
Abstract
With a chronic shortage of doctors in intensive care, alternative roles are being explored. One of these is the role of the Advanced Critical Care Practitioner. The Advanced Critical Care Practitioner Curriculum was developed by the Faculty of Intensive Care Medicine and is used to provide a structured programme of training. The Advanced Critical Care Practitioner programme consists of an academic and clinical component. This article outlines a practical approach of how the programme was developed and is currently being delivered at a single institution. This new advanced practice role offers opportunities to fill gaps in the medical workforce, improve continuity of patient care, provide mentoring and training for less experienced staff as well as offering a rewarding clinical role.
Background to Advanced Critical Care Practitioner (ACCP) programme
In the UK, advanced nursing practice has developed over the past 40 years. With a chronic shortage of doctors, a growing ageing population and greater numbers of patients with complex long-term conditions; advanced practitioner (AP) roles have grown in many settings including emergency, primary and secondary care.1–5 Although advanced critical care nurse practitioners (ACCNPs) have been established in the US since the early 1990s, this role has not developed to the same extent in the UK. 6 Also, whereas the critical care outreach nurse has been a well-established role throughout the UK, there was no national consensus on the ACCNP role. To address this, in 2015, the Faculty of Intensive Care Medicine developed a curriculum for Training for ACCPs that was applicable to both nurses and other allied health professionals. 7 Unlike other countries such as the US and Australia, nurse practitioners (NP) are not protected titles in the UK and there has been a lack of consensus on the definition of an AP or NP. The curriculum was developed for a Postgraduate Diploma/Masters level qualification in ACCP. Its development was informed by, and aligned to, the National Education and Competence Framework for ACCPs (Department of Health, March 2008) and the Advanced Practice Toolkit for Scotland (Scottish Government, June 2008).8,9
The curriculum builds on various frameworks including Skills for Health that attempts to benchmark practice and support a structured career ladder.10,11 Health Education England has recently released a definition for advanced practice:
12
Advanced Clinical Practice is delivered by experienced registered healthcare practitioners. It is a level of practice characterised by a high level of autonomy and complex decision-making. This is underpinned by a Masters level award or equivalent that encompasses the pillars of clinical practice, management and leadership, education and research, with demonstration of core and area specific clinical competence.
12
Given this new role and the publication of a specific curriculum by FICM, the aim of this article is to discuss the experience of implementing this new ACCP role at a central London critical care unit (CCU) that specialises in cancer care.
Rationale for introducing the role
In 2016, the Royal Marsden Hospital, approached Kings College London University with the aim of working collaboratively on appointing and supporting two ACCPs through the 2-year training programme. The rationale for setting up the ACCP programme was to develop a skilled practitioner role, which would aid multidisciplinary team working, facilitate continuity of patient care and provide support for gaps in the junior doctors' critical care rota. Anticipated benefits include enhancement of junior doctors training experience by allowing them to focus on training opportunities during their rotation. In addition, the ACCP programme provides a robust developmental pathway for senior nurses who wish to advance within a clinical nursing role, supporting recruitment and retention of skilled staff. A business case was put forward to the Trust demonstrating the potential advantages of this new role and the posts were financed through longstanding vacant junior doctors and nursing posts. The posts were presented to the Trust's Integrated Governance and Risk Management Committee (IGRM) to ensure that the Trust was satisfied with their scope of practice from a clinical governance perspective. The candidates were also strongly encouraged to take up personal indemnity at the start of their training programme.
Principal clinical duties and responsibilities for trainee ACCPs.
