
Abstract
Background
Critical care services underpin the delivery of many types of secondary care, and there is increasing focus on how to best deliver such services. The aim of this study was to investigate the impact of establishing a medical high dependency unit, in a tertiary referral center, on the workload, case mix, and mortality of the intensive care unit.
Methods
Single-center, 11-year retrospective study of patients admitted to the general intensive care unit, before and after the opening of the medical high dependency unit, using interrupted time series methodology.
Results
Over the duration of the study period, 3209 medical patients were admitted to the intensive care unit. There was a constant rate of medical admissions to the intensive care unit until the opening of the medical high dependency unit, followed by a statistically significant decline thereafter. There was a statistically significant decrease in the average severity of illness of medical patients prior to the opening of the medical high dependency unit, but there was no evidence of a change following the opening of the unit. There was no evidence of a statistically significant change in the estimated mean standardized mortality ratio for either medical or surgical admissions after the intervention.
Conclusions
The opening of a medical high dependency unit had a minimal impact on the intensive care unit. There was, in all likelihood, an unmet need—of less seriously ill patients, who were previously looked after on a normal ward, but did not require intensive care unit admission—who are now cared for in the new medical high dependency unit. Interrupted time series analysis, although not without limitations, is a useful mean of evaluating changes in service delivery.
Introduction
Critical care services underpin the delivery of many types of secondary care,1,2 and thus have an important role in ensuring the efficient operation of hospitals. Critical care is also resource-intensive, costing the National Health Service in England approximately £1bn per year. 2 As a result, there is increasing interest in how to best deliver these services and the impact of reconfigurations. 3
The needs of critically ill patients are often stratified into levels of care.2,4 In the United Kingdom, level 3 care is defined as the need for invasive respiratory support, or support of two or more failing organ systems, and is usually provided in intensive care units (ICUs). Level 2 care is defined as the need for single organ system monitoring and support, and is often provided in high dependency units (HDUs).2,5 High dependency care for patients with non-surgical diagnoses has long lagged behind that of surgical patients, but increasing recognition of the need for an intermediate level, between ward-based and ICU-based care, has prompted the development of specialist medical high dependency units (MHDUs, sometimes also known as intermediate care units) in many hospitals. 6
Previous studies of establishing high dependency or intermediate care units have focused on multidisciplinary models of care.7,8 The impact of establishing a dedicated MHDU has not been investigated in detail. It is conceivable that the establishment of an MHDU could result in a decrease in the number of medical patients admitted to the ICU, because less severely ill patients are now admitted to the MHDU instead. Such a change might be accompanied by an increase in the average illness severity of the medical patients who are admitted to the ICU, and possibly also a change in crude, but perhaps not case-mix-adjusted mortality. On the other hand, it is possible that a new MHDU might serve an unrecognized need, in that less severely ill patients, who were previously looked after on normal medical wards, without ever coming to the ICU, are now housed elsewhere. As a result, the impact on the ICU might be minimal. These changes in patient flow are of key importance to the planning and delivery of services, as well as the analysis of outcomes, but have not been studied in detail. Furthermore, many previous studies have adopted simple before/after comparisons,7,8 which may not be appropriate when there are underlying secular trends. 9
Aberdeen Royal Infirmary is a university hospital and tertiary referral center in the North of Scotland, which recently established an MHDU, separate from existing surgical HDUs, and the general and cardiothoracic ICUs. The aim of this study was to investigate the impact of the MHDU on the workload, case mix, and mortality of the ICU. Our objectives were to answer the following three research questions: (1) Has the opening of the MHDU impacted on the number of medical patients admitted to the ICU? (2) Has the opening of the MHDU impacted on the severity of illness of medical patients admitted to the ICU? (3) Has the opening of the MHDU impacted on the crude and case-mix-adjusted mortality number of medical patients admitted to the ICU?
Methods
Study design
This is a retrospective study of patients admitted to the general ICU at Aberdeen Royal Infirmary before and after the opening of the MHDU, using interrupted time series methodology.
Setting and intervention
Aberdeen Royal Infirmary is a 900-bed university hospital. Critical care services comprise a general medical/surgical ICU (16 beds), cardiothoracic ICU (6 beds), several surgical HDUs, and (since December 2012), a dedicated 10-bedded MHDU. The MHDU provides a greater numbers of nurses, in a ratio of one nurse to two patients. The nursing staff also have greater experience in the management of patients with critical illness, as compared to routine ward-based nurses. In addition to higher levels of nursing care, invasive monitoring, non-invasive respiratory support, and limited vasoactive drug treatment are provided. The unit took three months to become fully operational, and we therefore included a three-month “wash-out” period in our model. The intervention was defined as the opening of the MHDU, which took place from December 2012 until February 2013.
Data source and case definition
Data were obtained from the locally held WardWatcher™ (Critical Care Audit Ltd, Yorkshire, UK) audit database, which forms part of the Scottish Intensive Care Society Audit Group’s national audit programme and records demographic and clinical details on all patients admitted to ICUs in Scotland. Data were extracted on all patients who were admitted to the general ICU at Aberdeen Royal Infirmary, between 1 January 2005 and 31 December 2015, including date of admission, gender, age, illness severity (APACHE II [Acute Physiology and Chronic Health Evaluation] acute physiology score) and APACHE II predicted mortality, whether the patient was referred by a medical or surgical service, and status on discharge from hospital (alive or deceased). Data on surgical patients were included for comparison purposes. Patients who were readmitted to the ICU and those under the age of 16 were excluded. Those excluded from APACHE II scoring, were excluded from all but the sensitivity analyses. We also obtained data on the number of patients admitted to the MHDU, following its opening, from the hospital’s patient administration system. Detailed demographic and clinical data are not presently recorded for patients admitted to the MHDU.
