
Abstract
Historically, neutropenic sepsis has been associated with high mortality rates. However, there has been limited research into cancer patients admitted with suspected sepsis who are found to be non-neutropenic. C-reactive protein has been shown to be raised in cancer patients for reasons other than infection and there have been limited studies to look as its utility as a prognostic biomarker in suspected sepsis in this population. This study looked at 749 patients admitted to a tertiary cancer centre between January 2015 and February 2016 with suspected sepsis. The neutrophil count and C-reactive protein level was taken in all these patients on admission and at 72 h and compared to the primary outcome of 30-day all-cause mortality rates and hospital length of stay. There were 49 patients who died within 30 days (6.5%). Patients who died were found to have both higher neutrophil counts and C-reactive protein level on admission and at 72 h compared to survivors. Prolonged grade 4 neutropenia was shown to have higher mortality rates. There was only weak correlation between either neutrophil counts or C-reactive protein level and length of hospital stay. This study suggests that higher C-reactive protein level and neutrophil counts and prolonged grade 4 neutropenia are associated with higher mortality rates in cancer patients admitted with suspected sepsis and have utility as prognostic biomarkers in this population.
Background
Sepsis is more prevalent in patients with cancer.1,2 Neutropenic sepsis, in particular, has high mortality rates and prolonged inpatient hospital stays.3,4 The diagnosis of infection in this cohort is difficult as its early signs and symptoms are mimicked by non-infective causes, including the cancer itself and responses to systemic anti-cancer treatment (SACT). 5
The white cell count is not specific in septic patients with cancer as it is influenced by SACT, the use of steroids and granulocyte colony-stimulating factor (G-CSF), and the disease itself. 6 Patients can develop neutropenic fever without an infective source, most commonly due to the production of pro-inflammatory pyrogenic cytokines such as IL-2, IL-6 and tumour necrotic factor (TNF). 7 Biomarkers of infection, such as C-reactive protein (CRP) and procalcitonin, are potentially useful in its diagnosis and monitoring the response to antimicrobial therapy.8–10 Surviving Sepsis Campaign 2016 International Guidelines suggest biomarkers may be used to support shortening the duration of antimicrobial therapy in septic patients. 11
In cancer populations, the utility of CRP has not been widely studied and mainly focused on the neutropenic and intensive care populations. 6 Both neutropenic and non-neutropenic patients have been shown to mount a CRP response, the course of which was not influenced by the neutrophil count. 12 A study of 314 patients showed significantly lower day 3 to 5 CRP values in survivors versus non-survivors. 13
There are limited studies looking at length of stay as a clinical outcome to assess neutropenia or CRP. A 2-year study of 307 febrile neutropenic patients showed each day of neutropenia added 2% to the patient’s total hospital stay. 14 A single hospital study of 96 COPD patients failed to find a statistical link between CRP on admission and length of hospital stay. 15
It is currently not clear whether CRP levels or neutrophil counts can be used as prognostic biomarker, assessed by both overall 30-day mortality rates and overall length of hospital stay in an unselected cancer population with suspected sepsis, this study aims to address these questions.
Methods
A retrospective analysis was performed at a specialist oncology hospital in the North West of England from 1 January 2015 to 31 January 2016. The hospital has a medical admissions unit (MAU), 16 which receives patients via a number of access points including directly from the hospital patient hotline, outpatient clinics and as tertiary referrals from other hospitals.
Basic demographic data were collected for each patient who presented with suspected sepsis (based on SIRS criteria in operation at the time), 17 alongside site of primary cancer, neutrophil count and CRP level on admission and at 72 h (or the result on discharge if the patient was discharged within 72 h). The primary outcome was overall 30-day mortality. Secondary analysis was performed on the length of hospital stay.
The data were analysed using GraphPad Prism 7. The p value for statistical significance was 0.05 and was tested using student’s t test. Correlation coefficients were used to compare the neutrophil count and CRP level at admission and at 72 h to create gradients of the effect on length of hospital stay.