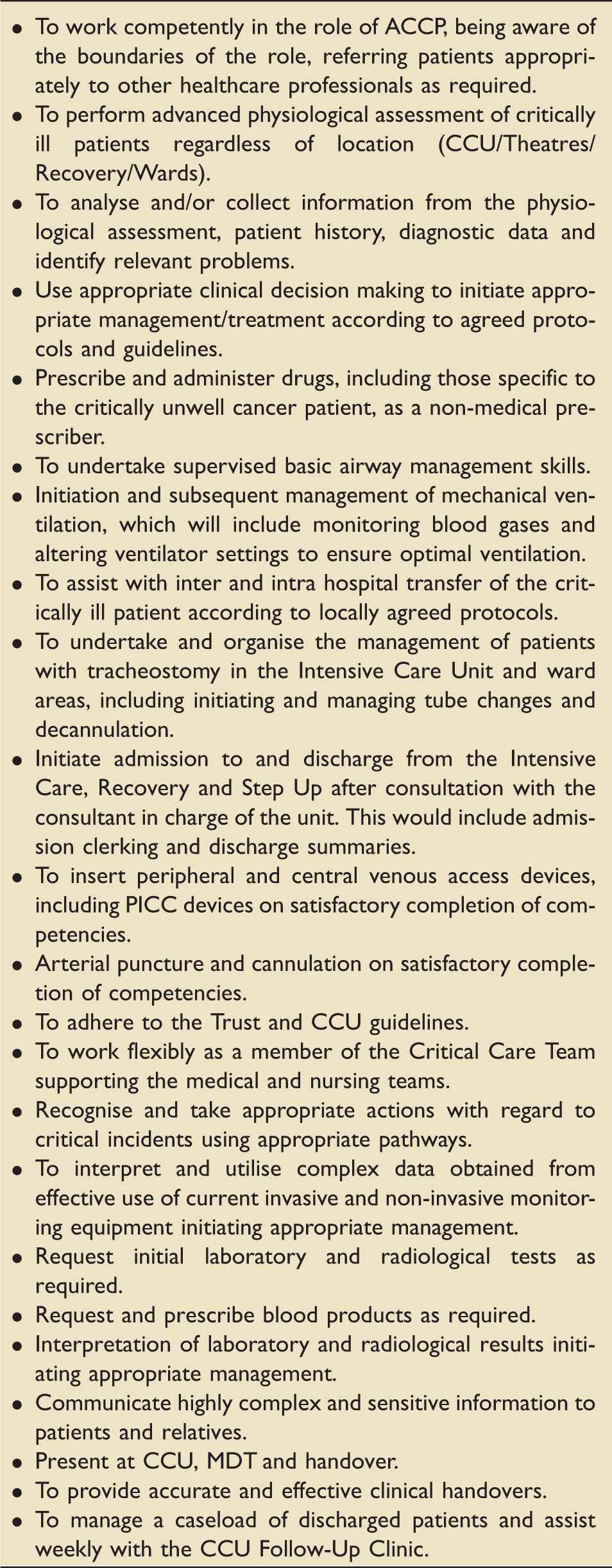
ACCP: Advanced Critical Care Practitioner; CCU: critical care unit; MDT: Multidisciplinary team; PICC: Peripherally inserted central catheter.
Preparation of ACCP programme: Curriculum, assessment and supervision
ACCP curriculum
ACCP competency framework aims.
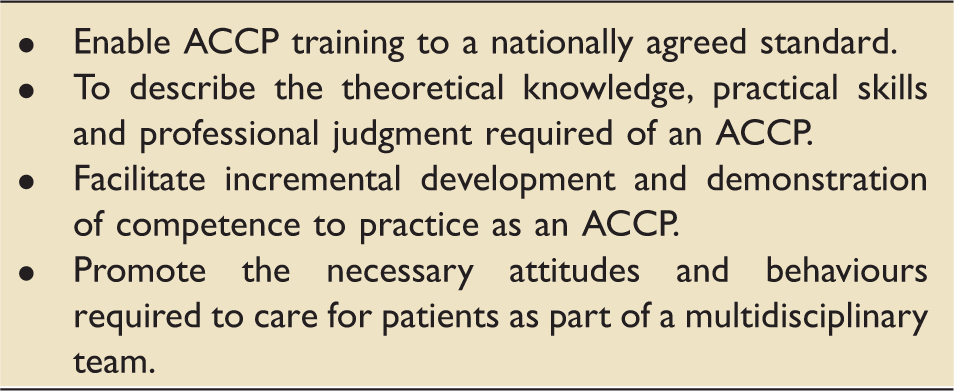
ACCP: Advanced Critical Care Practitioner.