Statistical analysis
The statistical analysis was conducted using both SPSS 24 (IBM Corp. Released 2016. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY: IBM Corp.) and STATA 14 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP.). Data were amalgamated to provide monthly total counts of patients admitted, counts of observed and expected deaths, and average severity. Descriptive statistics of the monthly counts of patients admitted were presented overall, and before and after the intervention.
Given the temporal nature of the data, and the potential presence of secular trends, interrupted time series methodology was used. Two approaches were used to evaluate whether there had been a change in the outcome under consideration, e.g. counts of admissions. Both allowed first-order autocorrelation—dependence between successive values. The first was an autoregressive integrated moving average regression model that allowed investigation of seasonal patterns alongside other parameters. Pairs of sine and cosine terms were introduced to the model to allow for seasonal effects (within procedure circular in STATA). This was followed by an interrupted time series Prais Winsten regression model through itsa procedure in STATA. This procedure allowed flexibility on the use of multiple intervention times, here used to represent the intervention and the end of the wash-out period, with changes in level and slope at each point, but had limitations on the inclusion of other structures.
Application to research questions
Research question 1 was investigated by evaluating and modeling the number of medical patients admitted to the ICU before and after the establishment of the MHDU. As a sensitivity analysis, daily counts of admissions were modeled with a negative binomial distribution to account for weekly as well as seasonal patterns using sine and cosine terms. Research question 2 was investigated by modeling the monthly mean APACHE II score of patients admitted. Research question 3 considered crude mortality by modeling the proportion of patients dying within each month and case-mix-adjusted mortality by modeling the standardized mortality ratio (SMR). Monthly SMRs were calculated using monthly counts of observed deaths and monthly counts of admissions with APACHE II mortality prediction >50% (expected deaths). 95% confidence intervals for the SMR were calculated using standard methods based on Poisson distributions.10,11
Results
Study population
