
Abstract
The use of medication to support patients and optimise outcomes is a fundamental strand of care. Pharmacists provide a key role managing medication within the complexity of various routes of administration, severe and rapidly shifting pharmacokinetic and dynamic parameters, and extremes of physiology in critical illness. Pharmacists intercept and resolve medication errors, optimise medication therapy and undertake broader professional activities within the job role that contribute to the smooth running of ICU. These activities are associated with improved quality, reduced mortality and reduced costs.
Introduction
The use of medication to support patients and optimise outcomes is a fundamental strand of care. The complexities posed by altered routes of administration, severe and rapidly shifting pharmacokinetic and dynamic parameters, combined with extremes of physiology in critical illness demand close scrutiny and careful management of drug therapy. Pharmacists provide a key role within the critical care multi-professional team in managing this aspect of therapy.
Training
An overview of the training path in the United Kingdom (UK) is shown in Figure 1.1–3 Newly qualified pharmacists receive five years of training before examination and registration with the General Pharmaceutical Council, the majority enter community pharmacy with only 10–15% opting to go into hospital. Several years of foundation training are required to acquire experience across a broad range of pharmacy activities including fundamental clinical training, manufacturing (parenteral nutrition, chemotherapy, etc.), medicines information services, governance, medicines law, supply chain handling, formulary and patient services (dispensary, patient information hotlines, etc.). Hospital pharmacists then begin to major in specific aspects of practice with many concentrating on ward pharmacy over other activities such as aseptics or medicines information.
An overview of pharmacists training path, milestones and professional activities at each level.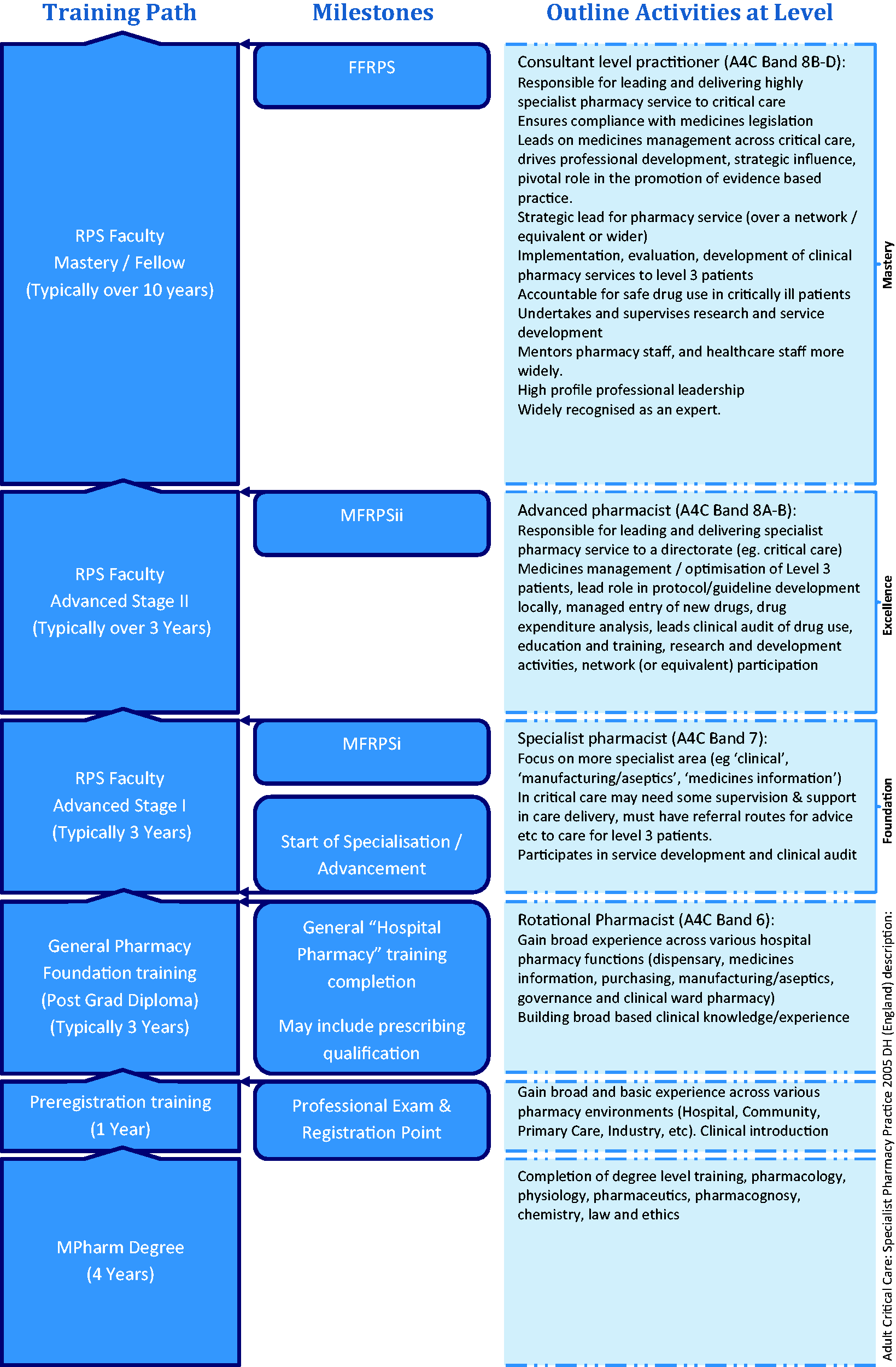
Those interested in progressing in critical care spend time in the area, link up with peers for support and advice, engage with the Royal Pharmaceutical Society’s (RPS) Faculty process and participate in education events such as those by the United Kingdom Clinical Pharmacy Association. A competency framework has been published, 2 though the terminology used has recently changed with ‘Foundation level’ competencies now termed ‘Advanced Stage I’ within the RPS Faculty. This was to accommodate a new general pharmacy foundation framework for the first three years of practice, filling the gap between registration and commencement of advanced practice.