Teaching
HEI-accredited PG Dip modules.
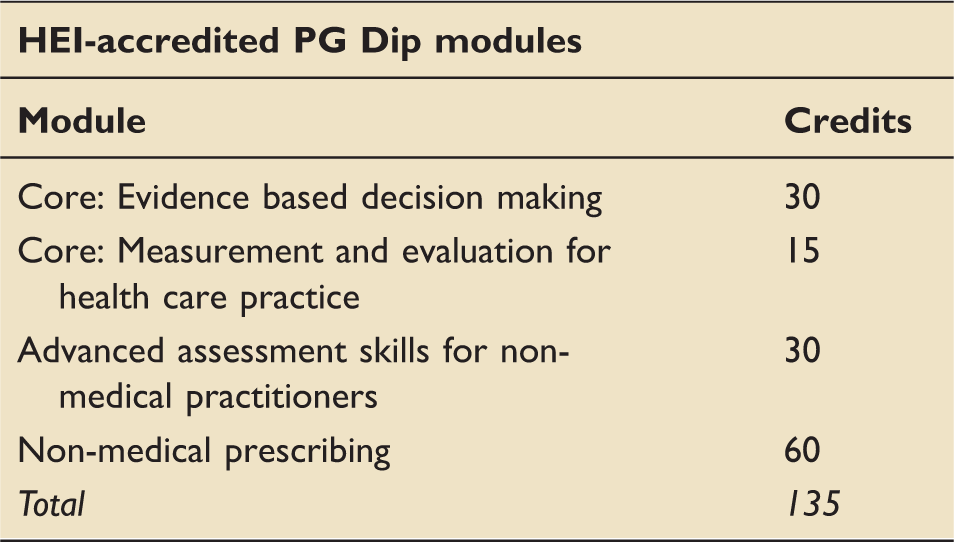
HEI: Higher Education Institution; PG Dip: postgraduate diploma.
Clinical supervision and course delivery
Clinical and academic training programme.
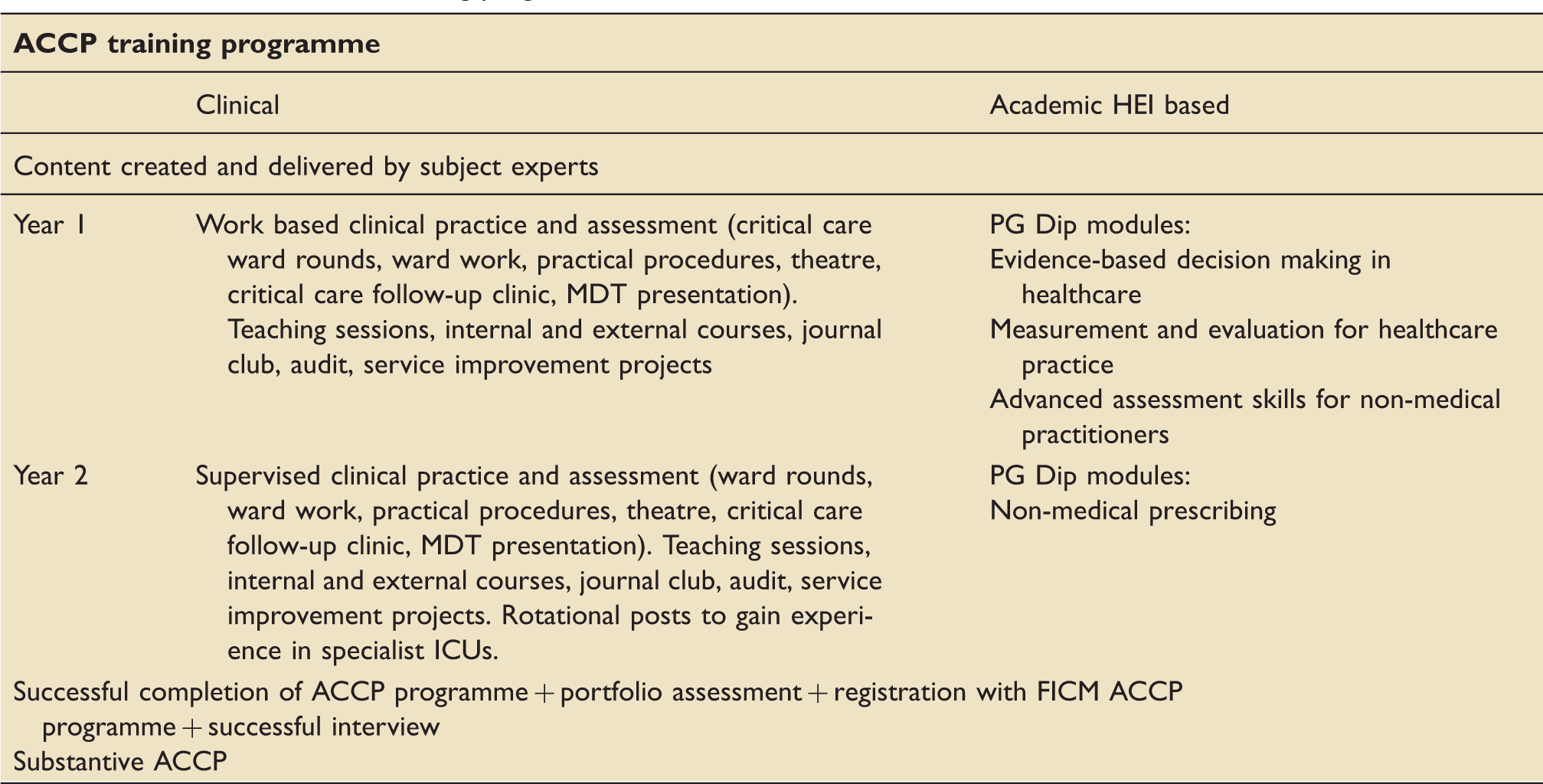
ACCP: Advanced Critical Care Practitioner; HEI: Higher Education Institution; PG Dip: postgraduate diploma.
The decision was taken that the first 8 months of training would be supernumerary during day time weekdays, the second 8 months would involve work and supervised training during day time weekdays but may include training outside these hours (evenings and weekends) and the third 8 months will include work and supervised supernumerary training on a rota in line with the junior medical critical care rota.
At the end of 2 years, ACCP trainees who have satisfactorily completed ACCP FICM competency training programme, completed their PG Dip or MSc and are accepted as Associate Members of the FICM will be invited to interview for the substantive ACCP role. At this point, they will no longer be supernumerary and be integrated into the junior medical doctors' rota.
Assessment
As well as the formal academic assignments and examinations as part of their HEI PG Dip or MSc, trainees are required to demonstrate that they have completed all the competencies of the ACCP FICM curriculum. Many of these have components common to doctors in training in Intensive Care Medicine and critical care nurses. For those competencies unable to be covered in the primary CCU, the ACCP trainees are allocated for rotational blocks of periods out of the primary unit. This includes spending time in specialist centres such as cardiothoracic intensive care, trauma units and neuro-CCUs.
The ACCP trainees maintain their training portfolio throughout the programme. This includes workplace-based assessments (WPBAs) that are integrated throughout the programme and allow the trainees to be given detailed and constructive feedback to improve their practice as well as allow review of their cognitive, psychomotor and behavioural learning outcomes. These WPBAs are mapped against the competences (based on the requirements of the GMC's Good Medical Practice); 13 WPBAs used include the ICM mini clinical evaluation exercise (I-CEX), directly observed procedural skills (DOPS), case-based discussion (CBD) and acute care clinical assessment tool (ACAT). Trainees are required to document each of these in detail as part of their portfolio. A minimum number of WPBAs is specified by FICM. The actual number of observations of work required are reviewed and adjusted according to the ACCP trainee's progress and set objectives during their quarterly review. In addition, the programme stipulates that the ACCP trainees have to gain at least a 50% pass in all the components of the end of year formative assessment (OSCEs, case presentations), attend at least 80% of the formal teaching sessions, pass all the relevant University modules and pass all the external courses (Advanced Trauma and Life Support Course, Basic Assessment and Support in Intensive Care, etc.).
