by the lung vasculature and the left atrial and ventricular chambers, and the outlet valve by the aortic valve. As a result, the heart is neither a pump nor a passive conduit as described by the cardiac or thoracic pump hypotheses, but rather an essential part of a larger pumping system. During chest compression, there is a rise in intrathoracic pressure which is transmitted equally to all intrathoracic structures. Although a minimal quantity of blood can flow backward from the pulmonary artery into the right ventricle and systemic veins until the closure of pulmonary valve occurs, the remaining blood must necessarily exit via the left chambers and the aortic valve. During relaxation, the intrathoracic pressure falls below that of the extrathoracic vasculature, blood flows into the thorax via the systemic veins, and pulmonary vascular volume is restored from right chamber blood flow.
The left atrial pump theory
Ma et al. 5 proposed the concept of “left atrial pump”, based on the evidence of simultaneous forward flow through an open mitral valve and backward pulmonary venous flow during chest compression in some patients. In this theory, the left atrium, rather than the left ventricle, is the main target of compressions (Figure 1(d)). The authors also noted that the timing from cardiovascular collapse to CPR was a major determinant of the pump mechanism observed. Shorter times were associated with the cardiac pump mechanism and longer times with the thoracic or left atrial pump mechanism. This was interpreted as the effect of the delay in starting CPR, which might change the compliance of the lungs and the heart and then alter the mechanism of compression. 6 This suggests that, during the late stages of resuscitation, a thoracic pump mechanism might be the major determinant of forward blood flow because of a relatively stiff myocardium.
The respiratory pump theory
Interestingly, in a recent paper from Convertino et al., 7 the concept of “respiratory pump” – another variant of the thoracic pump – was introduced (Figure 1(e)). In patients with cardiac arrest receiving CPR, enhancing the negative intrathoracic vacuum during the decompression phase with inspiratory resistance using an impedance threshold device (ITD) augmented blood flow to the heart and the brain. The cardiopulmonary interactions generated in this fashion were similar to those in spontaneously breathing patients. Each time the chest wall recoiled, there was an immediate decrease in intrathoracic pressure, enhancing blood flow back to the heart. This study might suggest that optimizing the thoracic pump during the compression and decompression phases of CPR could lead to an increase in vital organ blood flow.
Considering all the studies on cardiac massage mechanism, particularly those based on contrast transesophageal echocardiography,11–14 we speculate that either the cardiac pump theory or a combination of the cardiac pump and thoracic pump theory might represent the most realistic mechanism of forward flow into the aorta during CPR in humans. The cardiac pump theory is likely to be the main mechanism during the initial phases of CPR. The contribution of the thoracic pump mechanism probably increases during resuscitation, becoming relevant in prolonged CPR. While intriguing from a pathophysiological point of view, the clinical relevance of the remaining theories remains to be demonstrated, although it is likely that they could play a role in specific cases.
Mechanisms for chest compression devices
Rationale for mechanical chest compression
Survival in subjects with cardiac arrest is related to the amount of blood flow generated to the heart and brain during CPR. Manual chest compressions are often performed incorrectly, especially during transportation. In this regard, it could be hypothesized that automated devices may eliminate the variability and fatigue inherent in manual CPR, decrease interruptions, augment airway mechanism and improve blood flow and survival. 20 To date, three different classes of mechanical devices have been proposed: mechanical piston, load-distributing band, and active compression–decompression (ACD) devices.
Mechanical piston devices
These devices are based on a simple piston mechanic, provided by a compressed gas- or an electric-powered plunger placed over the sternum. Since sternal compressions are localized and not coupled with any active mechanic decompression, the potential efficacy of these devices mostly hinges on the pathophysiological hypotheses underlying the cardiac pump theory, under the assumption that the mechanical piston could allow a better compression of the left and right ventricle when compared to manual CPR. The first attempt of a piston device was made in 1908 by Pike et al., 21 who observed no benefit as compared with manual methods. During the successive decades, several devices of this type were proposed.22,23 Taylor et al. 24 used a pneumatic device (Thumper by Michigan Instruments), randomizing 50 patients to mechanical or manual CPR. Mechanical CPR was found to be comparable to manual CPR only when performed in specific conditions, i.e. when trained personnel were not readily available or where manual compression was technically difficult to perform. Moreover, an increase in sternal fractures in the Thumper group was found. Two successive small randomized controlled trials found no differences in survival between patients assigned to CPR using the Thumper device and those assigned to standard CPR.25,26 In both of these studies, no patient survived to hospital discharge.