Several postgraduate general clinical pharmacy courses exist, but with variation in critical care components ranging from a few lectures to several-month clerkships/clinical attachments. Most advanced training is self-directed, with attainment of level of competence independently verified through the RPS Faculty system. 1 Supporting systems such as face-to-face peer discussion, mentorship and work-based learning are practitioner development tools that need expansion and formalising to optimise the pharmacist’s skills. 4 Some of this is required by the revalidation for pharmacy professionals process which formally starts in 2018. 5
A high proportion of critical care pharmacists are also prescribers, 6 and this is set to become a standard feature. 7
Historical perspective
Pharmacists became involved in critical care in the USA starting in the 1960s followed by studies linking the role with improved outcomes and reduced costs. 8 Sporadic involvement in the UK health system developed from ward pharmacy and PN/nutrition teams in the 1990s towards a more overt in-depth role formally described by the NHS Modernisation Agency in 2002. 9 ‘Adult Critical Care: Specialist Pharmacy Practice’ was published by DH (England) in 2005 and very clearly articulated roles and responsibilities with a competency framework. 2 The publication of ‘Core standards for intensive care units’ in 2013 and subsequent incorporation into ‘Guidelines for the Provision of Intensive Care Services’ in 2016 has further cemented this.10,11 Now clinical pharmacy services are expected to transform into 7/7 coverage for high-risk patients and have better integration into the multi-professional team. 12 The Carter report in England 2016 called for more clinical pharmacists to be deployed on wards due to improved medicines optimisation and to serve the Getting-it-Right-First-Time agenda. 7 Pharmacists can now be identified on 98.6% of critical care units across the United Kingdom. 13
Current impact in critical care
Pharmacists see the entire casemix and so must manage the pharmaceutical care of an extreme range of health problems, as well as quickly assimilate information and management paths for conditions they may not have seen before. Frequently, this can mean making judgements about therapies where there is no evidence, where evidence is contradictory or where there are opposing therapeutic goals. Pharmacists are healthcare scientists and use their underpinning training to good effect in such circumstances.
Optimising medication is a central and key role expected of pharmacists in all clinical areas, not only in critical care. 14 They intercept a large number of prescribing errors, the majority of which have potential for moderate to severe clinical impact. The error rate picked up in ICU runs at a slightly lower rate than in the wider hospital population (6.8% versus 7.5–8.9%), but in addition to this activity pharmacists provide high optimisation rates (8.3%).15–17 Clinical impact gradings of critical care pharmacist activity in terms of error intercepts and optimisation activity have been verified by a 30-strong multi-professional panel. 18
Pharmacist’s activity can generally be grouped into three broad areas. 13 First, the pharmacist’s independent review occurs when reviewing charts, clinical data, performing medicines reconciliation, etc. as a specific pharmacy activity that has grown out of the traditional ‘ward pharmacy’ model and undertaken in almost all UK ICUs. 13
Second, there is active participation in the daily multidisciplinary team (MDT) round, where the pharmacist rounds with the team, the patients are reviewed and plans are drawn up for the day’s activities and for longer term planning. In a UK study, almost 60% of pharmacist’s contributions are made during the MDT round. 16
The third main area is broadly grouped as ‘professional support activity’ and includes guideline development, formulary applications, governance and incident reviews, financial reporting and forecasting, teaching, audit and research. Many functions grouped under this unit wide activity are associated with reduced mortality in US hospitals and contribute to the smooth running of the ICU. 19
The cost of employing a pharmacist at the recommended minimum staffing level is approximately £20 per patient per day. Several studies find that the role reduces overall expenditure through more efficient use of medicines and the avoidance of direct costs of iatrogenic harm, with additional savings made from avoiding payouts arising from damages claims.20–23 Recently, further cost reductions have been shown due to closer adherence to standardised care, 24 and in the UK replacing an existing ‘ward pharmacy’ type service with embedded critical care trained pharmacists who attend the daily MDT round further reduced direct medicines costs by £17 per patient bed day (£175,275 per annum). 25
Overall, pharmacists have been shown to improve the quality of critical care through medicines optimisation, medication error interception and greater regard to standardised therapy whilst reducing medication and care costs.
Future perspectives
Whilst pharmacists are increasingly embedded into critical care MDTs, significant challenges to the routine delivery of this proven resource exist. Many ICUs do not have pharmacists with the right experience level or who have the minimum required job time resulting in a poor or absent weekend pharmacy service, lack of attendance at ward round and impaired provision of good governance, guidelines, understanding of budgets and prescribing patterns. 13 A national training programme is required to ensure we can meet the demand for advanced-level critical care pharmacists. 26 Staffing models for delivery of true seven day services need further strategic development.
With greater availability comes an enhanced training capability around medicines accessible to all healthcare staff, be that for existing roles such as in medicine, nursing, physiotherapy, etc., or in evolving roles such as advanced critical care practitioners.
Pharmacy technicians (a regulated pharmacy profession) and assistants could be added to the critical care workforce. They will manage aspects of the medicines supply chain, logistics and provision of various kits (intubation, transfer bags, resus trolleys, etc.) and in so doing release nursing time back to doing actual critical care nursing. There are already pilots of pharmacy technicians preparing and administering medicines underway to reduce delayed and omitted doses, they may release nurse time back to other care activities.27,28 This could be extended to critical care where nursing time is at a premium and where high-risk medication preparation occurring at bed sides is common.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.