Students maintain a portfolio (known as the ARCP in FICM documentation) and this consists of the documentary evidence submitted by the ACCP trainee. The portfolio includes, as a minimum, a review of the ACCP trainee's Training Record and portfolio and a structured report from the educational or clinical supervisors. For the progression of students, we provide formal quarterly assessments of the trainees in the workplace with educational, clinical and HEI academic supervisors present.
Implementation of ACCP programme
Prospective ACCP candidates underwent a structured interview after shortlisting. Interviews were held in April 2016 with five candidates short-listed and the interview panel consisted of the ACCP Local Clinical Lead, a second Intensive Care Consultant, the Nurse Manager and the HEI Academic Lead and a representative from Human Resources. The calibre of candidates was excellent and two trainees were appointed. The trainee ACCPs programme commenced in June 2016 and the two ACCPs registered with FICM and enrolled in the HEI MSc. Both trainees are nurses: one trainee was an internal candidate and the second candidate had been working as a senior nurse in another London intensive care unit. As part of their appointment and as mandated by FICM, both trainees arranged their own professional indemnity cover.
At the first meeting with their respective educational and academic supervisors, an ACCP educational agreement was devised for each ACCP trainee. The agreement included clinical management objectives such as clinical assessment of acutely ill patients and undertaking micro ward rounds, expected number of practical procedures that should be undertaken (i.e. venepuncture, arterial line insertion and central line insertion), expected self-study modules to be completed, expected academic modules to be completed, expected courses and teaching sessions to be attended. Trainees also identified an audit that they could undertake and details of planned teaching and study days.
Both ACCP trainees have produced appropriate educational agreements and worked with their nominated Consultants presenting cases on a weekly basis and setting specific learning objectives to be achieved for the next meeting. Quarterly meetings were held to assess progress in October 2016 and January 2017.
In June 2017, the ACCP trainees' Annual Review of Competency Progression (ARCP) was undertaken with both trainees progressing and meeting all the requirements. The review was undertaken by the ACCP Local Clinical Lead, educational and academic supervisors and Nurse Manager. The academic supervisor completed the HEI End of Attachment Assessment and the educational supervisor completed the Educational Supervisor's Report.
Overall from a clinical and educational perspective, both trainees were able to be provide a comprehensive portfolio documenting all their study days, courses attended, self-study modules completed, teaching days attended, practical procedures undertaken, WBAT and evidence of FICM curriculum competencies achieved. In a formal ARCP meeting with the academic and educational supervisors, ACCP Local Clinical Lead and Nurse Manager we all agreed that the trainees were progressing at a satisfactory rate and had achieved their educational objectives and overall competencies. This included specific competencies relating to their specialist clinical roles and included knowledge such as infection diagnosis and management, haematology as it relates to critical care, mechanisms of drug action and practical skills such as venepuncture, central line insertion and urinary catheterisation.
Workplace-based assessments of ACCP trainees completed by end of Year 1.