Results
Patient demographics and neutrophil and CRP levels.
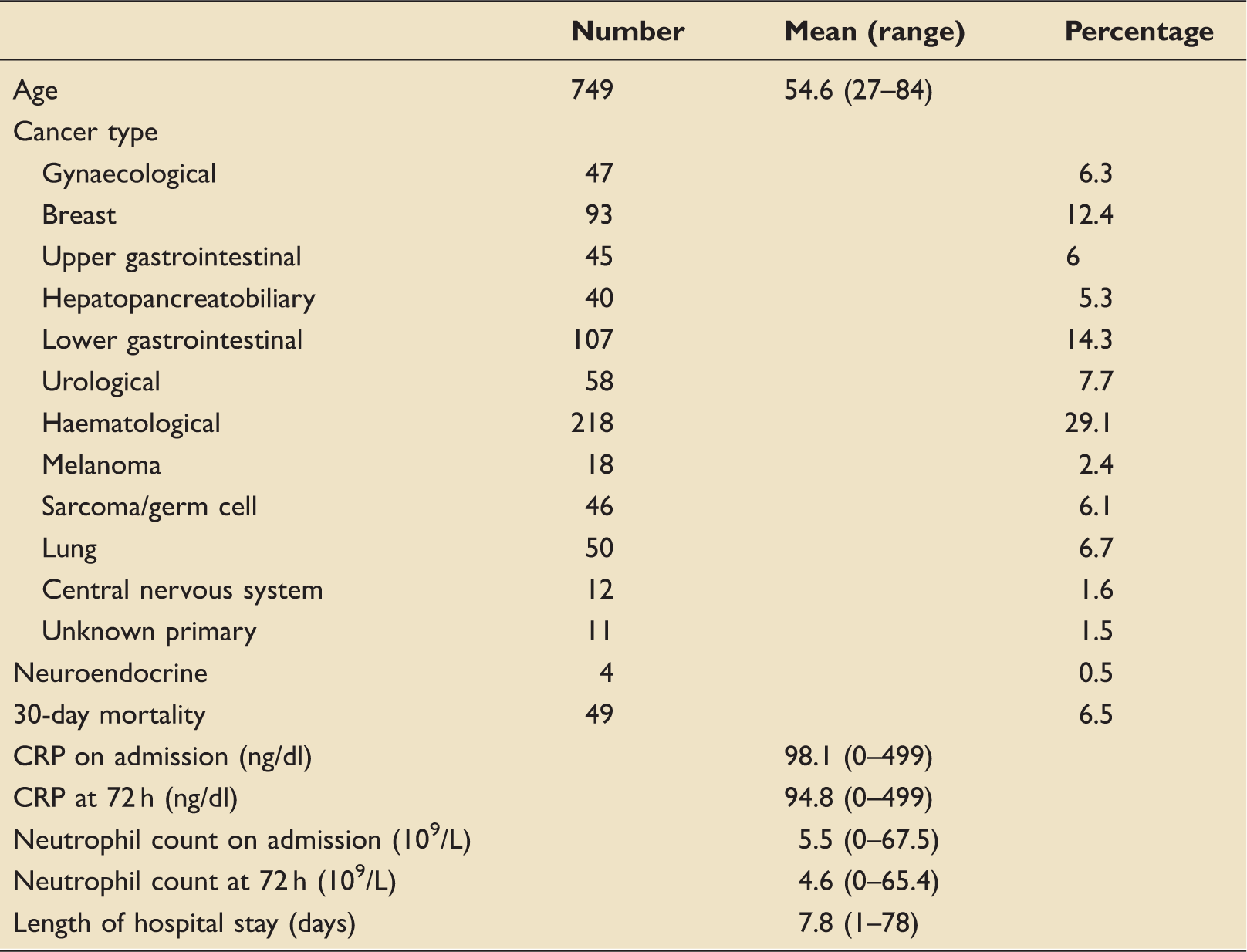
CRP: C-reactive protein.
Thirty-day mortality rates with neutrophil count split into grades of neutropenia on admission and at 72 h/discharge.