The derivation of the study population is shown in Figure 1. In total, 7571 patients were admitted to the ICU between 2005 and 2015. Of these, 3382 were medical and 4189 surgical patients. A number of patients were excluded, on the basis of no APACHE II score being available. The reasons were as follows: 124 were excluded from scoring, 4 had incomplete data, 18 had no appropriate diagnosis recorded, 10 lacked detailed of the nature of the operation undertaken, and 191 had an unknown length of stay, or a stay of less than 8 h. In total, 11 patients (six medical and five surgical) were excluded from all analyses due to being aged <16 years. Three hundred and eighty-two patients (173 medical and 209 surgical) were excluded from complete case analyses due to being aged <16, having no APACHE II score or having no hospital outcome, leaving 7189 patients (3209 medical and 3980 surgical, Table 1). An assessment of the percentage of missing data, by month, in those aged 16 years or older, revealed considerable variation ranging from 0 to 22%. In years 2005–2008, Apache II score was missing for less than 2% of patients; in 2009–2011, 7%; and 2012–2015 around 5%. However, no pattern could be identified until the final two months of the study, which had 17 and 44% missing data (dominated by missing hospital outcome, 11 and 39%, respectively). A sensitivity analysis imputing missing APACHE II score and APACHE II mortality prediction was run on all 7570 patients with age ≥16 years.
Study population. Baseline characteristics of study population. IQR: interquartile range.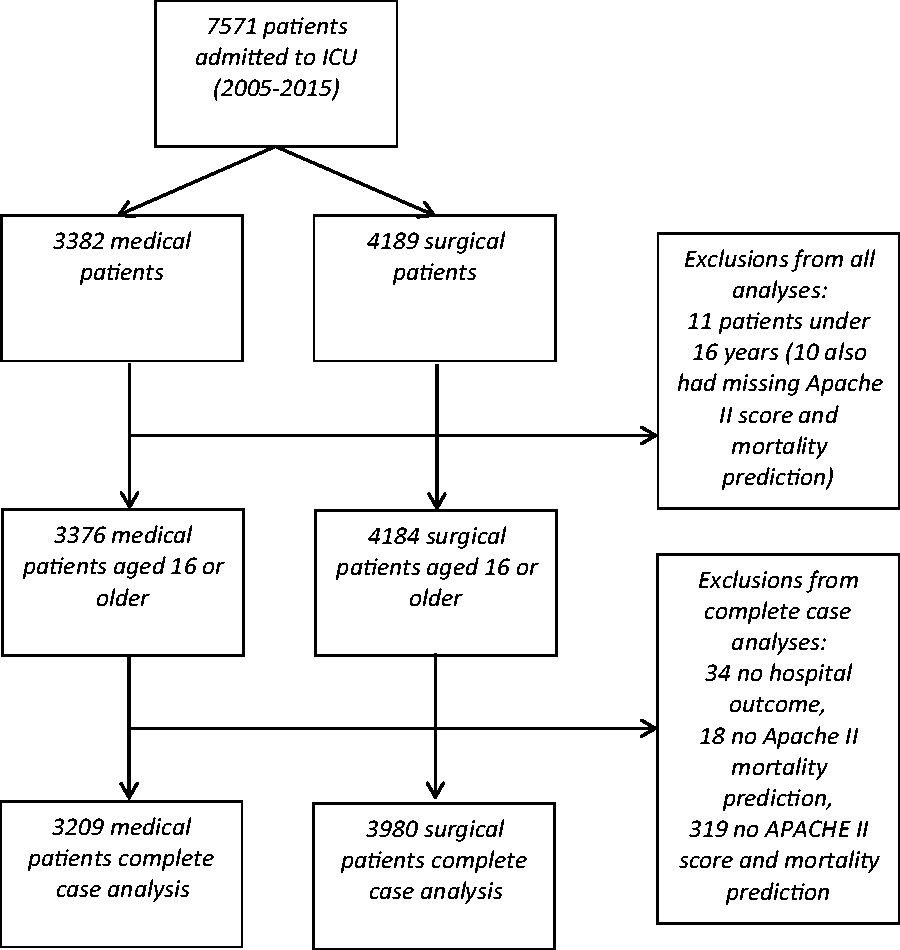
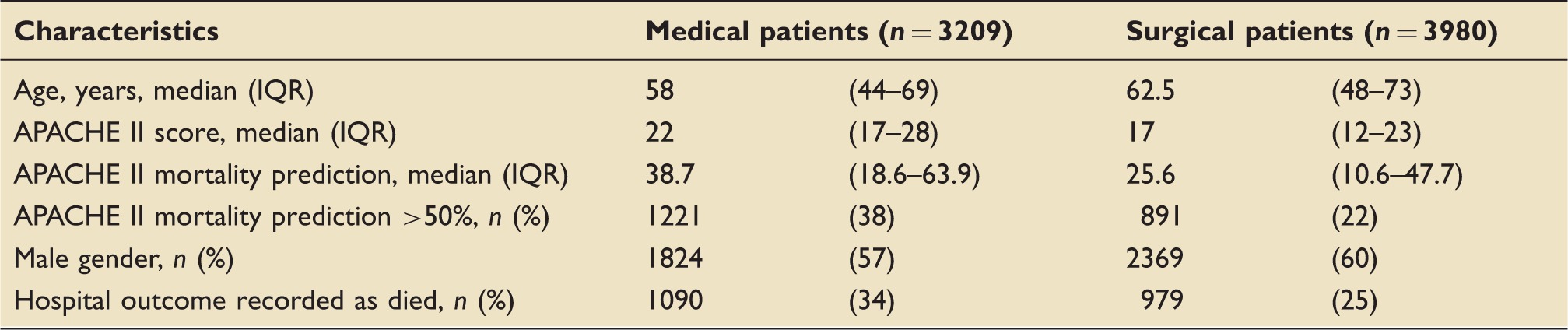
From 2005–2012, prior to the opening of the MHDU, a median of 24 medical patients (interquartile range (IQR) 21–28) and 30 surgical patients (IQR 24–34) were admitted to the ICU per month. Similar figures were recorded from 2013 to 2015, after the opening, with a median of 24 medical (IQR 19–27) and 31 surgical patients (IQR 28–35) per month. Comparisons ignoring time patterns (Mann-Whitney) showed no significant differences in the distributions of monthly counts of medical or surgical patient in the two periods, p = 0.40, 0.34, respectively. The MHDU admitted 3750 patients between December 2012 and November 2015. The first and final months of this period were not complete. Excluding these months, the medical HDU admitted a median of 105 patients (IQR 98–112) per month.
There was a modeled estimate of 60 ICU admissions per month, declining by −0.1 per month (−1.3 per year, p < 0.001) before the opening of the MHDU, to approximately 50 patients per month. Following the three-month wash-out period, there was an increase in the number of admissions to around 65 per month, and a subsequent steeper decline to approximately 45 patients per month, by the end of the study period. The linear decline in the count of admissions per month was by approximately −0.6 per month (6.8 per year, p < 0.001) (Figure 2). There was no evidence of any seasonal effect on overall admissions, medical admissions, or surgical admissions either by inspection or the statistical significance of these pairs of sine and cosine terms, which were therefore removed from the models.