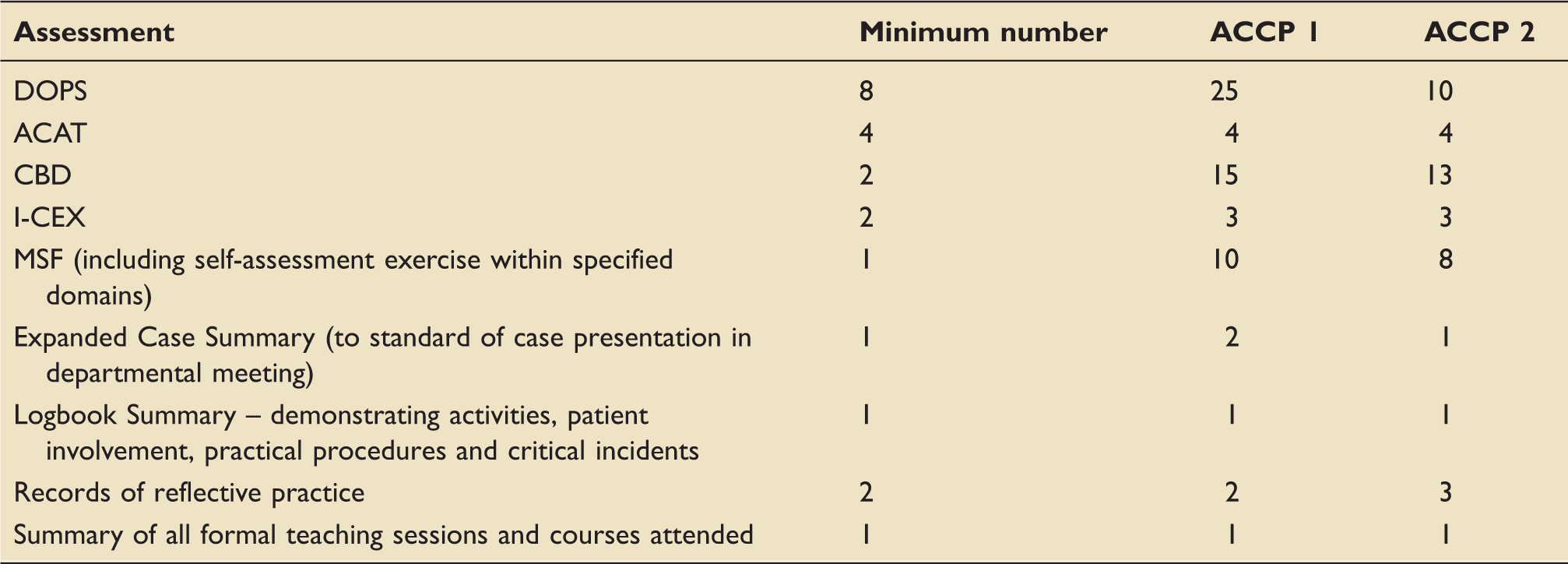
ACAT: Acute Care Assessment Tool; ACCP: Advanced Critical Care Practitioner; CBD: Case-based Discussion; DOPS: Direct Observation of Procedural Skills; I-CEX: ICM Mini-Clinical Evaluation Exercise; MSF: Multi-Source Feedback.
With the ACCP trainees' university modules, both have successfully completed their modules for the academic year 2016/2017. One trainee has completed all the diploma modules and is ready to start the dissertation and the second trainee has undertaken 60 credits to date. Collaborate quarterly meetings will be maintained for year 2 with the aim that both trainees will have completed academic and clinical requirements.
Feedback and learning to date
Key potential advantages and challenges of implementing the ACCP programme.