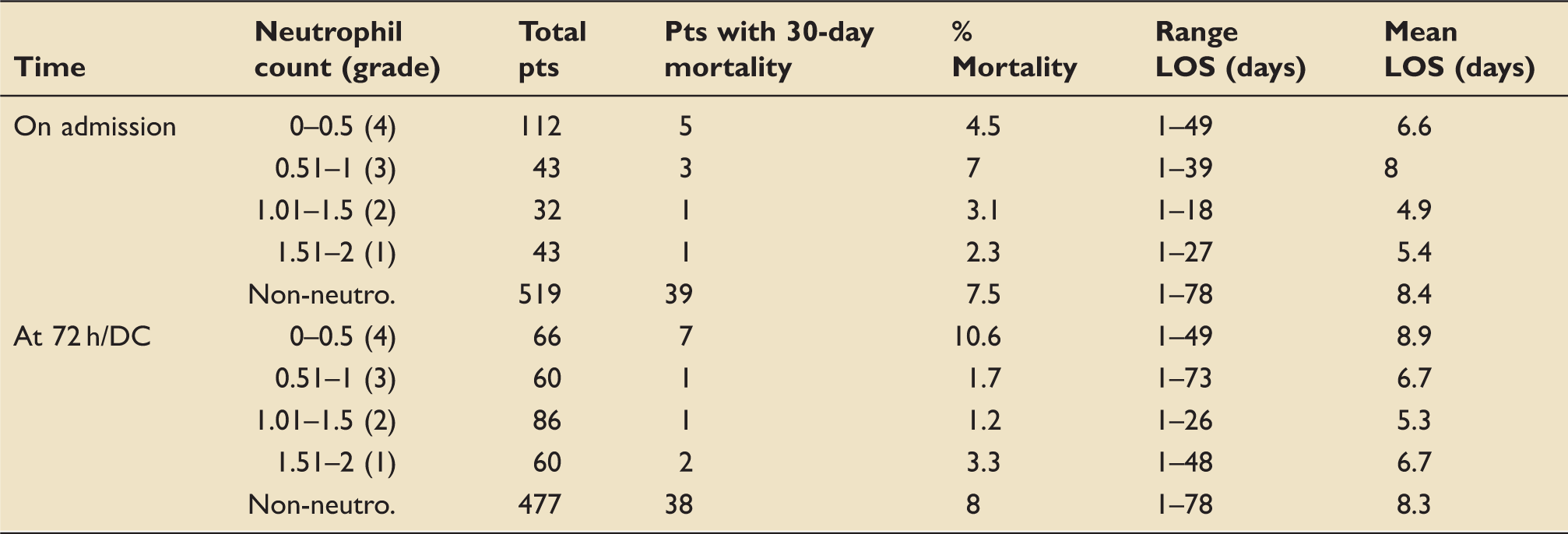
DC: discharge; LOS: length of stay.
Split of CRP on admission and at 72 h/discharge compared to 30-day mortality rate and length of stay.