Monthly number of patients admitted to ICU. The vertical lines indicate the period (December 2012–March 2013) during which the MHDU became operational.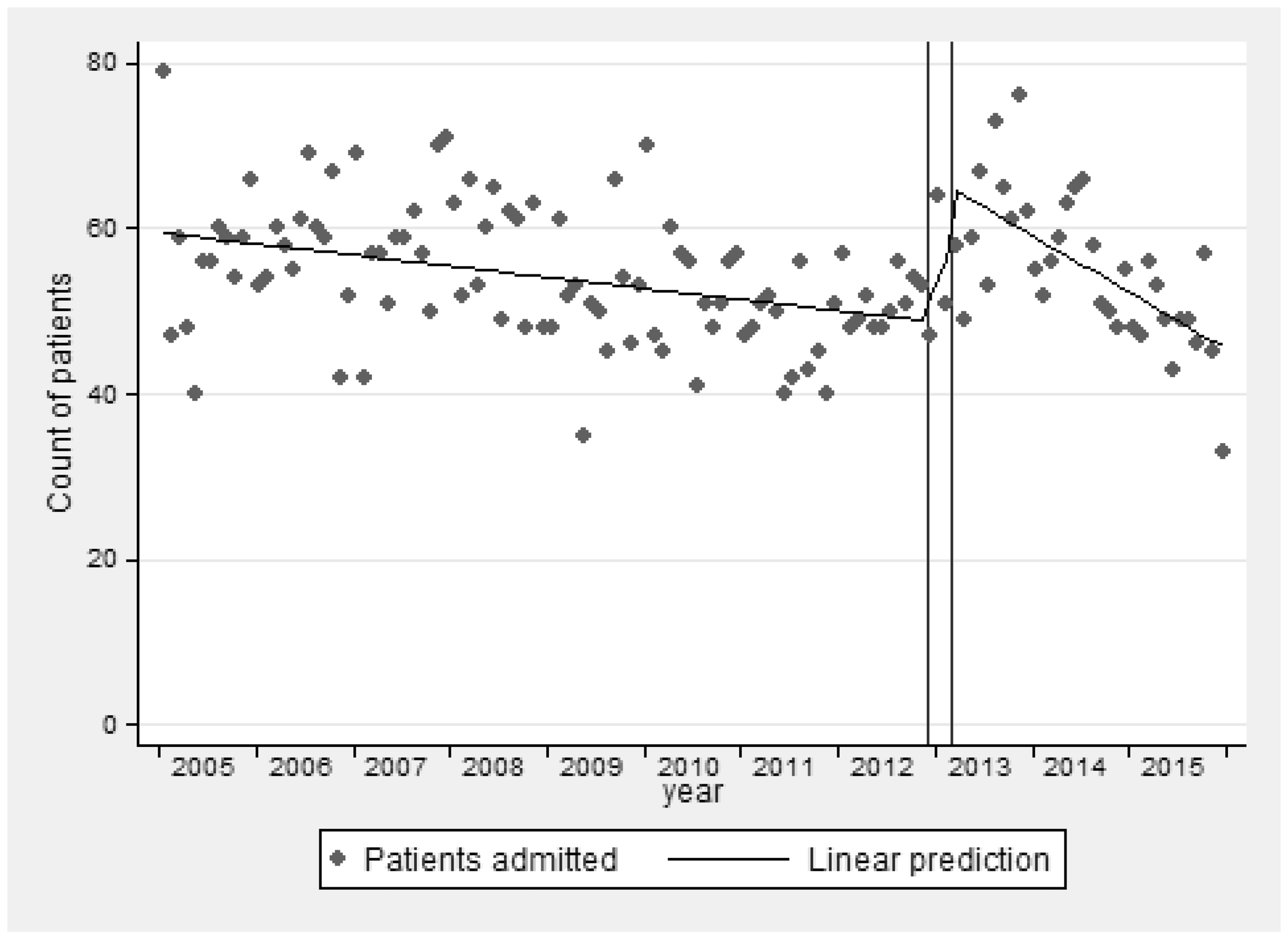
Differences between medical patients pre- and post-opening of the MHDUs
Number of patients admitted to the ICU
In 2005, there were approximately 25 medical admissions to the ICU per month. Over time, there was a non-significant decrease (−0.01 per month, p = 0.51) in the number of medical admissions until the opening of the MHDU. Following the wash-out period, there were around 27 patients per month, with a statistically significant decline thereafter of −0.2 per month (p = 0.007) down to 20 per month by December 2015 (Figure 3(a)).