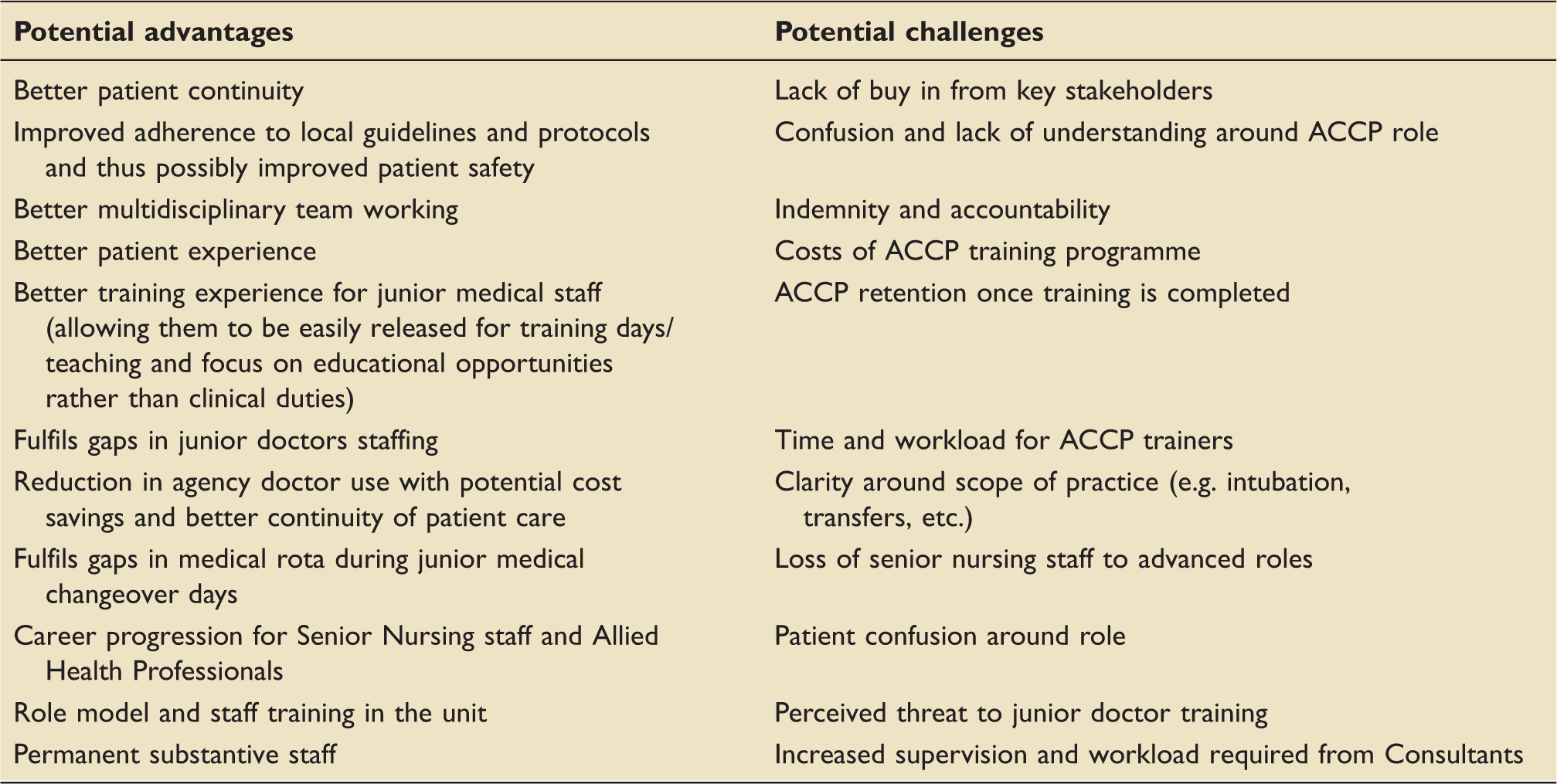
ACCP: Advanced Critical Care Practitioner.
The process of initiating and implementing an ACCP trainee programme is labour intensive and is not inexpensive. Setting up the programme required significant input from the local ACCP Lead Clinician, fellow ICU consultants who can act as educational and clinical supervisors, the Nurse Manager, an appropriate HEI academic supervisor and, most importantly, buy-in from key stakeholders. Regular weekly meetings between the Consultant and the ACCP trainee ensured that there was continuity and allowed regular feedback and setting specific SMART objectives. The success of the ACCP implementation is due to a strong partnership between the trainees, clinicians and HEI academic provider alongside support and engagement of the unit. From November 2017, all trainee ACCPs must be undertaking an accredited pathway in order to obtain FICM membership.
The costs of training programme need to be carefully evaluated. As the ACCPs remain supernumerary for the 8 months of the programme, and therefore are not included in the nursing and medical work force numbers but after that time, the ACCPs fill gaps in the rota. At our institution, we chose to train the ACCPs at a Band 7 – reflective of their base line experience and expected responsibilities within the training process and in line with the Agenda for change. The MSc/PG Dip and additional external courses, deemed essential, are funded by the nursing study leave budget.