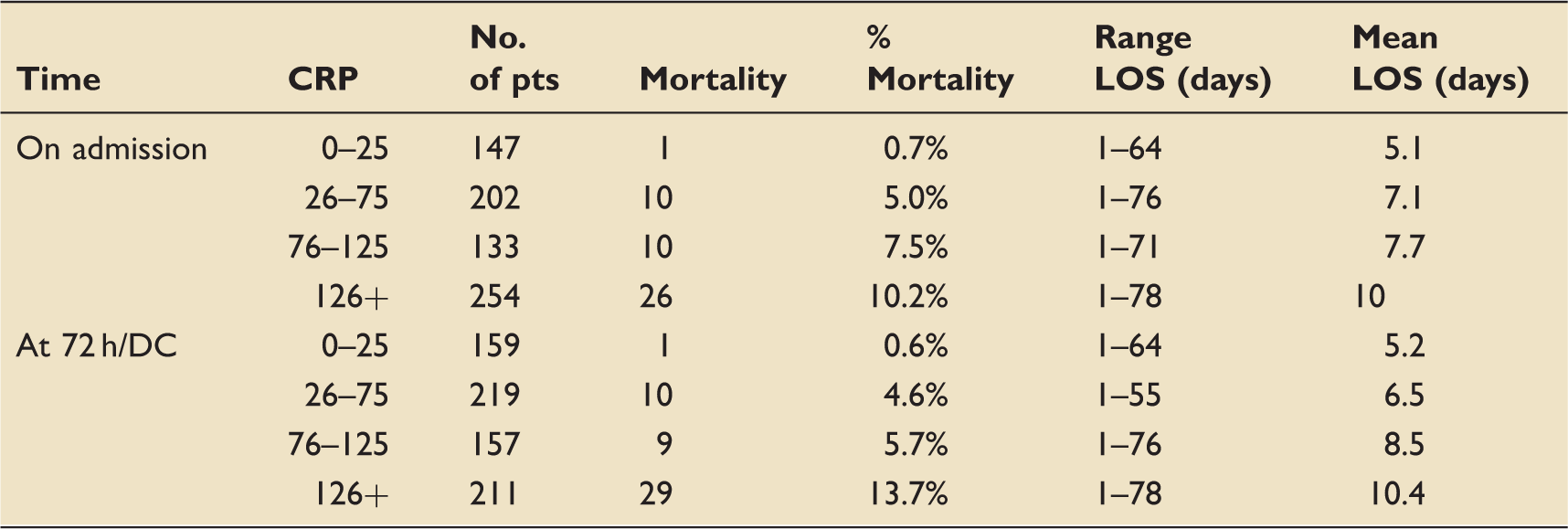
CRP: C-reactive protein.
The overall 30-day mortality rates increase in patients with higher CRP levels on admission and at 72 h (see Table 3). The mortality rate of patients who had a reduction in CRP between admission level and 72 h level was 5.5% compared to 10.3% in those patients with an increasing CRP level over the 72 h. Two patients died with a CRP of less than 25, one from progressive small cell lung cancer and one from pneumocystis jiroveci pneumonia.
At initial presentation, neutrophil count and CRP levels showed poor correlation. At 72 h, patients with neutrophilia (>8 × 109/L) and grade 4 neutropenia (<0.5 × 109/L) had significantly raised CRP levels (see Figure 1).
Box plots assessing CRP level and neutrophil count on admission and at 72 h. CRP: C-reactive protein.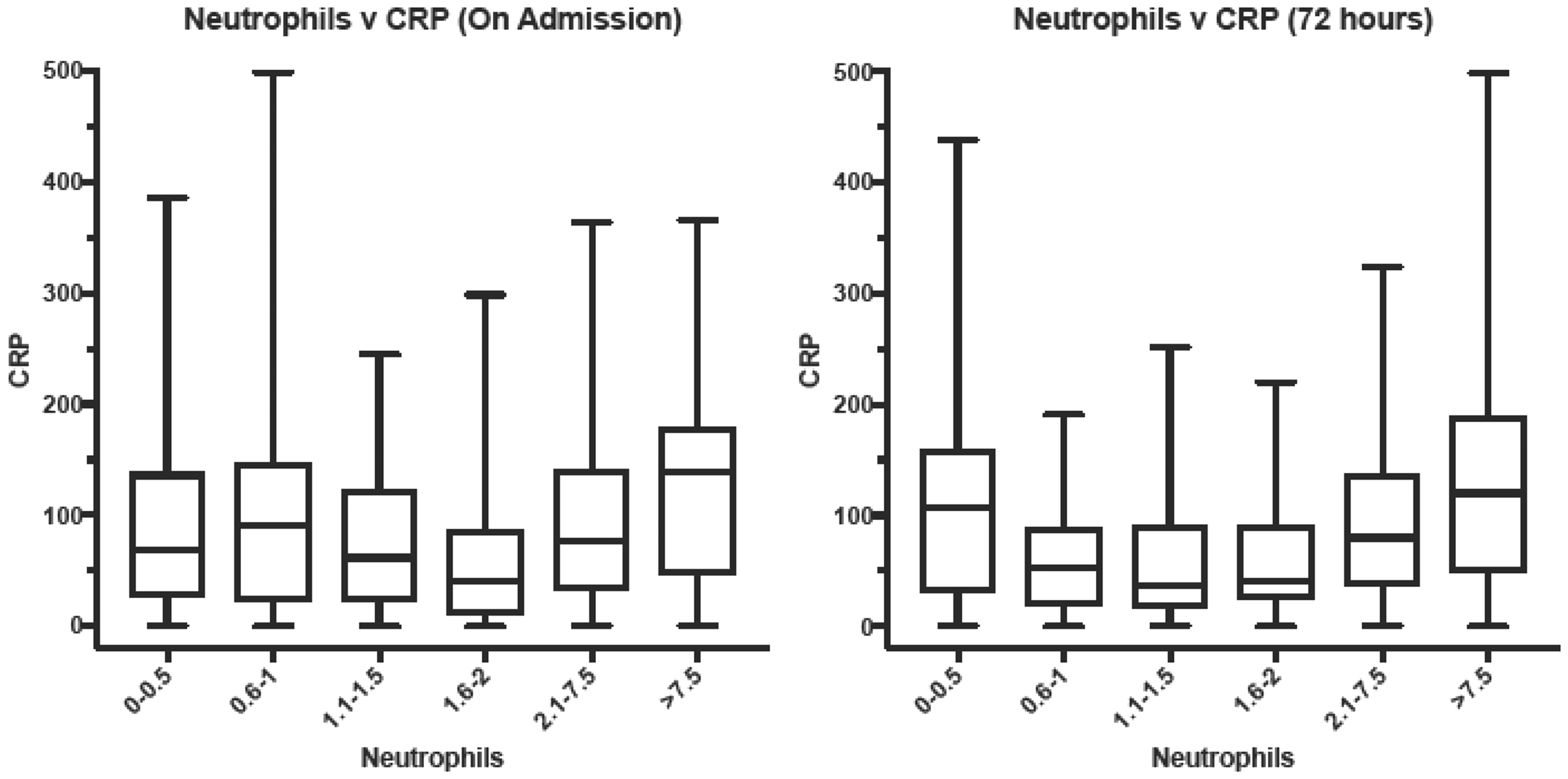
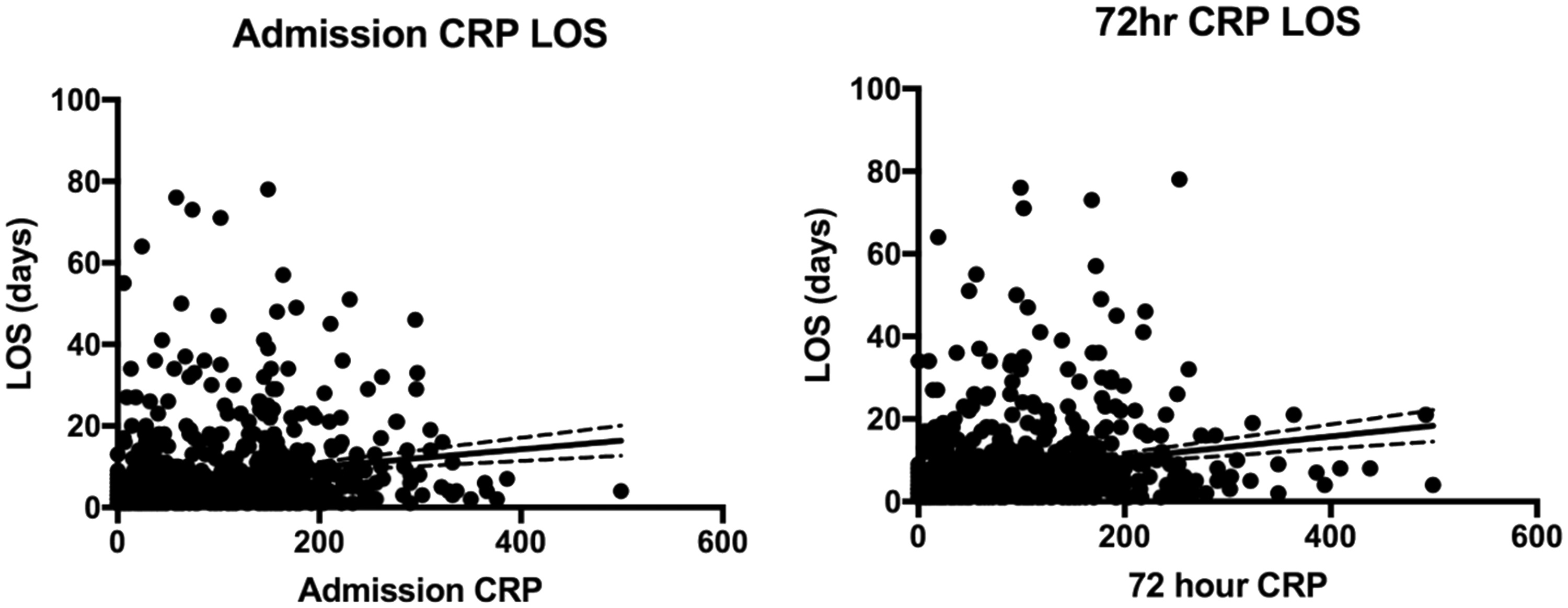
Both on admission and at 72 h, CRP levels and neutrophil counts had very weak correlation with length of hospital stay (length of stay compared to: CRP OA, r = 0.16; CRP at 72 h, r = 0.19; neutrophils OA, r = 0.05; neutrophils at 72 h, r = 0.13). The correlation worsens when looking at the change in both CRP and neutrophil over 72 h (r = 0.05 and r = 0.09, respectively) (see Figures 2 and 3).