The current version of the Thumper device (Figure 2(a)) is able to provide 100 chest compressions per minute, with adjustable stroke range and exponential compression waveform to optimize efficiency. However, the results of clinical studies provided inconsistent results. During electrically induced ventricular fibrillation in pigs, the Thumper device was shown to raise coronary perfusion pressures as much as vasopressor drugs.
27
On the other hand, in a prospective study carried out using a digital video-recording system set up in ambulances, Wang et al.
28
showed that CPR by a Thumper device had similar no-chest compression interval and lower average chest compression rate and average ventilation rate than manual CPR, suggesting that the advantage of lower no-chest compression intervals after activation of the device was counterbalanced by a larger time to deploy in a system with short transport time.
Principal mechanical devices: Thumper (a), Auto-Pulse load-distributing band (b), CardioPump (c), Lifestick (d), and LUCAS (e).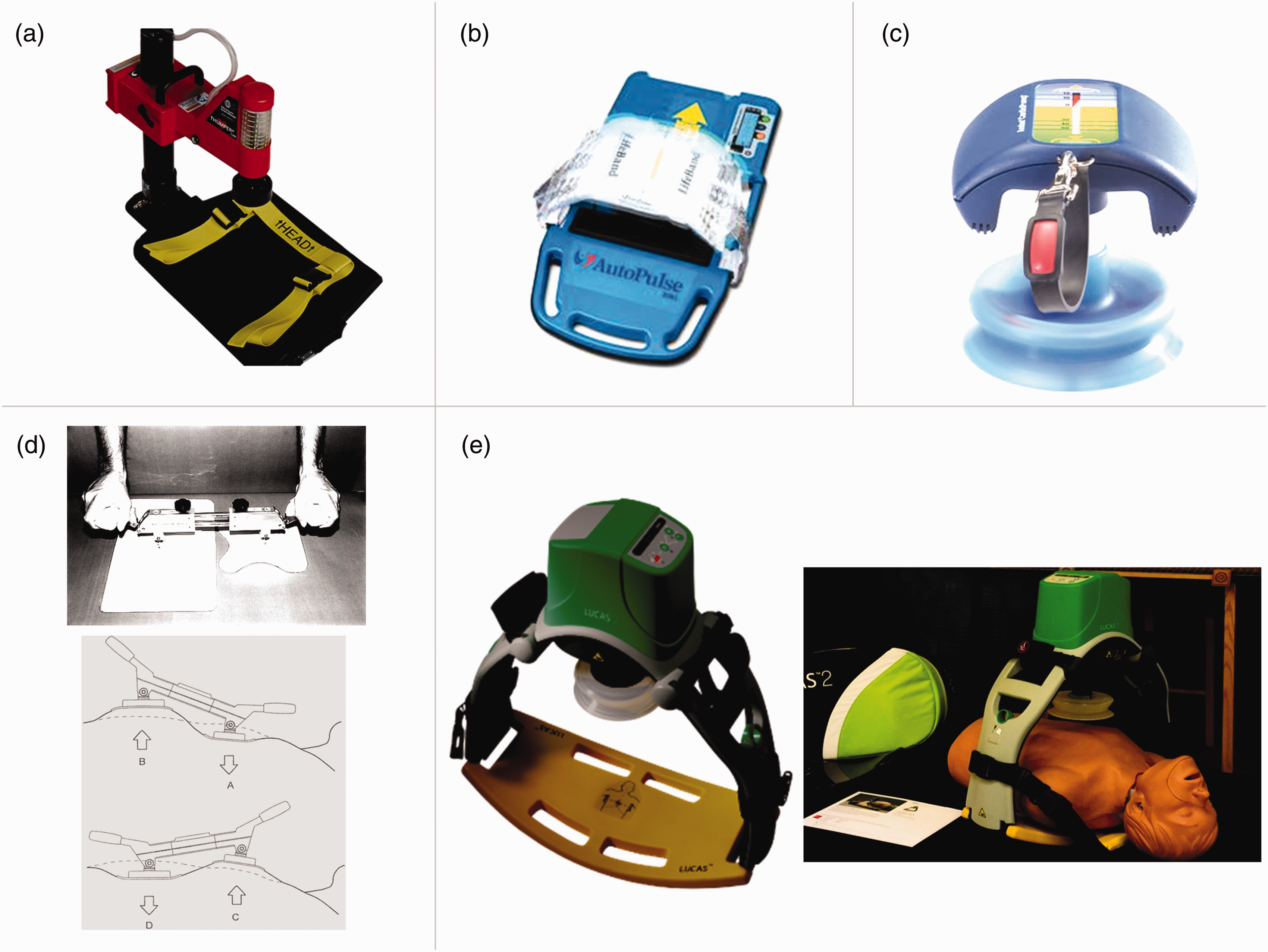
Load-distributing band devices
After 1980, a new mechanical device design, known as the CPR vest, was introduced. 29 This device was based on pathophysiological principles that hinged on the thoracic pump theory, according to the idea that a compression device composed of a chest-constricting band, creating a load-distributing system, could produce higher blood flow compared to CPR consisting of sternal compressions only. The vest was designed to be positioned around the patient’s thorax, and rapidly inflated and deflated. A similar principle was successively followed to develop a more flexible version, the Auto-Pulse CPR load-distributing band (Figure 2(b)). Despite initial encouraging results,30,31 successive studies did not confirm the clinical utility of these devices. 32 In the large multicenter ASPIRE trial on patients with out-of-hospital cardiac arrest (OHCA), the use of the Auto-Pulse CPR was associated with worse neurological outcomes and a trend toward worse four-hour survival. 33 In the randomized Circulation Improving Resuscitation Care trial, which enrolled 4573 OHCA patients, the Auto-Pulse yielded an equivalent survival to hospital discharge, with no difference in neurologic status at discharge when compared with manual CPR. 34
Active ACD devices
The rationale of the ACD approach is that an active decompression – obtained by a suction cup that lifts the anterior chest during the decompression phase and creates a negative intrathoracic pressure – might favor venous return to the heart when added to the standard compression mechanic. 