Estimated monthly counts of admissions to ICU for (a) medical and (b) surgical patients.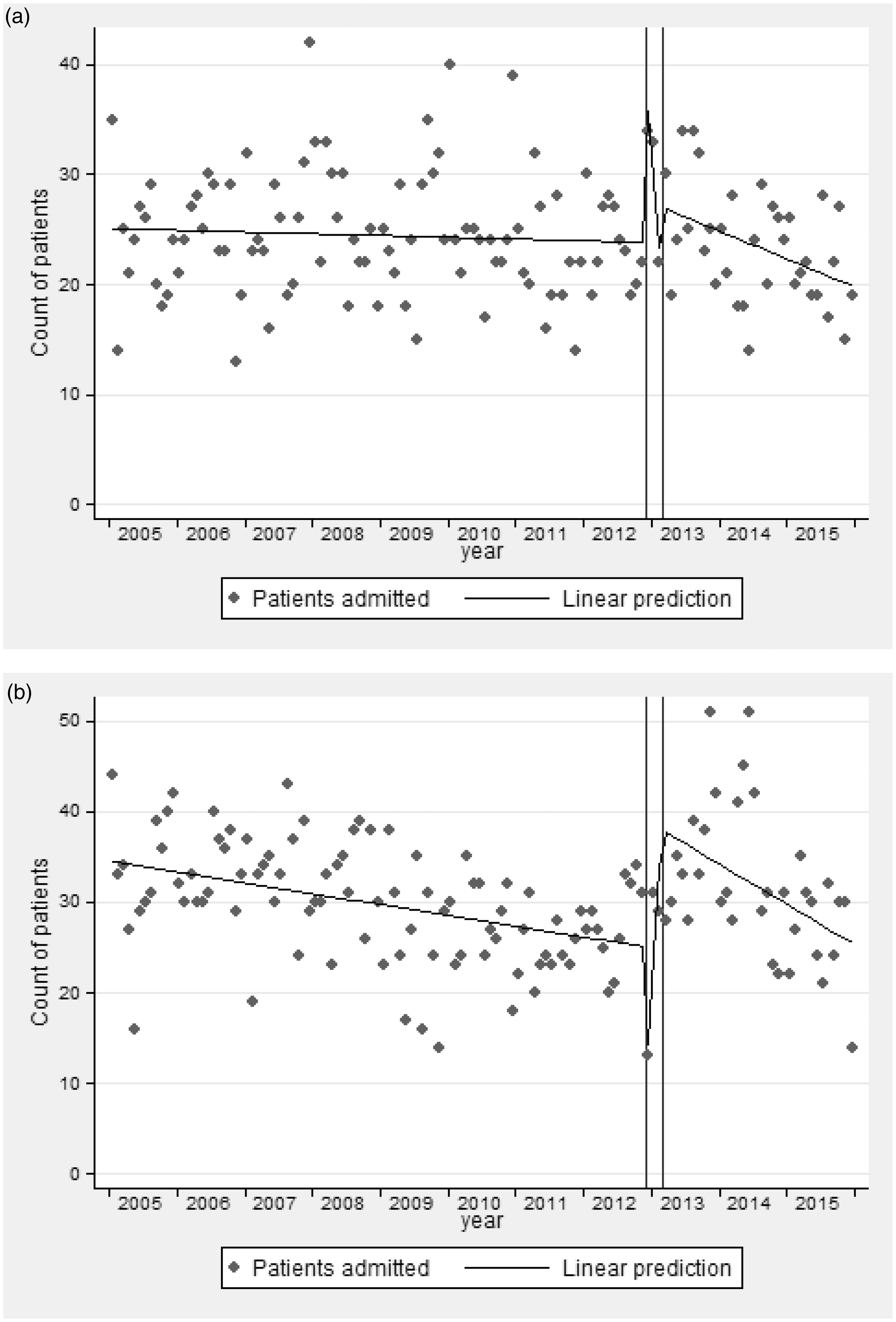
Severity of illness
The impact on severity of illness was analyzed by examining monthly mean APACHE II acute physiology scores. There was no evidence of seasonal patterns in mean APACHE score for either medical or surgical patients. For medical patients (Figure 4(a)), there appeared to be a small decline in the mean score before the intervention and a leveling off afterwards. The monthly mean APACHE II score was 24.6 in 2005, declining by −0.03 per month (p < 0.001) towards 21.5 by the opening of the MHDU. After the wash-out period, there was no significant further decline (−0.007 per month, p = 0.79).