Scatter graphs of neutrophil count on admission and at 72 h against length of hospital stay in days. Scatter graphs of CRP on admission and at 72 h against length of hospital stay in days. CRP: C-reactive protein.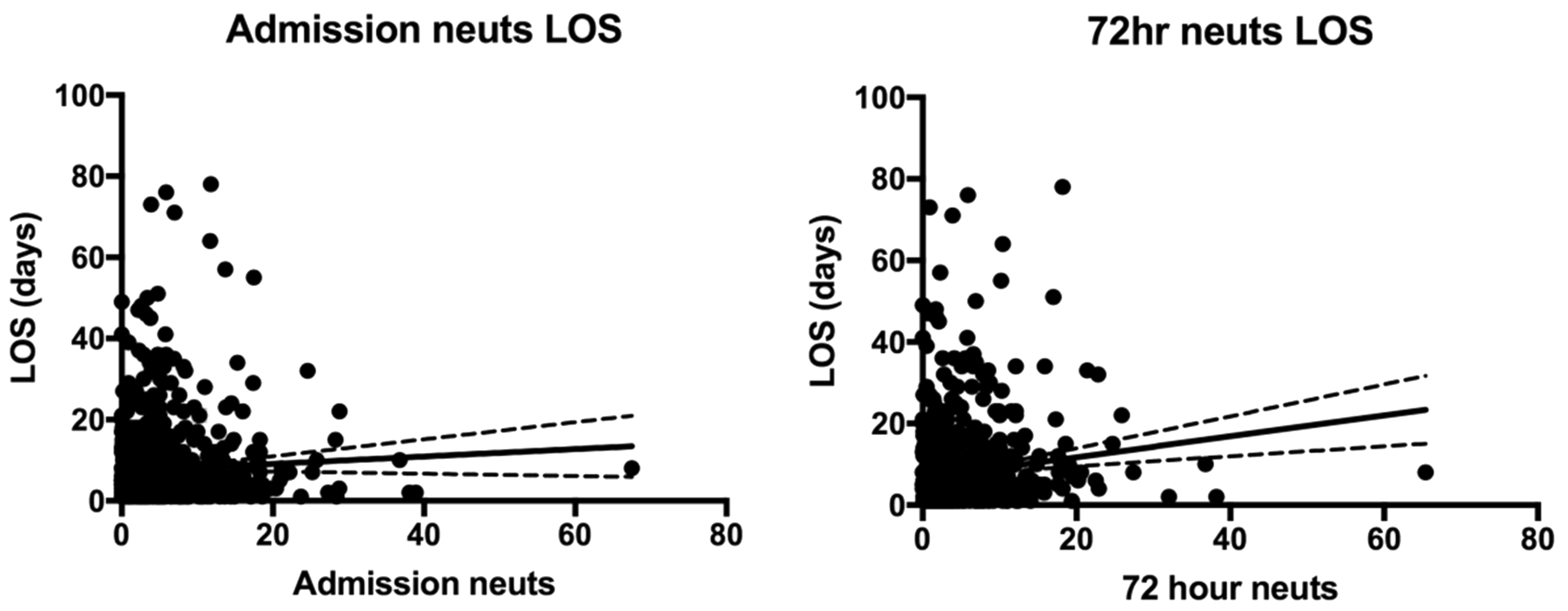
Discussion
This study suggests that the CRP level and neutrophil counts could be useful biomarkers in predicting outcomes in cancer patients presenting with signs and symptoms suggestive of sepsis. Both CRP level and neutrophil counts were significantly higher in patients with 30-day mortality but neither was predictive of a longer inpatient stay.
The identification of infection in patients with cancer is a key clinical challenge. Numerous biomarkers, such as CRP, procalcitonin, IL-6 and IL-8, have been studied with regards to diagnosis of infection, identification of infective agents and sepsis outcome prediction, particularly in the neutropenic population.6,10,11,18–20 Procalcitonin concentrations in septic patients with cancer are lower in those with leucopenia. 21 Furthermore, infection has been confirmed in neutropenic patients with procalcitonin levels <0.5 ng/ml. 22 In our study, a patient with a CRP <25 ng/dl died of an infective illness.