35 This hypothesis is consistent with the thoracic pump model, as the efficacy of the compression would be increased by the augmented venous return during the decompression phase.36,37 The ACD principle firstly resulted in two different devices called the ResQpump and the CardioPump (Figure 2(c)). These devices required both pushing and pulling and were found to be more physically demanding for the rescuer than performing standard CPR. 38 Again, their clinical application yielded conflicting results. Some clinical studies showed a higher short-term survival compared with conventional CPR.39,40 In the French Active Compression-Decompression Cardiopulmonary Resuscitation Study, 41 a randomized trial on patients with OHCA, CardioPump CPR was associated with higher rate of hospital discharge without neurologic impairment and better one-year survival rate as compared to manual CPR. However, a number of large prospective randomized clinical trials, comparing ACD-CPR to conventional CPR both in patients with OHCA and those with in-hospital cardiac arrest, found no difference in survival.42–48
Two other mechanical devices based on the ACD principle are the Lifestick and the Lund University Cardiopulmonary Assistance System (LUCAS). The Lifestick is a hand-held device able to provide a phased thoracic–abdominal compression–decompression sequence (Figure 2(d)). 49 A prospective randomized clinical study of OHCA patients demonstrated no difference in survival to hospital discharge with use of this device as compared to conventional CPR. 50 The LUCAS is an easy-to-handle, gas-driven or electric-powered device that includes a pneumatic cylinder mounted on two legs, connected to a stiff back plate, and a silicon rubber suction cup that attaches to the sternum and returns the sternum to the starting position when it retracts (Figure 2(e)). The device was shown to provide a higher rate of adequate compressions and decreased total hands-off time as compared to manual CPR in pre-hospital cardiac arrest scenarios. 51 Successively, two large trials on OHCA patients, the LUCAS in Cardiac Arrest (LINC) and the Prehospital Randomised Assessment of a Mechanical Compression Device in Cardiac Arrest (PARAMEDIC) trials, found no benefit for mechanical CPR over manual CPR in terms of both early and late survival.52,53 Moreover, in the PARAMEDIC population, the mechanical CPR group showed a lower probability of survival without significant neurological impairment at three months than the manual CPR group. 54 In 2002, a Cochrane meta-analysis of several studies showed no difference in survival or neurological outcome comparing ACD-CPR to conventional CPR. 55 A more recent meta-analysis found that ACD resuscitation is not able to improve the return to spontaneous circulation, although its efficacy could be somewhat increased by two important prognostic factors, namely witnessed status and low response time. 56 Recently, a multicenter randomized controlled trial on patients with OHCA of cardiac origin reported a significant improvement in both survival and neurological outcome over standard CPR using the combination of LUCAS with an ITD, a pressure-sensitive valve that limits air entry into the lungs during the decompression phase.57,58
Current recommendations
Main studies exploring the mechanisms of blood flow during cardiopulmonary resuscitation.