Mean APACHE II score for patients admitted to ICU for (a) medical and (b) surgical patients.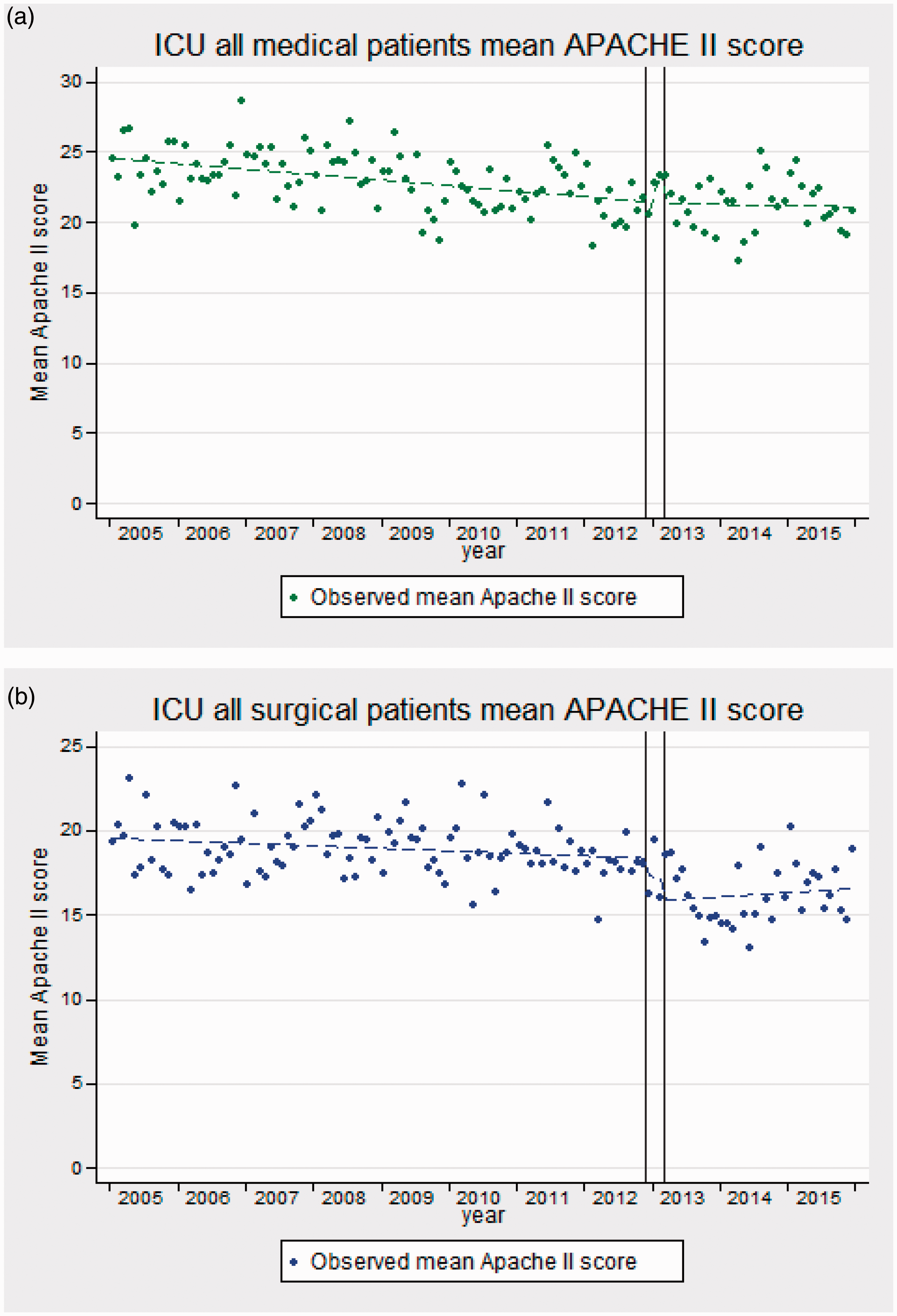
Crude and case-mix-adjusted mortality number of medical patients admitted to the ICU
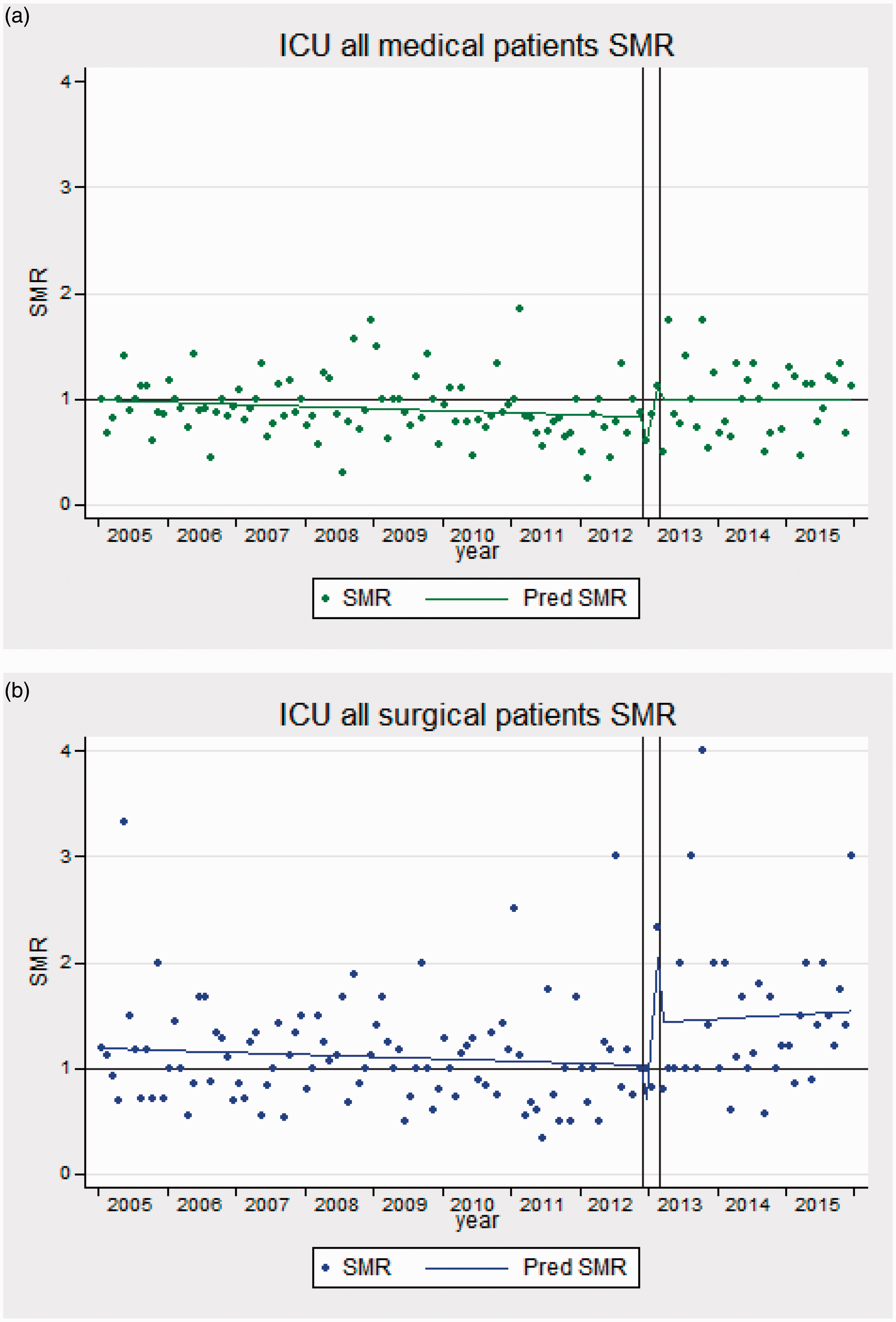
The modeled crude mortality of medical patients was 40% in 2005, decreasing by −0.1% per month (p = 0.007) to 30% before the opening of the MHDU, and increasing again by 0.3% per month (p = 0.054) to around 38% by 2015 (Figure 5(a)). The SMR was just under 1 in 2005 and showed a very small decline until the opening of the MHDU (slope −0.002 per month, p = 0.09) (supplementary Figures 1(a) and 7(a)). Following the wash-out period, the SMR returned to 1 and remained stable (slope −0.0001 per month, p = 0.99) (Figure 6(a)).