On completion of the programme in the UK, the cost of an ACCP at band 7 or 8a level may be £30,000–£45,000, the equivalent and in some cases more than a junior doctor (Foundation Year 2 doctor, Specialty Registrar CT1) salary, therefore the concept that ACCPs are an inexpensive workforce solution is misleading. However, compared to use of regular locum medical doctors, they may offer a number of other useful advantages as outlined in Table 6.
General discussion
The model of ACCNPs has been previously reported in US oncology CCUs. D'Agostino et al. faced challenges with recruitment, training, collaborating and communicating but experience at our institution has been positive. 14 This was probably due to early and enthusiastic buy-in from key stakeholders, a comprehensive job description outlining all aspects of the role and expectations, the ability to use the structured FICM ACCP curriculum and the close working relationship between each trainee and their nominated educational supervisor. The ACCP trainees were also able to work on developing their knowledge and skills in a variety of settings outside the CCU including outpatients (for supervised history taking and examination), theatres (basic airway management, central lines, arterial lines), emergency department, the medical assessment unit (venepuncture, PICC line insertion, cannulation) and part of the programme involved rotation to other specialised units (cardiothoracic intensive care, neurointensive care, trauma centres and burns units).
The impact of ACCPs in critical care has been evaluated in a few published studies.15,16 The positive benefits of the ACCPs in critical care have been observed in a prospective cohort study of 9066 admissions with the primary end-point of 90-day survival and secondary end-points of ICU and hospital length of stay. 15 The authors reported no difference in 90-day survival (6.3% vs. 11.6%, adjusted odds ratio 0.77; 95% CI: 0.63–0.94, p = 0.01), hospital mortality or ICU length of stay with the use of ACCPs. Another published study supported the use of NP and Physician's Assistants. 16 In this study, the authors evaluated 21 ICUs and demonstrated similar risk-adjusted mortality between the two groups (adjusted relative risk, 1.10; 95% CI: 0.92–1.31). More studies are required to determine the true impact of the use of ACCPs in critical care.
More recently, an editorial by Lilly and Katz advocated ACCP as part of the ICU staffing following two published studies. 17 Their key message was: ‘The accumulated evidence suggests that properly trained and supervised non-physician prescribing providers can provide high-quality critical care’. However, the authors also drew attention to the need for structured training with adequate senior supervision. Of note in the studies, ACCPs and residents showed no difference in mortality rates and this suggests the role is beneficial.16,17
Assessments provide opportunities for ACCP trainees to demonstrate excellence in their field as outlined. The WPBAs are comprehensive and clearly demonstrate requirements as per the GMC Good Medical Practice. 13 Given that ACCPs are a relatively new concept, it is important that the training record of trainee ACCPs is comprehensively documented for medico-legal reasons. The trainee ACCPs at our institution were able to produce their portfolios demonstrating development of all the required areas. Currently, these are in a paper format and hopefully an e-portfolio will be introduced to allow easier record keeping. Importantly, the WPBAs demonstrate the integration of theory to practice and the application of knowledge and skills. The portfolio assesses knowledge, judgement and practical skills. The FICM document also assesses personal characteristics such as initiative, manner, organisational ability, communication skills and time keeping. Given the intense demands from both educational and clinical perspectives, trainee ACCPs need to have a well-structured teaching programme and adequate time for clinical skills, training, teaching and study days.
In summary, this new advanced practice role offers opportunities to improve continuity of patient care, enhance mentoring and training for less experienced staff, support gaps in the medical workforce as well as offering a rewarding clinical role for senior non-medical staff.
At our institution, we were able to demonstrate successful implementation and integration of the ACCPs in our CCU. The implementation of the ACCP trainee programme is labour intensive and requires significant input from clinicians and academics and not inexpensive, however provided a satisfying and long-term sustainable workforce model for the CCU. The success of the ACCP implementation is due to a strong partnership between the hospital and the university but also buy-in from key stakeholders.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.