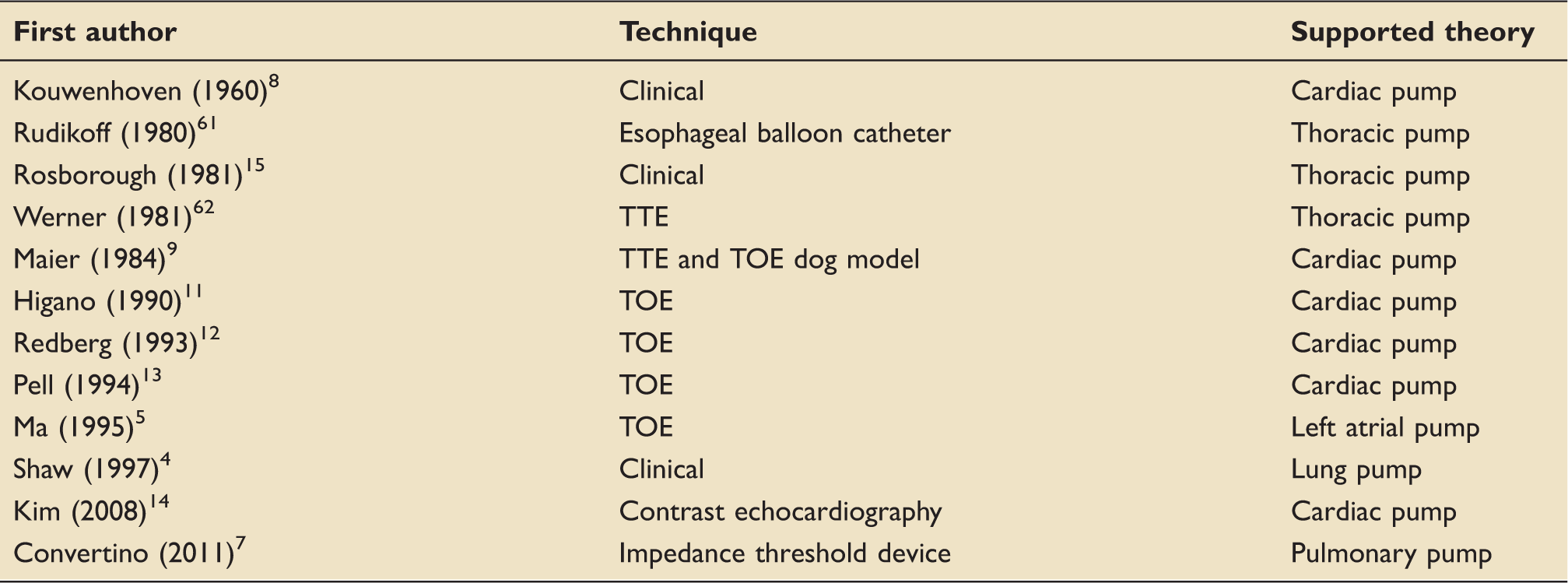
TOE: transesophageal echocardiography; TTE: transthoracic echocardiography.
Principal studies comparing clinical outcome between out-of-hospital cardiac arrest patients treated by mechanical vs. manual cardiopulmonary resuscitation (CPR).