Observed monthly crude death rates for (a) medical and (b) surgical patients. Interrupted time series model of SMR for (a) medical patients and (b) surgical patients showing observed SMR (dots) and predicted SMR (lines).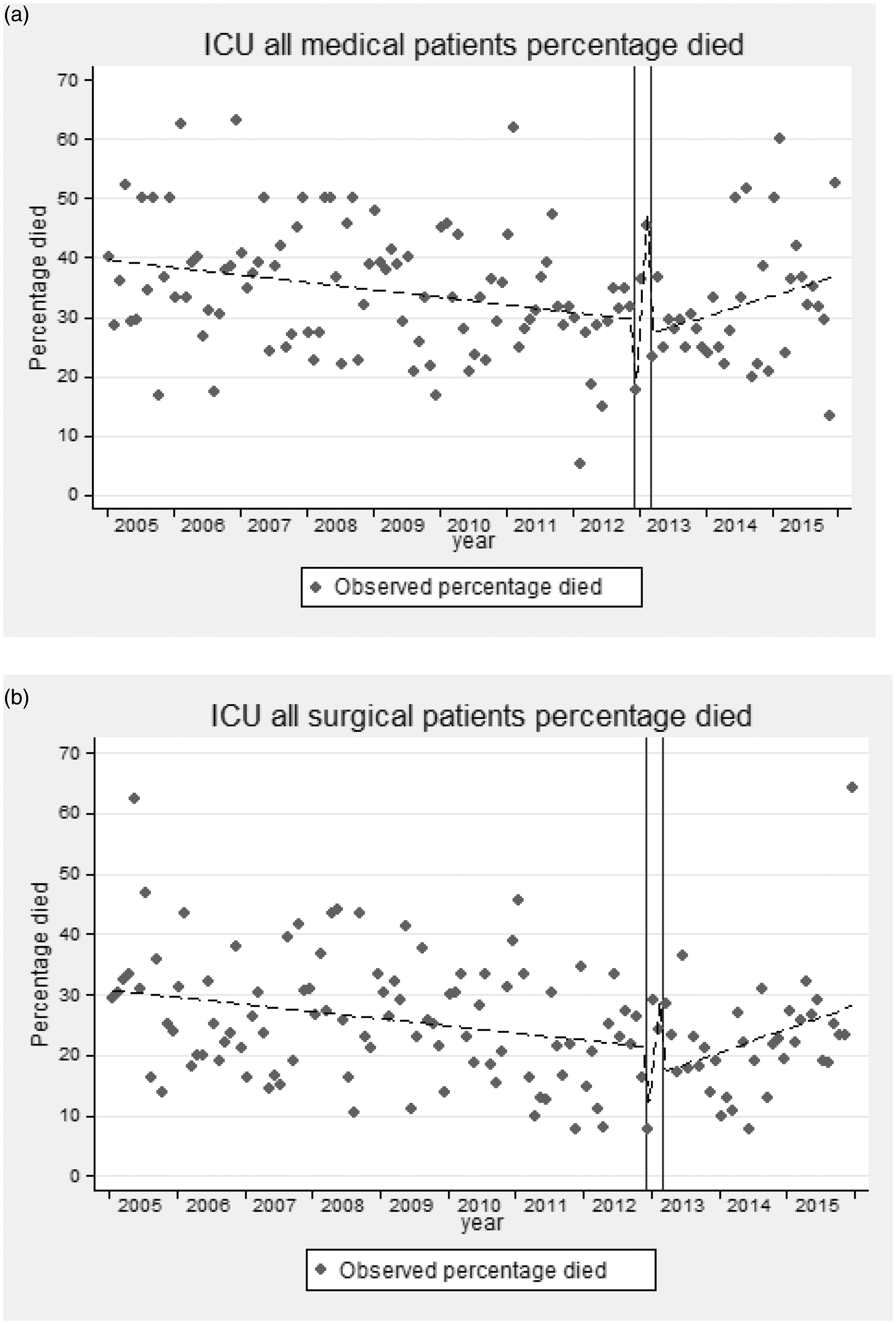
Differences between surgical patients pre- and post-opening of MHDU
Number of patients admitted to the ICU
In 2005, there were 34 surgical admissions per month with a significant decline over time of −0.1 per month (95% CI −0.2, −0.05, p < 0.001), to around 26 admissions per month before the opening of MHDU. Following the wash-out period, around 37 patients were admitted per month with a statistically significant decline (−0.36 per month, p = 0.005) thereafter to 25 per month by December 2015 (Figure 3(b)).
Severity of illness
For surgical patients, there was also a small, but significant decline (−0.01 per month, p = 0.023) in the mean APACHE II score (Figure 4(b)) from 19.6 in 2005 to 18.4 by the intervention. Following the wash-out period, there was a significant drop in the mean APACHE II score to around 16 (drop −2.3, p = 0.007, if modeled as a single step). There was little change thereafter (slope 0.02 per month, p = 0.57).
Crude and case-mix-adjusted mortality number of surgical patients admitted to the ICU
For surgical patients, the modeled crude mortality rate was 31%, decreasing (−0.1% per month, p = 0.012) to 22% before the opening of the MHDU (Figure 5(b)). Afterwards, there was a non-significant increase in the monthly crude mortality rate of 0.3% per month (p = 0.14) to around 28% by 2015. For surgical patients admitted to the ICU, the initial SMR was 1.19 in 2005 and there was a non-significant decline (−0.002 per month, p = 0.45) to 1 prior to the opening of the MHDU (supplementary Figures 1(b) and 7(b)). There was greater volatility in the observed surgical SMRs after the wash-out period, coinciding with the temporary closure of the neurosurgical HDU. Despite the apparent step increase in modeled SMR to 1.4 which remained stable (slope 0.003, p = 0.81), there was no evidence of a statistically significant change (p = 0.13 if modeled as a single-step change) (Figure 6(b)).