This study almost demonstrates an increasingly noted trend of lower mortality rates in patients with neutropenic sepsis compared to non-neutropenic sepsis in cancer patients. This may reflect that high mortality rates in neutropenic patients reflect a different era of both sepsis management and chemotherapy prescribing. This study adds to the evidence that with appropriate patient selection for myelosuppressive chemotherapy regimens and high quality care of patients with suspected neutropenic sepsis, mortality rates should be less than 5%. Patients at the highest risk of mortality include those with ongoing grade 4 neutropenia at 72 h, persistent neutrophilia or those with a rising CRP at 72 h.
This study is limited by being a retrospective single centre analysis. We also only studied neutrophil and CRP levels for the first 72 h. It is also difficult to determine definitively if the patients died from sepsis or progressive cancer but this reflects the diagnostic challenge in this population. Due to use of retrospective data, this study hasn’t analysed disease severity or accounted for other confounders such as co-morbidities and disease severity. As of 2016, SIRS criteria were replaced by the quick sequential organ failure assessment (qSOFA) after it was shown to be more prognostic for in hospital mortality, 23 however, using our selected population allows comparison with previous studies. This study is strengthened by being the largest single centre analysis of cancer patients with suspected sepsis in the UK and the fact that 96.4% of patients presenting with suspected sepsis to the OAU receive their first dose of intravenous antibiotics within 1 h through a previously described nurse-led protocol. 24 Delays in administration of antibiotics in septic patients with cancer have been shown to affect both mortality and length of stay.25,26
Conclusion
Increasing CRP, neutrophilia or 72 h of sustained neutropenia appear to be useful independent prognostic biomarkers of 30-day mortality in cancer patients with suspected sepsis. Additional prospective research of these biomarkers analysing for confounders such as disease severity, comorbidities and qSOFA scores would add further clarity to their utility in cancer patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.