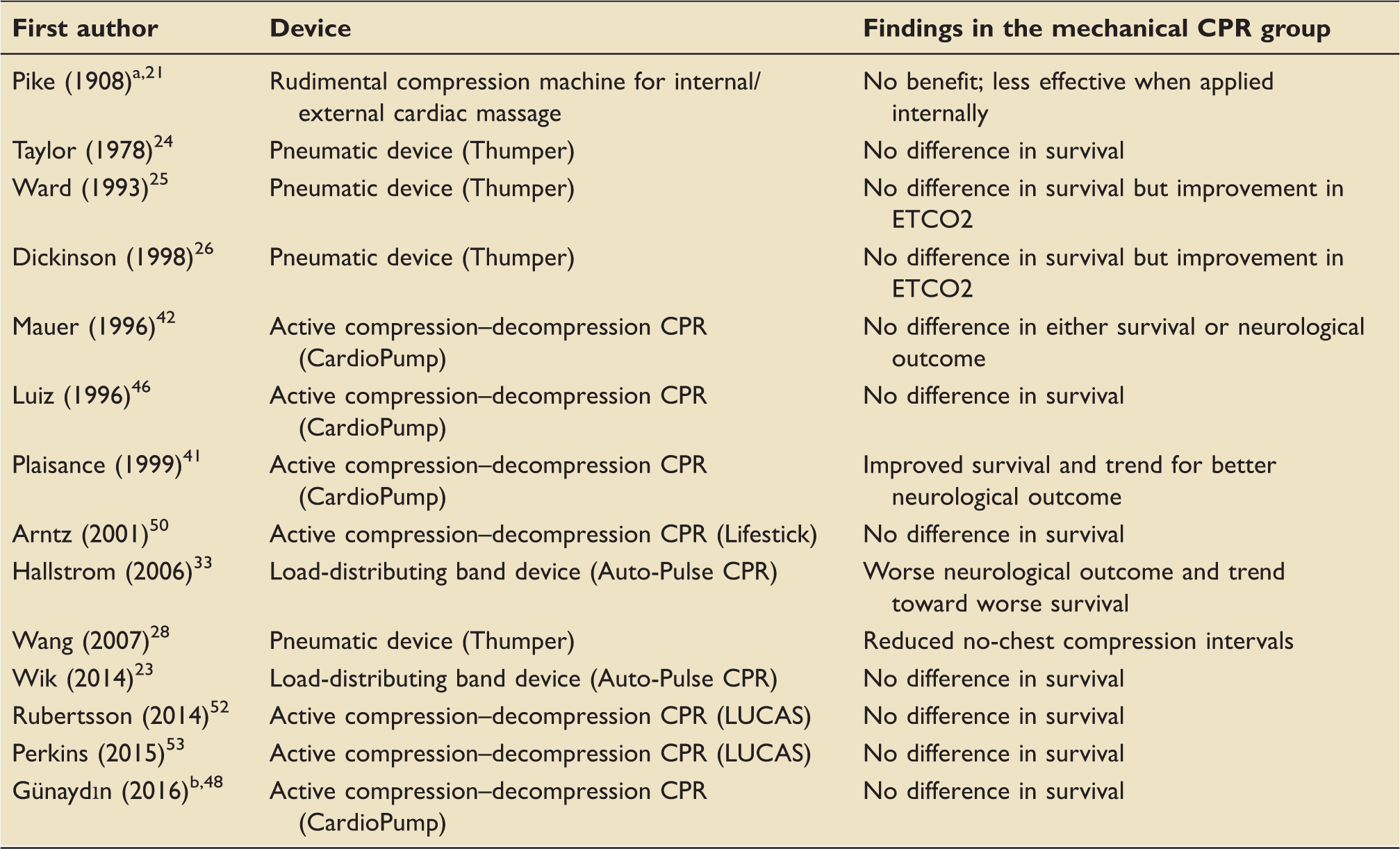
CPR: cardiopulmonary resuscitation; ETCO2: end-tidal CO2; LUCAS: Lund University Cardiopulmonary Assistance System.
Study performed on animals.
Study including both out-of-hospital and in-hospital cardiac arrest patients.
Conclusion
Based on current evidence, a single theory is probably not sufficient to explain the development and maintenance of forward blood flow during CPR in each patient. The cardiac pump theory and thoracic pump theory seem to be more supportable and convincing, and probably represent the main mechanisms in the initial and late stages of CPR, respectively. However, it is likely that other mechanisms could be involved in particular cases, and that the relative contribution of each to the efficiency of cardiac massage depends on a complex interaction between clinical and pathophysiological factors. Among these, age, body habitus, thoracic flexibility, possible artificial ventilation, cardiac chambers stiffness and size, delay from cardiovascular collapse to starting of CPR, compression force and rate, airway pressure, early or late CPR, and presenting electrocardiogram may ultimately influence the predominant pump mechanism at work in each specific case. For instance, if the left atrial size is huge, the left atrial pump theory might be more important for this specific case. Perhaps, we might get to the bottom of this multi-theory problem observing blood flow and valve movement by repeated contrast-enhanced echocardiography investigations during CPR in humans in different clinical contexts. The complexity of these mechanisms, combined with the need of adequate training in order to correctly utilize a mechanical device in emergency settings, may also probably explain the poor efficacy of mechanical devices in the majority of clinical studies on patients with OHCA. Although some studies suggest a potential role of mechanical CPR to improve outcomes in the setting of IHCA, to date the level of evidence is low. Until new studies provide further information about the utility of CPR devices, it is reasonable to consider mechanical CPR only in settings where adequate manual CPR is challenging or dangerous for the provider.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.