In summary, the number of medical and surgical patients increased just after the intervention and declined significantly thereafter. Although there was a decrease in the average severity of illness of medical patients prior to the opening of the MHDU, there was no evidence of a change following the opening. There was clearly a step decrease in the severity of surgical patients at the opening of the MHDU, but little change thereafter. Although there were small decreases in crude mortality in medical and surgical patients, before the opening of the MHDU, and increases subsequently, these increases were not statistically significant. For both medical and surgical patients, there were no statistically significant changes in the case-mix-adjusted mortality before or after the intervention.
When missing APACHE II scores and APACHE II mortality scores were imputed in 10 datasets, the findings were almost identical. The one exception was that for some imputed datasets, the apparent step up in SMR for surgical patients just crossed the threshold for statistical significance.
Discussion
This study presents a detailed evaluation of the effect of critical care service reconfiguration. There have been previous analyses, but these have concentrated on multidisciplinary high dependency/intermediate care units, rather than a specialist MHDU. A recent study from the Netherlands found that the establishment of such an intermediate care unit resulted in improved ICU utilization. However, the number of referrals, readmissions to the ICU and mortality rates did not change. 8 A further somewhat older study, from Canada, found that the closure of an intermediate care area altered ICU admission and discharge decision-making. The number of less seriously ill admissions increased and patients remained in the ICU for longer, until they required less nursing care. 7
The establishment of an MHDU in our hospital has had a small impact on the number, but little effect on the average illness severity, crude mortality, or case-mix-adjusted mortality of medical patients admitted to the ICU. Although there are measurable changes in these parameters—in particular, a small increase in the number of surgical admissions and increases in medical and surgical crude mortality—these do not reach the traditional limits of statistical significance, but could represent a small change in case mix. These changes have taken place on the background of a small overall decrease in the number of patients admitted to the ICU over time.
Overall, the impact of the new MHDU on the ICU has therefore been relatively minor. However, given the large number of patients who have been admitted to the MHDU, it appears that there was a large unmet need, in terms of medical patients who required high dependency care, but not intensive care, including those admitted for observation following, for example, gastrointestinal hemorrhage. These patients were, presumably, cared for on normal wards before the MHDU opened.
A recent report, by the Scottish Intensive Care Society Audit Group, had identified the ICU at Aberdeen Royal Infirmary as an outlier, in terms of risk-adjusted mortality. 12 A subsequent investigation raised the question of whether the opening of the MHDU, by removing less seriously ill patients from the analysis, could have accounted for the observed results. Our study shows that this is unlikely to have been the case.
This study evaluated the impact of service change from the perspective of the ICU. ICUs in Scotland have a long tradition of collecting detailed data permitting case-mix-adjusted comparison of outcomes. 12 Such detailed data are not currently available for all HDUs, or patients in conventional wards. It is therefore difficult to evaluate changes in the outcome of these populations over time or to compare differences in outcomes of patients with similar illness severities when managed in different settings. Consideration should be given to enhancing routine data collection, as also advocated for by the Scottish Intensive Care Society, 12 in order to facilitate a more comprehensive evaluation, of the impact of HDU care on patient outcomes.
This analysis has limitations, the most important being that it is a single-center study. The results pertain to a particular service configuration (and reconfiguration). The delivery of medical level 2 critical care across the National Health Service of the United Kingdom is very heterogeneous, with some hospitals having no HDUs, to others which have combined level 2/3 high dependency/ICUs, 2 and direct extrapolation of our findings to other settings may thus not be appropriate. The study, by its nature, also encompasses a long period of time, and there are coincident events, such as the temporary closure of the neurosurgical HDU, which could have influenced the results. Interrupted time-series analysis does not account for non-secular changes in service demand, e.g. increases related to influenza severity or coincident service reconfiguration, which might have been mitigated by using independent medical wards as a control.
However, our analysis also has strengths. The use of interrupted time series methodology, rather than a simple before/after comparison, permits the contribution of underlying long-term secular trends to be identified. 9 When comparing differences in variables over long periods of time, these secular trends must be accounted for in order to prevent the false perception of a significant difference attributable to an event, such as the opening of new facilities. Previous studies have not always used such designs.7,8 Our concomitant analysis of the number of surgical patients admitted to the ICU, which permits a degree of comparison, is an additional strength.
Conclusion
In conclusion, this single-center study, drawing on more than a decade of data, has shown that the opening of an MHDU in our hospital has had a minimal impact on the ICU. There was, in all likelihood, an unmet need—of less seriously ill patients, who were previously looked after on a normal ward, but did not require ICU admission—who are now cared for in the new MHDU.
Supplemental Material
Supplemental material for Evaluating service development in critical care: The impact of establishing a medical high dependency unit on intensive care unit workload, case mix, and mortality
Supplemental material for Evaluating service development in critical care: The impact of establishing a medical high dependency unit on intensive care unit workload, case mix, and mortality by Nabeel Amiruddin, Gordon J Prescott, Douglas A Coventry and Jan O Jansen in Journal of the Intensive Care Society
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.